





In the Arab world, little is known about cancer patient's satisfaction with the care provided by the oncology nurses. The only explanation for this dearth of knowledge is lack of a specified, valid and reliable tool that can be utilized with all types of cancer. This regional study was conducted to translate and validate the Arabic version of quality of oncology nursing care scale (QONCS).
MethodsBrislin's model of translation was used with a cross-sectional, cross-cultural and psychometric design. A convenience sample of 517 from three countries (Jordan, Oman and Egypt) completed the study's surveys.
ResultsThe results indicated that the total QONCS-Ar was reliable with Cronbach's alpha 0.88 and 0.84, 0.87, 0.83, 0.89 and 0.86 for being supported and confirmed, with the religious and spiritual care, belonging, being valued and being respected domains respectively. Exploratory factor analysis supported the dimensional structure of the 34-item scale with five domains with Kaiser–Meyer–Oklin (KMO) measuring 0.872 and Bartlett's Test of Sphericity being significant (significant p<0.001)
ConclusionQONCS-Ar is a relatively short, valid, reliable and easy to use instrument that can be applied with all types of cancer, research and educational institutions in the Arabic region.
En el mundo árabe se sabe poco acerca de la satisfacción de las pacientes de cáncer con los cuidados prestados por las enfermeras de oncología. La única explicación para esta escasez de conocimiento es la carencia de una herramienta específica, válida y fiable que pueda utilizarse con todos los tipos de cáncer. Se realizó este estudio regional para traducir y validar la versión árabe de la escala QONCS (Quality of Oncology Nursing Care Scale).
MétodosSe utilizó el modelo de traducción de Brislin, con un diseño transversal, transcultural y psicométrico. Una muestra de conveniencia que incluyó a 517 personas procedentes de tres países (Jordania, Omán y Egipto) completó las encuestas del estudio.
ResultadosLos resultados indicaron que la escala QONCS-Ar total era fiable, con un valor de alfa de Cronbach de 0,88, y de 0,84, 0,87, 0,83, 0,89 y 0,86 para respaldo y confirmación de los dominios de cuidados religiosos y espirituales, pertenencia, ser valorada y ser respetada, respectivamente. El Análisis de factor exploratorio respaldó la estructura dimensional de la escala de 34 ítems, con un valor de 0,872 en la escala de cinco dominios KMO (Kaiser–Meyer–Oklin), siendo significativa la Prueba de Esfericidad de Bartlett (significación p<0,001).
ConclusiónQONCS-Ar es un instrumento relativamente breve, válido, fiable y fácil de utilizar, que puede aplicarse a todos los tipos de instituciones de cáncer, investigación y formación en la región arábiga.
Cancer is a chronic and life-threatening disease, and a global health concern that increases the pressure on the healthcare system and healthcare costs.1 The number of patients with cancer is increasing annually: in 2013 there were around 15 million new cases of cancer and more than eight million deaths worldwide; the number is expected to be around 24 million cases per year by 2030.1,2 In the Arab World, the number of patients diagnosed with cancer increased in the last decade and in line with world trends, breast, lung, colorectal prostate and gastric cancers are the commonest cancers.3
As soon as the diagnosis of cancer is confirmed, different treatment modalities such as surgical intervention, chemotherapy and radiotherapy treatment can be used dependent on the type and stage of cancer and patient health's status.4 Despite of the powerful and therapeutic effect of these modalities, many wide ranging side effects and complications are attached to these modalities such as gastrointestinal disturbances, low immunity, oral mucositis, hormonal changes and skin problems.5 In addition to these physical complications, patients with cancer experience many psychosocial feelings such as anxiety, depression, low self-esteem and distress.6 These complexities and difficulties within the cancer management require specialized and multidisciplinary support and care for cancer patients.
In the context of quality of healthcare, oncology nurses play a significant and increasingly important role in providing optimal, high quality, safe, evidence-based and appropriate care to cancer patients. As a bedside worker and as the largest group of healthcare workers, the scope of oncology nursing care goes from the prevention through to palliative phases.7 Quality oncology nursing care was emphasized as a holistic care that is provided in a safe and competent manner, it covers the patients’ needs such as religious care, clinical care, humanistic care, communication and continued support.8 Furthermore, the quality of oncology nursing care is defined as patients’ perception of the care provided by nurses.9 Additionally, as conceptualized previously, the six dimensions reflecting optimal oncology nursing care include Being valued, Respect, Receiving care by communicative and supportive nurses, Confirmed, Spiritual and religious care, and Sense of belonging.10 Therefore, oncology nursing care is an essential component in the quality of the healthcare system. Patient satisfaction and perception about nursing care is an important and fundamental aspect of evaluating cancer patients’ quality of care.11
Cancer patient satisfaction with the hospital experience is a complex and multifactorial strategic goal for the healthcare system and patient satisfaction with oncology nursing care is an integral part of this goal.12 For decades, patient satisfaction has been a pivotal indicator of quality nursing care.13 Importantly, patient's satisfaction with nursing care has been linked with and identified as an influential factor for patient quality of life (QOL),14 compliance with the treatment, hope and coping.11 Therefore, evaluating patients’ satisfaction in cancer patients with oncology nursing care is highly recommended and considered as a priority for nursing researchers, administrators and clinical practitioners.
