




This study examines the relationship between academic performance (Kardex grades) and clinical competence, measured by the Practical Professional Examination (PPT), in medical graduates from the Universidad de Sonora. While academic grades are often used to predict clinical success, their correlation with clinical skills remains uncertain.
MethodsAn observational, retrospective analysis of 358 graduates (2019–2024) was conducted, assessing both final grades and PPT performance. Nine key clinical competencies, including diagnostic reasoning, physical examination, and patient communication, were evaluated. Spearman's correlation was used for non-normal distributions.
ResultsThe mean Kardex grade was 92.76, and the mean PPT score was 87.72. Significant correlations were found between clinical competencies (e.g., differential diagnosis and physical examination) and PPT performance, with the strongest correlation in differential diagnosis (r = 0.777, p < 0.001). However, the correlation between Kardex grades and PPT performance was weak (r = 0.152, p = 0.004), suggesting that academic grades do not reliably predict clinical competence.
ConclusionFindings indicate that strong academic performance does not guarantee clinical skills. Essential competencies, such as diagnostic reasoning, are crucial in clinical assessments. Medical education should integrate theoretical knowledge with hands-on practice through strategies like problem-based learning (PBL) and Objective Structured Clinical Examinations (OSCE). While academic performance reflects theoretical knowledge, it is not a strong predictor of clinical competence. Enhancing the integration of theory and practice is essential to better prepare graduates for real-world clinical settings.
Este estudio examina la relación entre el rendimiento académico (calificaciones Kardex) y la competencia clínica, medida a través del Examen Profesional Práctico (PPT), en egresados de Medicina de la Universidad de Sonora. Aunque las calificaciones académicas suelen utilizarse para predecir el éxito clínico, su correlación con las habilidades clínicas sigue siendo incierta.
MétodosSe realizó un análisis observacional y retrospectivo de 358 egresados (2019–2024), evaluando tanto las calificaciones finales como el desempeño en el PPT. Se evaluaron nueve competencias clínicas clave, incluyendo el razonamiento diagnóstico, el examen físico y la comunicación con el paciente. Se utilizó la correlación de Spearman para distribuciones no normales.
ResultadosLa calificación promedio del Kardex fue de 92.76, y la puntuación promedio del PPT fue de 87.72. Se encontraron correlaciones significativas entre las competencias clínicas (por ejemplo, diagnóstico diferencial y examen físico) y el desempeño en el PPT, siendo la correlación más fuerte en el diagnóstico diferencial (r = 0.777, p < 0.001). Sin embargo, la correlación entre las calificaciones del Kardex y el desempeño en el PPT fue débil (r = 0.152, p = 0.004), lo que sugiere que las calificaciones académicas no predicen de manera confiable la competencia clínica.
ConclusiónLos resultados indican que un buen rendimiento académico no garantiza habilidades clínicas. Competencias esenciales, como el razonamiento diagnóstico, son cruciales en las evaluaciones clínicas. La educación médica debe integrar el conocimiento teórico con la práctica mediante estrategias como el aprendizaje basado en problemas (PBL) y los Exámenes Clínicos Estructurados Objetivos (OSCE). Aunque el rendimiento académico refleja el conocimiento teórico, no es un predictor fuerte de la competencia clínica. Mejorar la integración de la teoría y la práctica es esencial para preparar mejor a los egresados para los entornos clínicos del mundo real.
