




To evaluate the relation between the coronary calcium score and the posterior choice of kilovoltage according to radiologists’ criteria in a standard coronary CT angiography protocol to rule out coronary disease.
To quantify the reduction in ionizing radiation after linking kilovoltage to patients’ body mass index in a low-dose protocol with iterative model reconstruction.
To evaluate the image quality and diagnostic performance of the low-dose protocol.
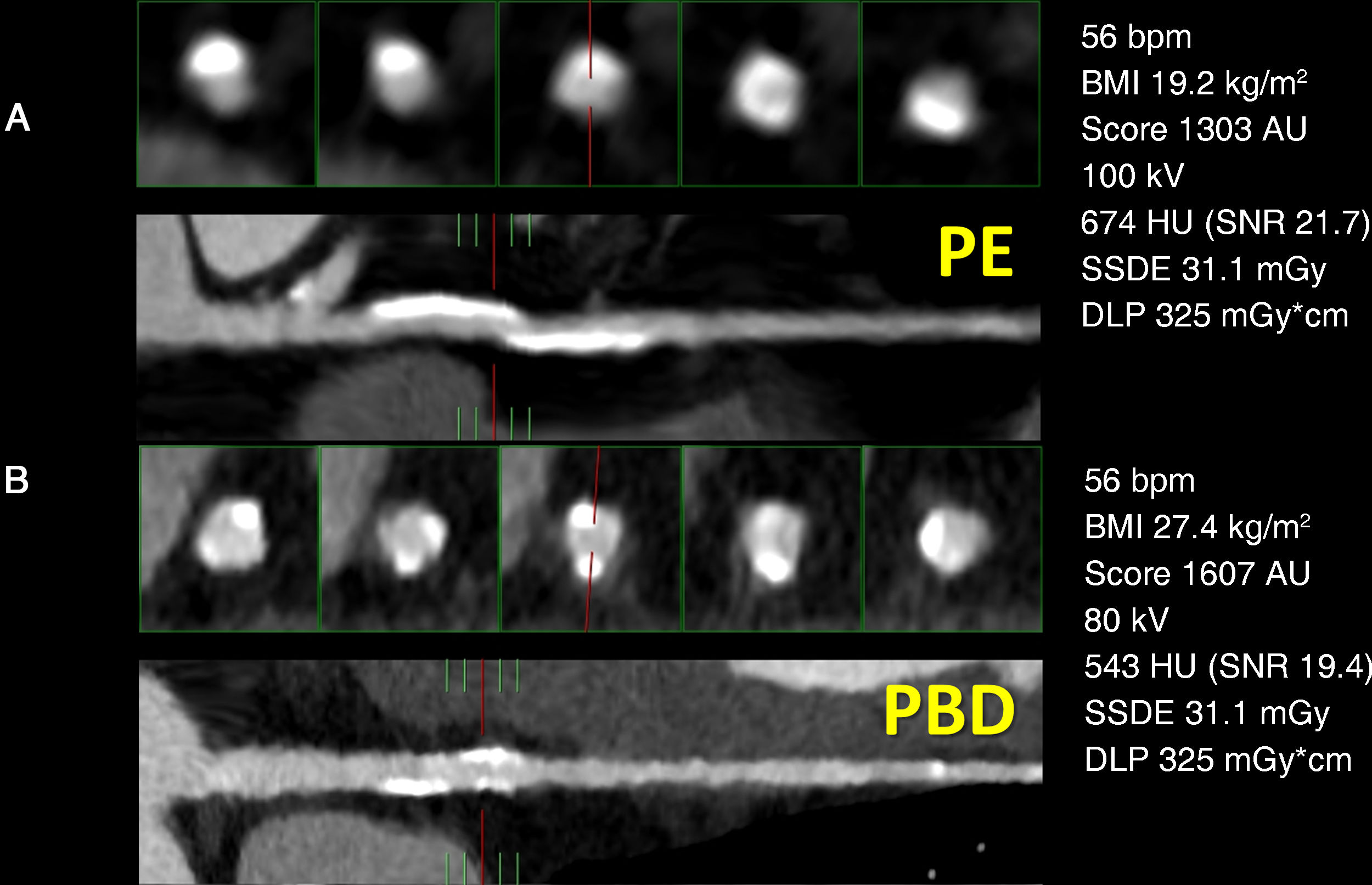
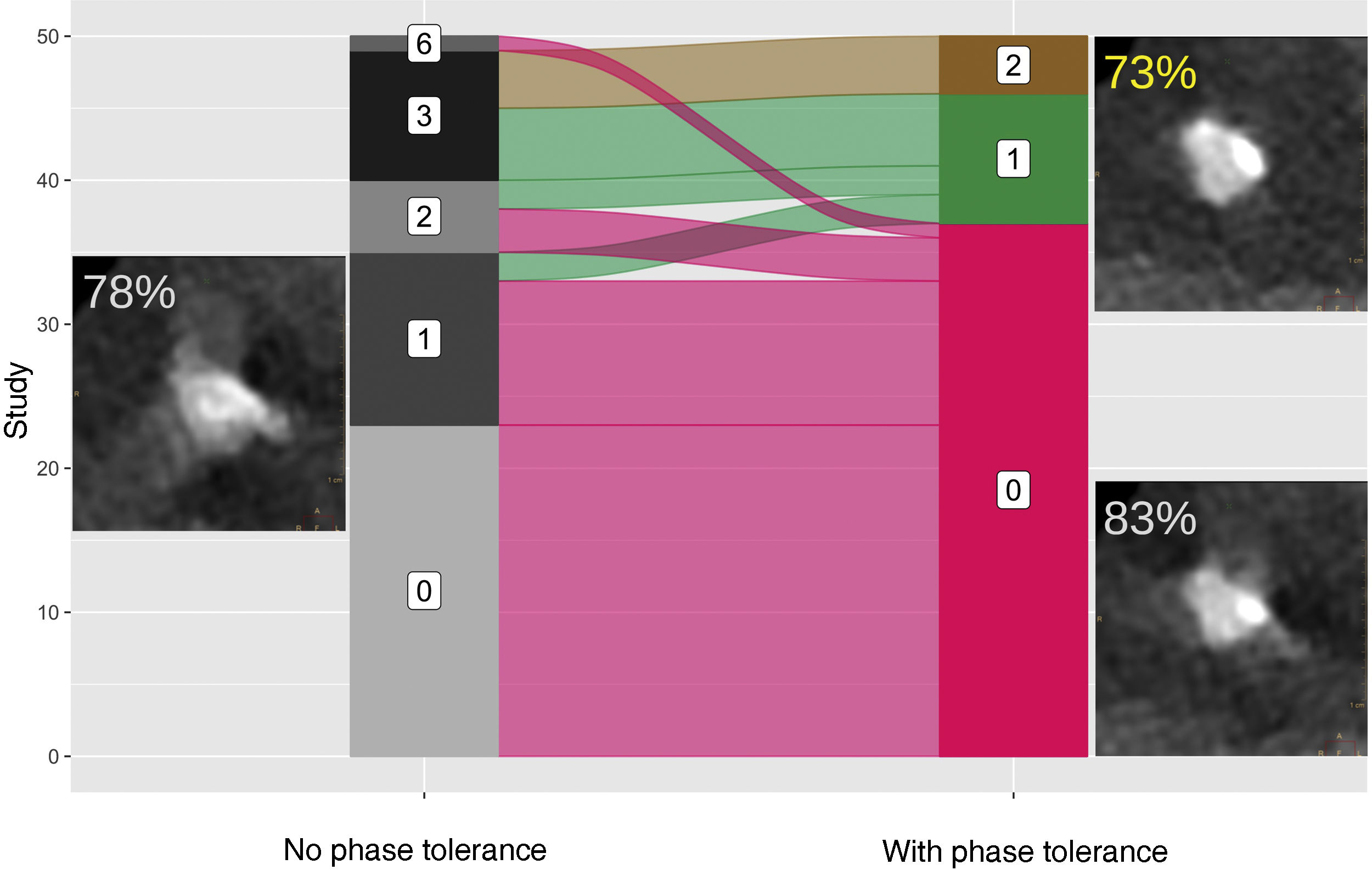
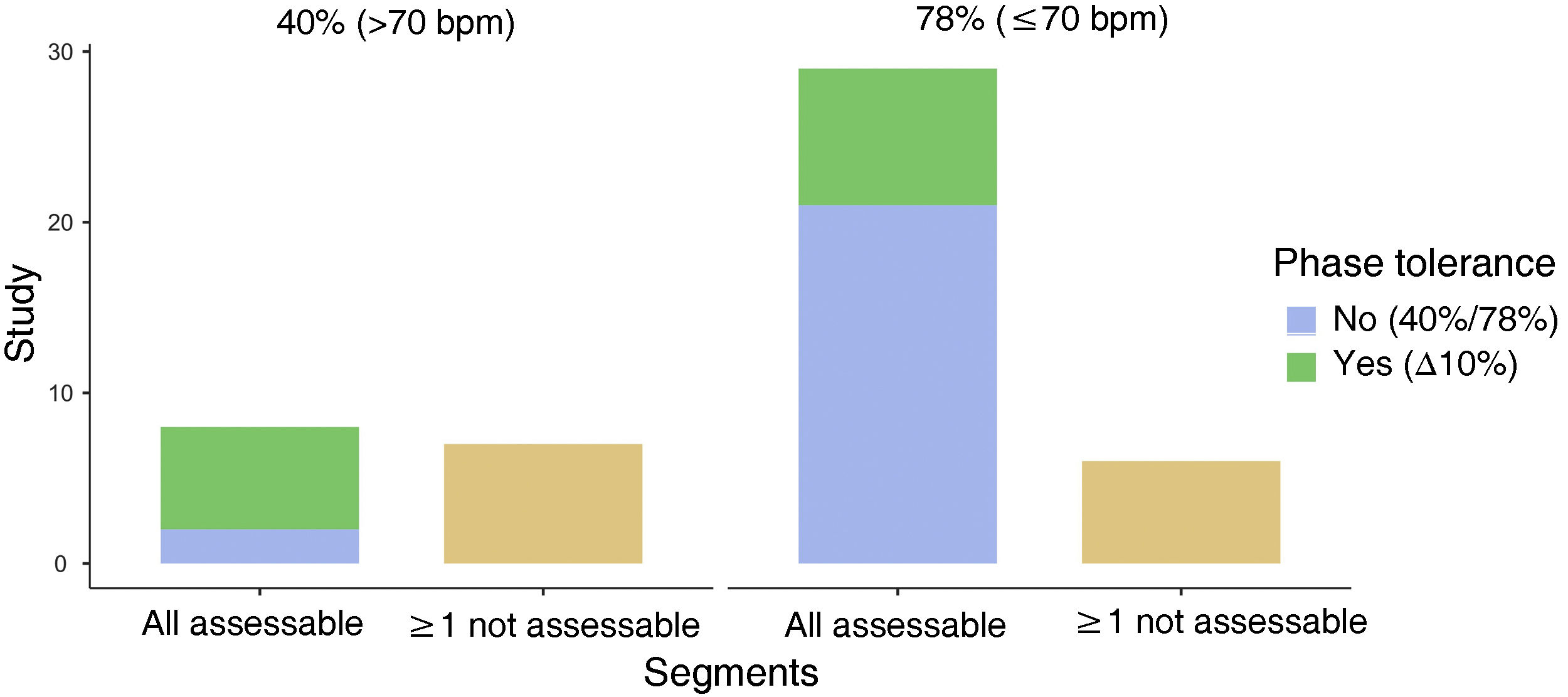
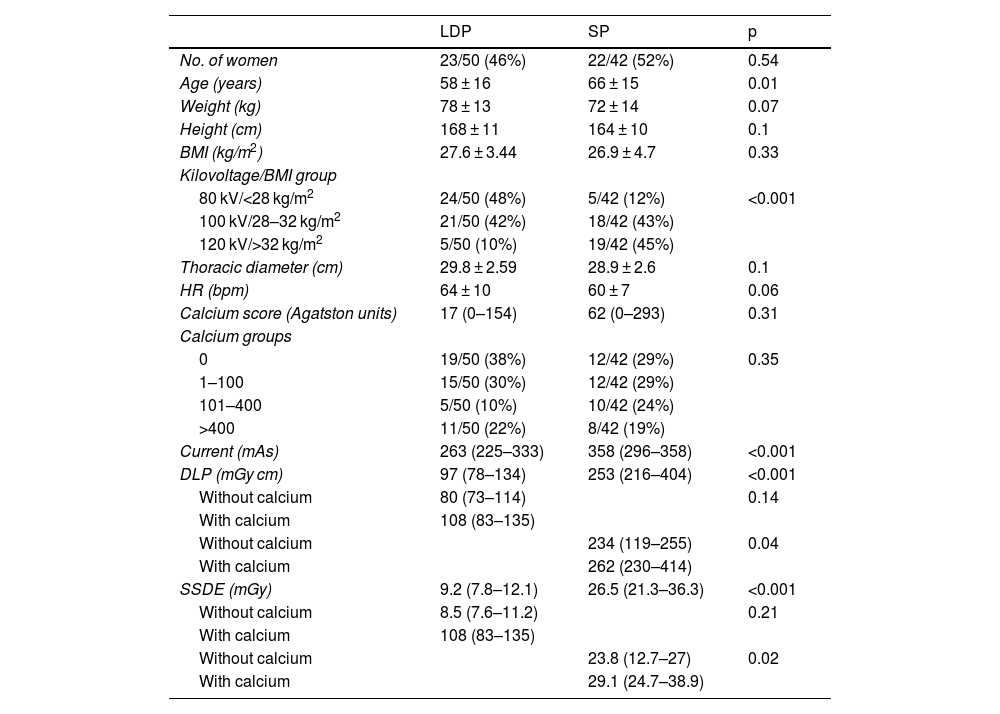
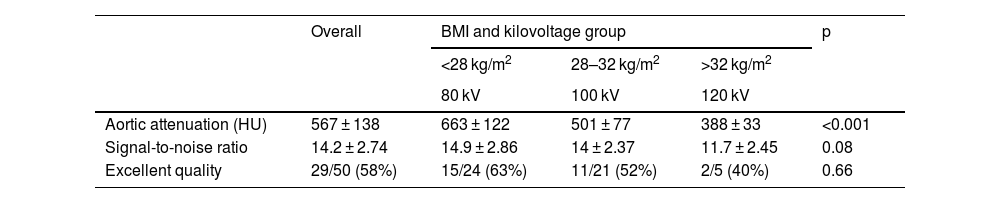
Material and methodsWe compared anthropometric characteristics, calcium score, kilovoltage levels, size-specific dose estimates (SSDE), and the dose-length product (DLP) between a group of 50 patients who were prospectively recruited to undergo coronary CT angiography with a low-dose protocol and a historical group of 50 patients who underwent coronary CT angiography with the standard protocol. We correlated these parameters, the number of coronary segments that could not be evaluated with and without temporal padding, the attenuation, and the signal-to-noise ratio in the ascending aorta in the low-dose protocol with excellent imaging quality according to a semiquantitative scale. To calculate the diagnostic performance per patient, we used 24-month clinical follow-up including all tests as the gold standard.