There is a limited number of specified scales to measure cancer patient's satisfaction with oncology nursing care; only two scales are available namely, oncology patients’ perceptions of the quality of nursing care scale (OPPQNCS)15 and quality of oncology nursing care scale (QONCS).16 As defined early, oncology nursing care is comprehensive, holistic and should address the patient's needs, however, spiritual care is not adequately discussed in the OPPQNCS. In contrast, QONCS is a valid and reliable scale that can be used with all types of cancers, it addresses the main domains of nursing care including being supported and confirmed, religious and spiritual care, belonging, being valued and being respected.16 However, in the Arab world, there is no specific scale in the Arabic language to evaluate the cancer patient's satisfaction with oncology nursing care. Regardless of the large number of cancer patients in the Arab world, little is known about their satisfaction with the care provided by the oncology nurses. The only explanation for this dearth of knowledge is lack of a specified, valid and reliable tool that can be utilized with all types of cancer.
Thus, this regional study was conducted to translate and validate an Arabic version of the quality of oncology nursing care scale (QONCS). The results of the current study could increase nursing researchers’, administrators’ and clinical practitioners’ cross-cultural understanding about patient's satisfaction with oncology nursing care in the Arab region.
Material and methodsDesign and participantsA cross-sectional, cross-cultural and psychometric design was used with a convenience sample of 517 patients with cancer participated and completed the study survey from three countries in the Arab region (200 participants from Jordan, 137 from the Sultanate of Oman and 180 from Egypt). Data were collected from six hospitals and cancer centers (2 hospitals in each country). The research team purposefully conducted this study in three widespread countries to have a broad representative sample from the Middle East and North Africa (MENA) region, consequently, the findings can be generalized so the tool can be widely used. It was recommended to have 3–6 participants per item to perform psychometric testing and factor analysis.17 However, a larger sample was recruited to increase accuracy, validity and generalizability of the results. Ethical approvals were granted from the research and ethics committees in these countries.
The inclusion criteria included: able to read and write Arabic, diagnosed with any type of cancer, were under active treatment, were more than 18 years old, alert, mentally oriented, aware about his diagnosis, were hospitalised for cancer diagnosis or treatment and agreed to participate. Participants were invited to take part by the oncology nurses at each unit and the nurses obtained their initial agreement. Then the research team in each country provided participants with a package including the cover and information sheets (research methods and purposes were detailed) and study surveys in an envelope. The research team asked the participants to return the questionnaire to the focal person in each unit in a sealed envelope without identification details. Then the research member collected the questionnaire on a weekly basis. Participants were assured that they were free to participate, decline and withdraw anytime with no penalty. The data were collected in a three month period between January and March 2020.
MeasuresIn addition to sociodemographic data including participant's age, gender, marital status, education, number of admission times in the last two years including this time and type of cancer, the participants completed the following questionnaires:
Arabic version of Patient Satisfaction with Nursing Care Quality Questionnaire (PSNCQQ)The Patient Satisfaction with Nursing Care Quality Questionnaire-Arabic (PSNCQQ-Ar) is a 17-item scale measuring patient satisfaction with nursing care (PSNC) quality during the hospital stay. The PSNCQQ-Ar consists of two domains, satisfaction with the provided care and satisfaction with the provided information. It has a 5-point Likert scale ranging from poor (1) to excellent (5) and item scores for each domain can be summed and averaged to yield a single value for each patient. Report of PSNC quality can be a composite score (i.e., overall PSNC quality) or domain-based score. For detailed and actionable results, item scores can be reported. The overall Cronbach's alpha coefficient for the PSNCQQ-Ar was excellent and similar across different hospital units (0.96).13
Arabic version of Functional Assessment of Cancer Therapy-General (FACT-G)The Arabic version FACT-G will be used to measure quality of life among cancer patients following cancer treatment modalities. This instrument was originally developed by Cella and colleagues (1993) to measure four cornerstone dimensions of QOL: physical well-being (PWB); social well-being (SOWB); emotional well-being (EWB); and functional well-being (FWB).18 The Arabic version of the FACT-G is a 27-item, self-administered, Likert-type generic format. Each item is rated on a 5-point scale (0–4, where 0=not at all, 1=a little a bit, 2=somewhat, 3=quite a bit, and 4=very much). An additional item related to sexual activity was used to measure sexual satisfaction, with score ranges between 0 and 4, with a higher score indicating a higher sexual satisfaction. The total scores of the Arabic version of the FACT-G range from 0 to 108, with higher rating scores reflecting higher QOL.19
Arabic version of quality of oncology nursing care scale (QONCS)The QONCS is valid and reliable with overall Cronbach alpha 0.95 for the entire scale.20 The instrument consists of 34 items divided into five main domains including being supported and confirmed (16 items), religious and spiritual care (6 items), belonging (5 items), being valued (4 items), and being respected (3 items). Answers were rated using a 5-point Likert scale ranging from 1 (completely disagree) to 5 (completely agree).