The assessment of academic and clinical performance in the training of healthcare professionals is an essential component to ensure that graduates possess the necessary competencies for professional practice. In medical education, this evaluation process is complex and multifaceted, integrating both theoretical knowledge and practical skills to ensure high-quality patient care.1 Among the assessment methods used, the Practical Professional Examination (PPT) has become a key requirement for graduation in various medical education institutions in Mexico, as it evaluates clinical competence through predefined and standardized rubrics.2
In this text, academic performance is defined by the authors as the level of achievement attained by a student in relation to established learning objectives, measured through grades, assessments, and other educational indicators. This definition, proposed specifically for the purposes of this study, not only refers to the mastery of theoretical knowledge but also includes the development of practical and attitudinal skills necessary for competent professional practice.3 In medical training, academic performance is evaluated through written exams, practical activities, and participation in clinical settings, reflecting the student's level of preparedness to face the challenges of professional practice.4
The relationship between academic performance during medical school and outcomes in practical assessments such as the PPT has been a subject of debate in the medical education literature. While some studies suggest a positive correlation between these aspects,4 others indicate that theoretical knowledge does not always translate into strong clinical skills due to variability in teaching and assessment methodologies.5 This discrepancy raises questions about the effectiveness of current pedagogical strategies and the relevance of using academic grades as predictors of clinical performance.
Several factors may influence this relationship, including learning style, opportunities for clinical practice, and exposure to real healthcare settings.6 Specifically, key competencies such as diagnostic reasoning, physical examination, and effective patient communication have been shown to be determinants of final clinical performance.1 However, the lack of a strong correlation between final grades and PPT outcomes7 suggests the need for a comprehensive evaluation approach that considers both theoretical knowledge and practical skill development from the early stages of medical training.
Therefore, this study aims to determine the relationship between the final grade of graduates from the Bachelor of Medicine program at the Universidad de Sonora and their performance in the PPT. For the purposes of this study, academic performance will be defined as the final grade obtained by students upon completing their medical studies. The findings of this research will help determine whether academic performance can be considered a reliable predictor of clinical competence and, consequently, guide the implementation of educational strategies that strengthen the integration of theoretical and practical aspects in medical training.
Materials and methodsThis study employed an observational, retrospective, and correlational design to analyze the relationship between the final Kardex grade of Bachelor of Medicine students at a university in northwestern Mexico and their performance in the PPT. Kardex is understood as the official document that summarizes a student's academic performance. Data were collected from academic records and official evaluation reports corresponding to PPTs conducted between 2019 and 2024, allowing for a detailed analysis of the study variables.
The study population included graduates from the Bachelor of Medicine program at a university in northwestern Mexico who took the PPT as part of the graduation requirements between 2019 and 2024.
The sample was selected based on specific criteria, including graduates who took the PPT before faculty members of the university and whose records contained complete information on both their final grade and their PPT performance. Records with missing data in any of the variables of interest and those presenting inconsistencies, such as duplicate grades or transcription errors, were excluded.
The PPT assessment instrument consists of nine items that measure the key competencies of a competent physician. These variables include (The value of each item on a base scale of 100 is specified in parentheses):
- •
Professional presentation and respect for the patient (5)
- •
Active listening and patient-centered attention (5)
- •
Appropriate history-taking (10)
- •
Physical examination focused on the patient's condition (20)
- •
Identification and interpretation of complementary studies (15)
- •
Establishment of differential diagnoses (20)
- •
Knowledge of treatment options and alternatives (15)
- •
Confidence in communication and subject matter expertise (5)
- •
Patient and family communication regarding the condition (5)
This instrument was validated by expert judgment and demonstrated a reliability of 0.803 according to Cronbach's alpha.
- 1.
Data Collection
- ○
Data collection was based on two official information sources. First, the institutional academic database was used to obtain the final grade of each graduate from the institution's administrative records. Second, the official PPT rubric was employed, detailing student performance in each of the previously described variables, as well as the overall PPT score.
- ○
- 2.
Data Analysis
- ○
Data analysis was conducted using Statistical Package for Social Sciences (SPSS), version 26.0.0, at three levels:
- ○
- 3.
Descriptive analysis:
- ○
Mean values, standard deviations, and distributions of final grades and PPT scores were calculated.
- ○
- 4.
Normality test:
- ○
The Kolmogorov–Smirnov test for a single sample was applied to assess the normality of the distributions of final grades and PPT scores.
- ○
- 5.
Correlation tests:
- ○
Based on the normality test results, Pearson's correlation was applied for normal distributions and Spearman's correlation for non-normal distributions to determine the relationship between the final grade and the PPT outcome. A correlation coefficient (r) was established with a 95% confidence level (p < 0.05).