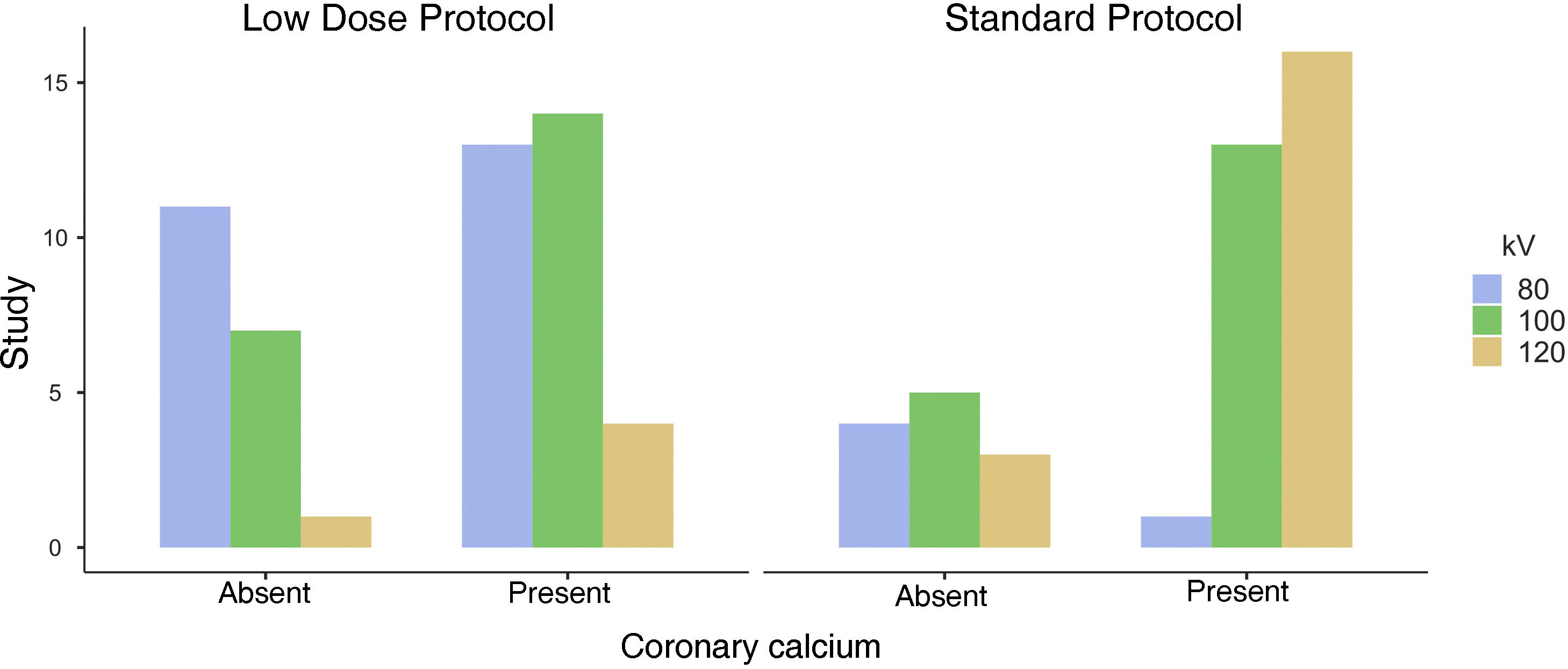
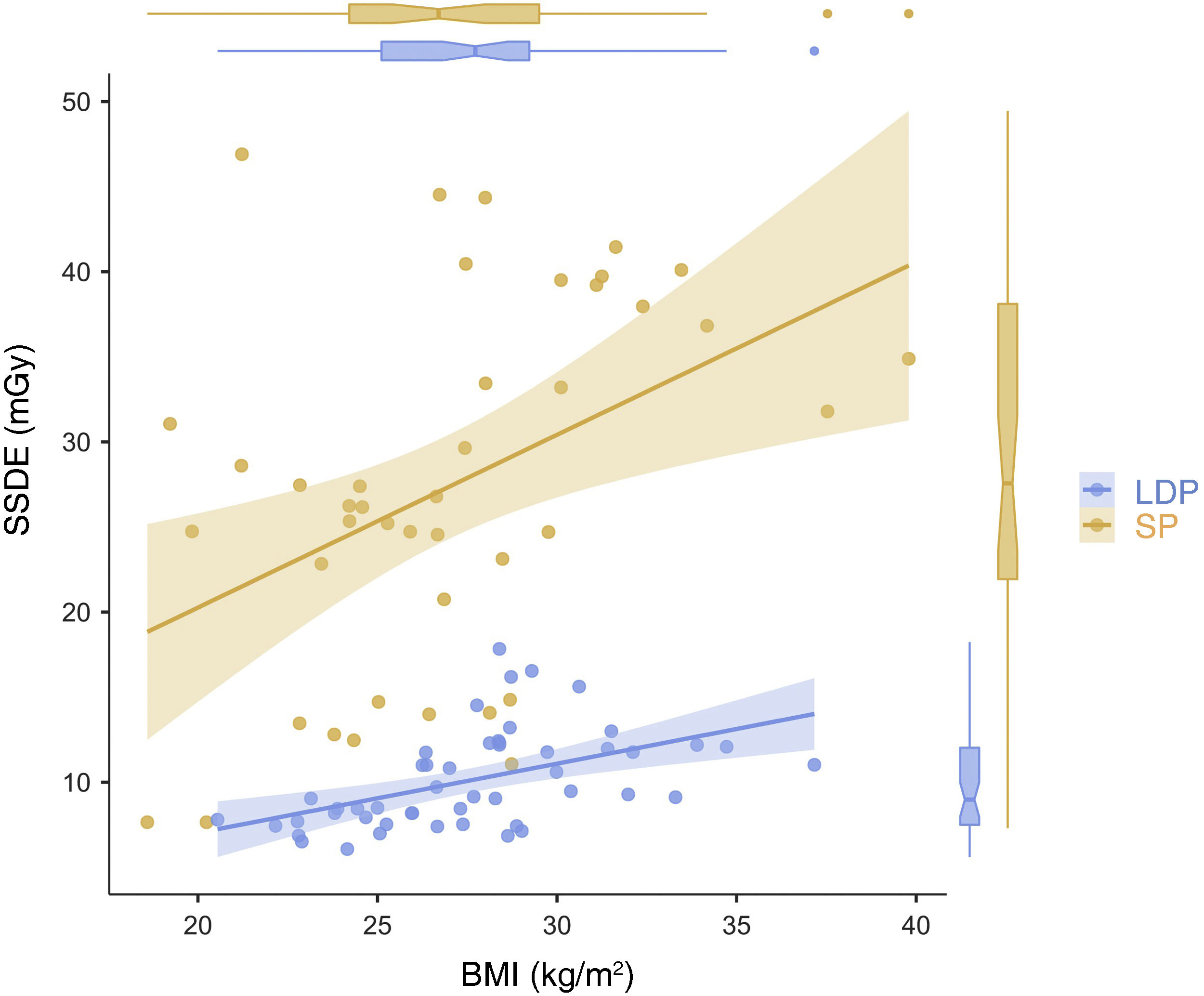
ResultsIn the standard protocol, the presence of coronary calcium correlated with the selection of high kilovoltage (p = 0.02); this correlation was not found in the low-dose protocol (p = 0.47). Median values of SSDE and DLP were significantly (p < 0.001) lower and less dispersed in the low-dose protocol [9.22 mGy (IQR 7.84–12.1 mGy) vs. 26.5 mGy (IQR 21.3–36.3 mGy) in the standard protocol] and [97 mGy cm (IQR 78–134 mGy cm) vs. 253 mGy cm (IQR 216–404 mGy cm) in the standard protocol], respectively.