Translation process and linguistic validation of the Arabic translationBrislin's model of translation is the most common and widely used method for cross-cultural translation by the researchers worldwide.21,22 It is a well-known method of translating and preparing a valid and reliable scales to be used in different cultures and population.23 According to the Brislin's model, several steps should be undertaken including the scale should be translated by one bilingual researcher from the original language into the target language, then, a another bilingual expert back-translates the scale into the original language (blindly).21
In the current study, Brislin's model (1986) was adopted to translate QONCS into to the Arabic language.24 Structured and clear processes with four steps were undertaken to translate the Quality of oncology nursing care scale (QONCS) from the original English language into the target Arabic language. The process of translation started with forward translation of the scale form English to Arabic language by two native Arabic qualified speakers (PhD in nursing and familiarity with medical terms), then, reconciliation of forward translation was undertaken by a qualified and expert Arabic language speaker (not involved in the first step), after that, back translation of the reconciled version was done by an English speaker fluent in Arabic (PhD in nursing, not participating in the previous steps), finally, the two versions were compared by the primary author. A pilot testing of the translated scale was performed before distributing the scale: a convenience sample of 50 participants who had the same inclusion criteria and were willing to be included in the study's population completed the translated scale. The participants were asked to express their concerns related to clarity of the scale items, flow of the items and time to answer the questions. Preliminary analysis indicated that the translated version of QONCS was reliable with Cronbach's alpha 0.83. No changes were made to the translated scale.