- ○
Since this study utilized pre-existing databases without direct contact with human subjects, approval from an ethics committee was not required. However, data were handled anonymously and confidentially in compliance with current data protection regulations in Mexico.
ResultsDescriptive Results.
The study included 358 participants, of whom 60.9% were women and 39.1% were men. The nine PPT variables were evaluated, yielding mean values and standard deviations that reflect participant performance in different areas (Table 1). The mean score for Professional presentation and respect for the patient was 97.82 (SD = 7.54), while Active listening and patient-centered attention had a mean score of 98.16 (SD = 7.63). The ability to conduct an Appropriate history-taking showed a mean of 85.34 (SD = 16.46), and Physical examination focused on the patient's condition had a mean of 82.91 (SD = 16.43).
Descriptive Statistics of the Study.
| Mean | Standard deviation | |
|---|---|---|
| Professional presentation and respect for the patient | 97.82 | 7.541 |
| Active listening and patient-centered attention | 98.16 | 7.630 |
| Appropriate history-taking | 85.34 | 16.459 |
| Physical examination focused on the patient's condition | 82.91 | 16.431 |
| Identification and interpretation of complementary studies | 89.34 | 14.490 |
| Establishment of differential diagnoses | 86.34 | 15.091 |
| Knowledge of treatment options and alternatives | 87.5233 | 15.86627 |
| Confidence in communication and subject matter expertise | 85.00 | 17.549 |
| Patient and family communication regarding the condition | 93.46 | 13.832 |
| PPT score | 87.7151 | 10.35334 |
| Final Kardex grade | 92.7574 | 2.76246 |
For Identification and interpretation of complementary studies, the mean score was 89.34 (SD = 14.49), while the Establishment of differential diagnoses had a mean of 86.34 (SD = 15.09). Regarding Knowledge of treatment options and alternatives, a mean of 87.52 (SD = 15.86) was obtained, whereas Confidence in communication and subject matter expertise showed a mean of 85.00 (SD = 17.55). Finally, Patient and family communication regarding the condition had a mean score of 93.46 (SD = 13.83).
Additionally, grades obtained in the PPT were compared with those recorded in the academic transcript (Kardex). The mean PPT score was 87.72 (SD = 10.35), ranging from 60.00 to 100.00, while the mean Kardex grade was 92.76 (SD = 2.76), with a range of 80.35 to 97.24.
Normality Test.
To assess data distribution, the Kolmogorov–Smirnov test was applied to each analyzed variable. Results indicated that none of the variables followed a normal distribution, as all cases yielded a two-tailed asymptotic significance value below.001 (p < 0.05).
Both PPT scores (Mean = 87.72, SD = 10.35) and Kardex grades (Mean = 92.76, SD = 2.76) showed a non-normal distribution. Similarly, clinical competence scores had significance values below 0.05, suggesting an asymmetric data distribution.
Since the results did not meet the normality assumption, the use of non-parametric statistical tests in subsequent analyses was considered appropriate to ensure the validity of comparisons and inferences in this study.
Comparative analysisCorrelation Between Clinical Skills and PPT Scores.