The overall quality of the images obtained with the low-dose protocol was considered good or excellent in 96% of the studies. The parameters associated with image quality in a multivariable model (C statistic = 0.792) were heart rate (estimated coefficient, −0,12 [95% confidence interval: −0.2, −0.04]; p < 0.01) and the SSDE (estimated coefficient, −0,26 [95% confidence interval: −0.51, −0.01]; p < 0.05).
The CAD-RADS modifier for a not fully evaluable or diagnostic study was used on two occasions (4%); the final measures for the diagnosis of coronary disease were sensitivity 100%, specificity 94%, and efficacy 94%.
ConclusionsIn the standard protocol, the radiologist selects higher kilovoltage for CT angiography studies for patients whose previous calcium score indicates the presence of coronary calcium. In the low-dose protocol, linking kilovoltage with body mass index enables the dose of radiation to be reduced by 65% while obtaining excellent or good image quality in 96% of studies and excellent diagnostic performance.
Valorar la relación entre el score de calcio coronario y la elección posterior del kilovoltaje según el criterio del radiólogo en un protocolo estándar (PE) de angio-TC coronaria (aTCC) para descartar enfermedad coronaria.
Cuantificar la reducción de la radiación ionizante después de vincular el kilovoltaje al índice de masa corporal en un protocolo de baja dosis (PBD) con reconstrucción iterativa de modelado.
Valorar la calidad de imagen y el rendimiento diagnóstico del PBD.
Material y métodoLas características antropométricas, el score de calcio, los niveles de kilovoltaje y los valores de dosis estimada específica para el tamaño (SSDE) y del producto dosis-longitud fueron comparados entre un grupo de 50 pacientes con PBD reclutados prospectivamente y una cohorte histórica adquirida con el PE. Estos parámetros, el número de segmentos coronarios no valorables sin y con tolerancia de fase, la atenuación y la relación señal-ruido en la aorta ascendente en el PBD fueron correlacionados con una calidad de imagen de nivel excelente según una escala semicuantitativa. El rendimiento diagnóstico por paciente fue calculado usando la revaloración clínica a los 24 meses como el método diagnóstico de referencia, incluyendo las pruebas derivadas.
ResultadosEn el PE existía una relación entre la presencia de calcio coronario y la elección de kilovoltajes altos (p = 0,02), que desaparecía en el PBD (p = 0,47). Los valores de SSDE y de DLP en el PBD fueron significativamente inferiores y presentaron menor dispersión que en el PE (9,22 mGy [RIQ 7,84-12,1 mGy] y 97 mGy*cm [RIQ 78-134 mGy*cm] contra 26,5 mGy [RIQ 21,3-36,3 mGy] y 253 mGy*cm [RIQ 216-404 mGy*cm]; p < 0,001 para las comparaciones de las medianas y de las dispersiones entre ambos grupos).
La calidad global del PBD fue considerada buena o excelente en un 96% de los estudios y los parámetros que mostraron relación con esta última en un modelo multivariable (estadístico C = 0,792) fueron la frecuencia cardíaca (coeficiente estimado –0,12 [intervalo de confianza del 95%: –0,2, –0,04; p < 0,01) y la SSDE (coeficiente estimado –0,26 [intervalo de confianza del 95%: –0,51, –0,01]; p < 0,05).
El modificador CAD-RADS para un estudio no completamente diagnóstico fue usado en 2 ocasiones (4%), con una sensibilidad, una especificidad y una eficacia finales para el diagnóstico de enfermedad coronaria del 100, el 94% y el 94%, respectivamente.
ConclusionesEn el PE, el radiólogo elegía kilovoltajes más altos para la adquisición de la aTCC ante la presencia de calcio coronario en el score de calcio previo. La vinculación del kilovoltaje al índice de masa corporal en el PBD permitió reducir un 65% la dosis de radiación, con una calidad global excelente o buena en un 96% de los estudios y un rendimiento diagnóstico excelente.

