






This scoping systematic review aimed to collate and synthesize available evidence on research ethics and consent aspects related to research integrity standards in RCTs. Prospective registration (https://osf.io/gxryb).
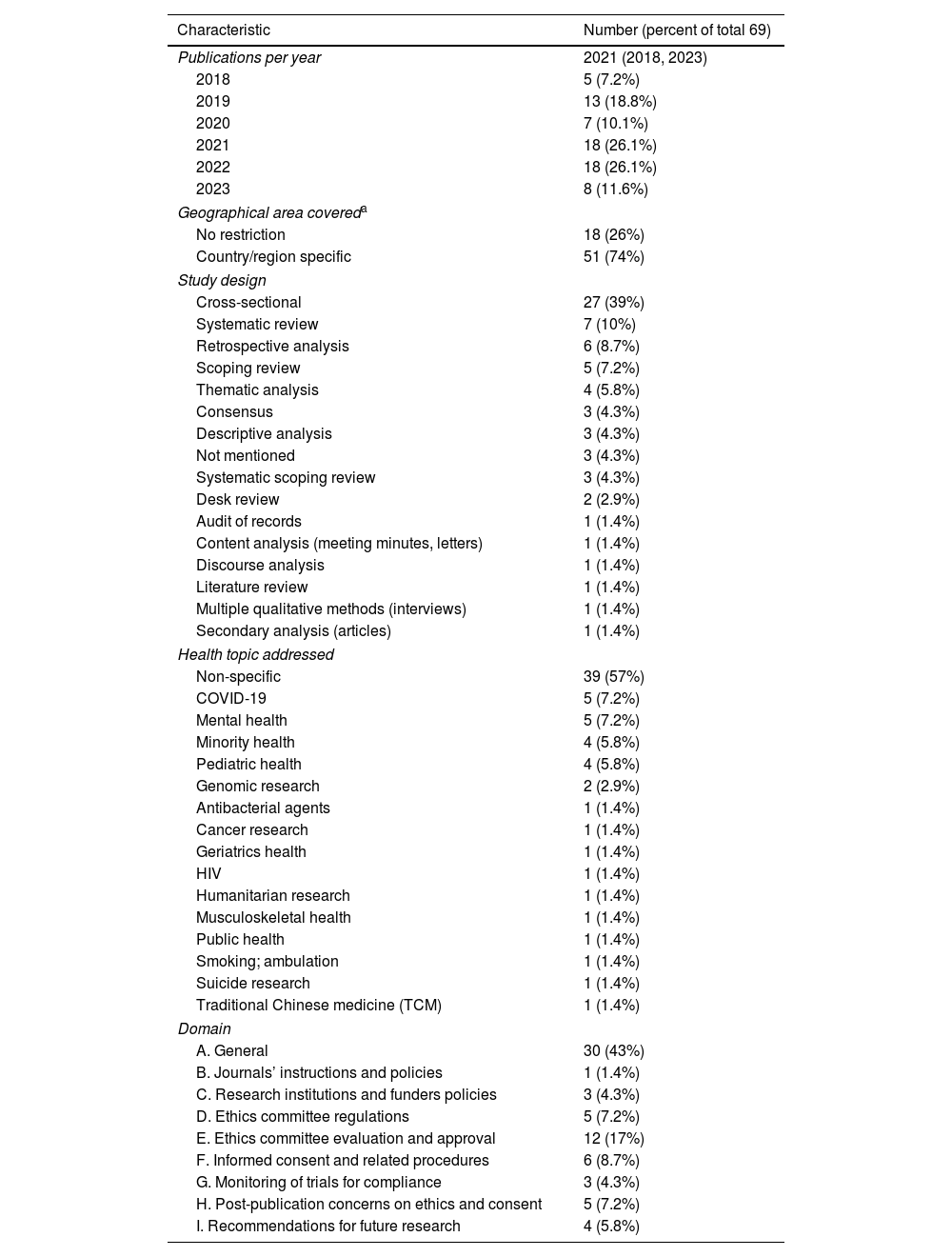
Materials and methodsWe searched PubMed and Scopus databases from January 2018 to August 2023, using combinations of terms related to research ethics, approval, and informed consent. We included full academic articles relevant to the scope of the review without language restriction, including primary research articles, systematic reviews, scoping reviews, and narrative reviews. Two teams of four reviewers independently assessed the full text to select articles and extract data, performing the tasks independently and any disagreements were resolved through arbitration. A descriptive synthesis of the included articles main characteristics and findings were performed.