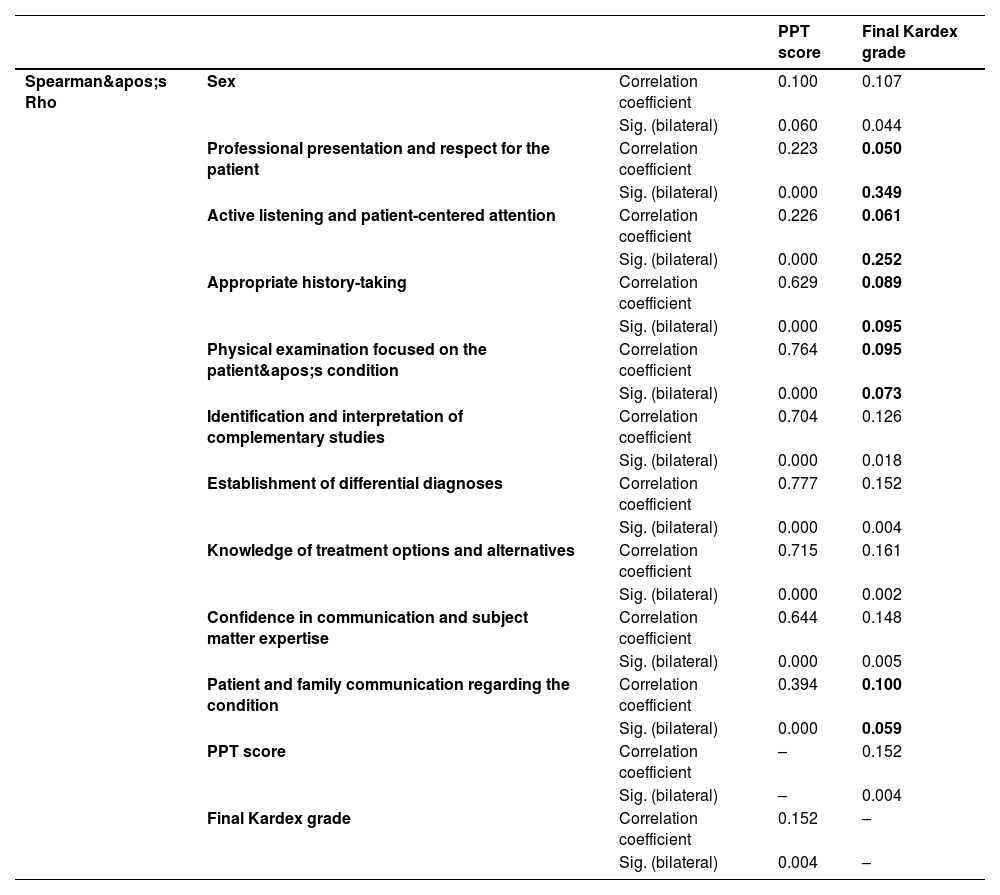
Spearman's correlation analysis revealed significant relationships between evaluated clinical skills and PPT scores (Table 2). This finding was expected, as the assessed competencies directly align with the criteria in the evaluation checklist used for practical assessment. Therefore, the observed correlations reflect consistency between the clinical aspects evaluated and the final PPT outcome.
Spearman's Correlation of Items Evaluated by the Practical Professional Exam Against Final Kardex Grade. (Data with no correlation are highlighted).
| PPT score | Final Kardex grade | |||
|---|---|---|---|---|
| Spearman's Rho | Sex | Correlation coefficient | 0.100 | 0.107 |
| Sig. (bilateral) | 0.060 | 0.044 | ||
| Professional presentation and respect for the patient | Correlation coefficient | 0.223 | 0.050 | |
| Sig. (bilateral) | 0.000 | 0.349 | ||
| Active listening and patient-centered attention | Correlation coefficient | 0.226 | 0.061 | |
| Sig. (bilateral) | 0.000 | 0.252 | ||
| Appropriate history-taking | Correlation coefficient | 0.629 | 0.089 | |
| Sig. (bilateral) | 0.000 | 0.095 | ||
| Physical examination focused on the patient's condition | Correlation coefficient | 0.764 | 0.095 | |
| Sig. (bilateral) | 0.000 | 0.073 | ||
| Identification and interpretation of complementary studies | Correlation coefficient | 0.704 | 0.126 | |
| Sig. (bilateral) | 0.000 | 0.018 | ||
| Establishment of differential diagnoses | Correlation coefficient | 0.777 | 0.152 | |
| Sig. (bilateral) | 0.000 | 0.004 | ||
| Knowledge of treatment options and alternatives | Correlation coefficient | 0.715 | 0.161 | |
| Sig. (bilateral) | 0.000 | 0.002 | ||
| Confidence in communication and subject matter expertise | Correlation coefficient | 0.644 | 0.148 | |
| Sig. (bilateral) | 0.000 | 0.005 | ||
| Patient and family communication regarding the condition | Correlation coefficient | 0.394 | 0.100 | |
| Sig. (bilateral) | 0.000 | 0.059 | ||
| PPT score | Correlation coefficient | – | 0.152 | |
| Sig. (bilateral) | – | 0.004 | ||
| Final Kardex grade | Correlation coefficient | 0.152 | – | |
| Sig. (bilateral) | 0.004 | – | ||
The highest correlations were observed in fundamental aspects of clinical reasoning and decision-making, which are central elements in the practical examination. For instance, Establishment of differential diagnoses showed the highest correlation (r = 0.777, p < 0.001). Similarly, Physical examination focused on the patient's condition presented a high correlation (r = 0.764), highlighting this skill as essential in clinical performance assessment.
Other skills such as Identification and interpretation of complementary studies (r = 0.704, p < 0.001) and Knowledge of treatment options and alternatives (r = 0.715, p < 0.001) also demonstrated strong correlations. This is logical since these competencies are explicitly measured and weighted in the evaluation rubric. Consequently, students who scored higher in these areas obtained better overall PPT scores.
Even communication skills, such as Patient and family communication regarding the condition, showed significant correlations (r = 0.394, p < 0.001), reinforcing the notion that these competencies were actively evaluated during the practical assessment. On the other hand, basic professional skills, such as Professional presentation and respect for the patient, exhibited lower but still significant correlations (r = 0.223 and r = 0.226, p < 0.001). This is likely because, although these skills are important, their weighting in the PPT is lower compared to more technical or analytical competencies.
Correlation Between Clinical Skills and Final Kardex Grades.
Spearman's correlation analysis identified significant correlations between some clinical skills and Kardex grades. However, specific competencies demonstrated a stronger relationship with academic performance, suggesting that certain aspects of clinical training influence the grades obtained throughout medical school.
Among the competencies with the highest correlations with Kardex grades was Knowledge of treatment options and alternatives, which showed a correlation of r = 0.161, p = 0.002. This indicates that students with greater mastery in this area tended to achieve higher academic scores. Similarly, establishment of differential diagnoses presented a correlation of r = 0.152, p = 0.004, suggesting that proficiency in diagnostic reasoning was reflected in academic performance.
Furthermore, Confidence in communication and subject matter expertise showed a significant correlation (r = 0.148, p = 0.005), implying that students who demonstrated greater confidence in their knowledge achieved higher Kardex grades. In contrast, Identification and interpretation of complementary studies presented a weaker but statistically significant correlation (r = 0.126, p = 0.018), indicating that this skill had a modest relationship with academic performance.
On the other hand, some clinical competencies, such as Physical examination focused on the patient's condition, Appropriate history-taking, and Patient and family communication regarding the condition, did not show significant correlations with Kardex grades. These findings suggest that these skills were not directly reflected in the academic grading system, or their evaluation was influenced by other unconsidered factors in this analysis, such as the subjectivity of evaluation depending on the teaching criteria or the type of patient assigned to the student.
Correlation Between PPT Scores and Final Kardex Grades.
Spearman's correlation analysis revealed a significant relationship between PPT scores and Kardex grades (r = 0.152, p = 0.004). Although the correlation magnitude was low, its statistical significance suggests that there is a relationship between cumulative academic performance throughout medical school and final assessment results.
DiscussionThe findings of the present study show a significant relationship between the clinical competencies assessed in the Practical Performance Exam (PPT) and the academic performance recorded in the academic history. However, the magnitude of the correlations suggests that performance in the practical evaluation does not always reflect academic performance proportionally, which is consistent with recent studies that have identified discrepancies between theoretical grades and performance in clinical assessments.8 This statement is evidenced by reviewing the specific relationships of each item, where some elements that could be considered essential in medical competencies do not have much correlation with academic history.