ResultsSixty-nine articles were selected, covering RCT-related ethics and consent issues in 141 countries, including 89 (63%) low or middle-income ones. The extracted data fell into nine domains: general issues (30 articles; 43%), journals’ instructions and policies (one article; 1.4%), research institutions and funders’ policies (three articles; 4.3%), ethics committee regulations (five articles; 7.2%), ethics committee evaluation and approval (12 articles; 17%), informed consent and related procedures (six articles; 8.7%), monitoring of trials for compliance (three articles; 4.3%), post-publication concerns on ethics and consent (five articles; 7.2%), and recommendations for future research (four articles; 5.8%).
ConclusionsThe key areas include standardization of ethics committee approval processes and enhancement of informed consent procedures. There were notable deficiencies in trial registration and reporting concerning ethics and consent. The observed variability in ethics and consent practices across RCTs globally needs to be addressed through an international expert consensus.
Esta revisión sistemática tuvo como objetivo recopilar y sintetizar la evidencia disponible sobre la relación entre los aspectos éticos de la investigación y las condiciones del consentimiento informado con los estándares de integridad de la investigación en ECA.
Materiales y métodosTras el registro del protocolo (https://osf.io/gxryb), se realizaron búsquedas en las bases de datos PubMed y Scopus desde enero de 2018 hasta agosto de 2023, utilizando combinaciones de términos relacionados con la ética de la investigación, la aprobación y el consentimiento informado. Se incluyeron artículos académicos completos relevantes para el alcance de la revisión sin restricción de idioma, incluyendo artículos de investigación primaria, revisiones sistemáticas y revisiones narrativas. Dos equipos de cuatro revisores evaluaron de forma independiente el texto completo para seleccionar los artículos y extraer los datos, realizando las tareas de forma independiente y cualquier desacuerdo se resolvió mediante arbitraje. Se realizó una síntesis descriptiva de las principales características y hallazgos de los artículos incluidos.
ResultadosSe seleccionaron 69 artículos que abordaban cuestiones éticas y de consentimiento relacionadas con los ECA en 141 países, incluyendo 89 (63%) de ingresos bajos o medios. Los datos extraídos se dividieron en nueve áreas: cuestiones generales (30 artículos; 43%), instrucciones y políticas de las revistas (un artículo; 1,4%), políticas de las instituciones de investigación y agencias financiadoras (tres artículos; 4,3%), reglamentos de los comités de ética (cinco artículos; 7,2%), evaluación y aprobación de los comités de ética (12 artículos; 17%), consentimiento informado y procedimientos relacionados (seis artículos; 8,7%), monitorización del cumplimiento de los ensayos (tres artículos; 4,3%), inquietudes posteriores a la publicación sobre ética y consentimiento (cinco artículos; 7,2%) y recomendaciones para futuras investigaciones (cuatro artículos; 5,8%).
ConclusionesLos puntos clave incluyeron la estandarización de los procesos de aprobación de los comités de ética y la mejora de los procedimientos de obtención del consentimiento informado. Se observaron deficiencias notables en el registro y la notificación de ensayos clínicos en relación con la ética y el consentimiento. La variabilidad observada en las prácticas éticas y de consentimiento en los ECA a nivel mundial debe abordarse mediante un consenso internacional de expertos.
Artículo
Diríjase al área privada de socios de la web de la SEMERGEN, (https://www.semergen.es/index.php?seccion=biblioteca&subSeccion=revistaSEMERGEN ) y autentifíquese.