These results suggest that strong theoretical performance throughout the course does not necessarily guarantee a high score in the professional exam, highlighting the importance of strengthening the integration between theoretical training and practical preparation. Furthermore, the incorporation of teaching methodologies based on problem-based learning (PBL) and evaluation through Objective Structured Clinical Examinations (OSCE) may help bridge the gap between theoretical knowledge and its application in the clinical context.9 PBL is a student-centered approach where learning occurs through the analysis of clinical cases, fostering critical thinking and the integration of theory with practice. It promotes active learning and enhances clinical reasoning skills.10
One of the most relevant findings of the study is the high correlation between essential clinical reasoning competencies and the score obtained in the PPT. In particular, the ability to establish a differential diagnosis (r = 0.777, p < 0.001) and perform a physical examination focused on the presenting complaint (r = 0.764, p < 0.001) stand out as key skills in clinical performance. These results support previous evidence4 that underscores the importance of these competencies in medical practice and their impact on final evaluations. Additionally, the interpretation of diagnostic studies and knowledge of appropriate treatment also showed high correlations with the exam score, further reinforcing their relevance in the assessment of clinical competencies.11
On the other hand, competencies related to communication with the patient and family regarding the illness showed significant correlations (r = 0.394, p < 0.001), although lower compared to technical skills. This trend is consistent with previous studies that have identified a lower weight of communicative skills in clinical performance evaluation, despite their importance for professional practice.12 Nevertheless, beyond their lower weighting in clinical evaluations, factors such as limited assessment time, subjective scoring of interpersonal interactions, and a predominant focus on technical skills may also contribute to the lower correlation observed.
Regarding academic performance reflected in the Kardex and the clinical competencies assessed, the correlation coefficients were low, although significant in key skills such as knowledge of treatment and alternatives (r = 0.161, p = 0.002) and the ability to establish a differential diagnosis (r = 0.152, p = 0.004). These results suggest that, while academic performance may reflect certain theoretical knowledge, it does not necessarily predict the practical application of this knowledge, as documented in previous research on medical education.12
In general terms, the findings indicate that, while some clinical skills showed a relationship with the academic performance recorded in the Kardex, this relationship was weaker compared to that observed in the professional exam. This could be related to the grading structure in the Kardex, which likely reflected theoretical performance and continuous evaluation to a greater extent, rather than the practical development of fundamental clinical competencies for medical practice.
Finally, the weak correlation between the PPT score and the Kardex score (r = 0.152, p = 0.004) indicates that, while a significant relationship exists, accumulated academic performance throughout university training is not a direct predictor of final clinical performance. This reinforces the need to design comprehensive evaluation strategies that combine both theoretical knowledge and practical competence. For this, it is essential to incorporate teaching methodologies based on clinical simulations, competency-based evaluation, and structured feedback. Additionally, integrating early practices in real clinical environments could contribute to better preparation for students, ensuring that their academic training more accurately reflects the skills necessary for professional practice.
It is also important to consider that, despite assessing clinical competencies, the PPT may not fully reflect students' actual practical skills. As a standardized examination, it often emphasizes adherence to predefined checklists rather than evaluating real-world performance. Therefore, its results might indicate students' ability to meet exam-specific criteria rather than providing an infallible measure of their overall clinical competence. Recognizing this limitation is essential when interpreting outcomes and designing strategies for comprehensive skills development.
In conclusion, the results highlight the importance of reinforcing the teaching and assessment of clinical competencies from a comprehensive approach, balancing theory and practice. To achieve this integration, it is recommended to implement strategies such as clinical simulations, interactive case studies, and supervised clinical rotations from the early stages of training. Future research could focus on analyzing the effectiveness of different pedagogical strategies and their impact on professional performance to optimize medical training and ensure a higher level of preparedness in graduates.
FundingNo specific funding.
The authors declare that there are no financial, personal, or institutional conflicts of interest that could have influenced the conduct of this research. This study was developed independently, without external funding from private or governmental entities that could compromise the objectivity of the findings. Furthermore, it is assured that the data have been analyzed impartially, and the conclusions strictly reflect the results obtained.
None.