Statistical analysisStatistical Package for the Social Sciences (SPSS version 23.0) was used to analyze the data. Descriptive analyses including mean, standard deviation (SD), frequency and percentage (%) were calculated. Correlational analysis using Pearson (r) was used to determine the relationship between the study's variables. Content and face validity tests were undertaken and finally, exploratory factor analysis (EFA) with Varimax rotation was conducted in the current study.
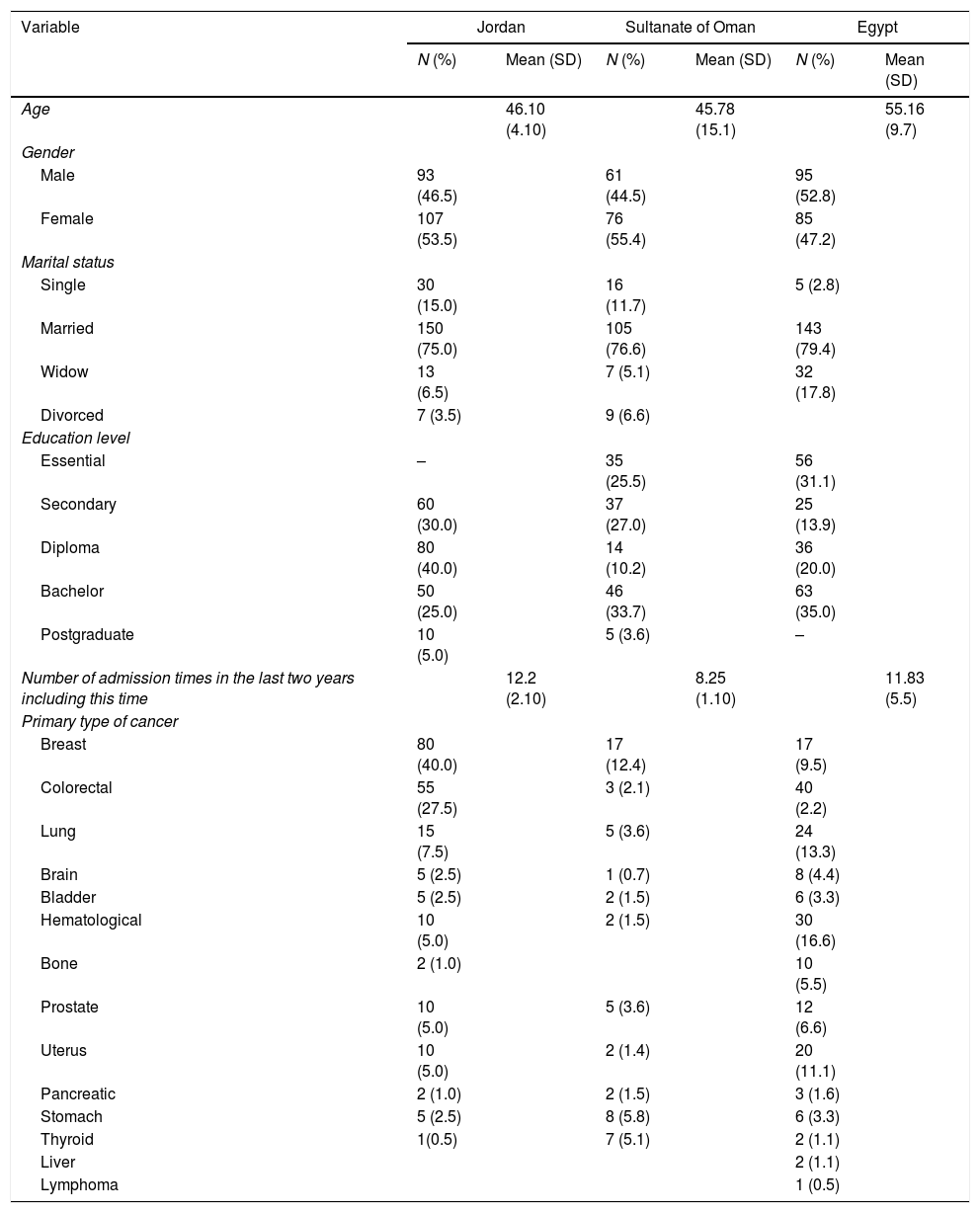
ResultsSociodemographic characteristicsThe sample consisted of 517 patients from three countries (Jordan, 200, 38.7%, Sultanate of Oman, 137, 26.5% and Egypt, 180, 34.8%), more than half of the participants were female (N=268, 51.8%), married (398, 76.8) with breast cancer (114, 22.10%) and colorectal cancer (98. 18.9%). Table 1 details these results.
Sociodemographic characteristics by country (N=517).
| Variable | Jordan | Sultanate of Oman | Egypt | |||
|---|---|---|---|---|---|---|
| N (%) | Mean (SD) | N (%) | Mean (SD) | N (%) | Mean (SD) | |
| Age | 46.10 (4.10) | 45.78 (15.1) | 55.16 (9.7) | |||
| Gender | ||||||
| Male | 93 (46.5) | 61 (44.5) | 95 (52.8) | |||
| Female | 107 (53.5) | 76 (55.4) | 85 (47.2) | |||
| Marital status | ||||||
| Single | 30 (15.0) | 16 (11.7) | 5 (2.8) | |||
| Married | 150 (75.0) | 105 (76.6) | 143 (79.4) | |||
| Widow | 13 (6.5) | 7 (5.1) | 32 (17.8) | |||
| Divorced | 7 (3.5) | 9 (6.6) | ||||
| Education level | ||||||
| Essential | – | 35 (25.5) | 56 (31.1) | |||
| Secondary | 60 (30.0) | 37 (27.0) | 25 (13.9) | |||
| Diploma | 80 (40.0) | 14 (10.2) | 36 (20.0) | |||
| Bachelor | 50 (25.0) | 46 (33.7) | 63 (35.0) | |||
| Postgraduate | 10 (5.0) | 5 (3.6) | – | |||
| Number of admission times in the last two years including this time | 12.2 (2.10) | 8.25 (1.10) | 11.83 (5.5) | |||
| Primary type of cancer | ||||||
| Breast | 80 (40.0) | 17 (12.4) | 17 (9.5) | |||
| Colorectal | 55 (27.5) | 3 (2.1) | 40 (2.2) | |||
| Lung | 15 (7.5) | 5 (3.6) | 24 (13.3) | |||
| Brain | 5 (2.5) | 1 (0.7) | 8 (4.4) | |||
| Bladder | 5 (2.5) | 2 (1.5) | 6 (3.3) | |||
| Hematological | 10 (5.0) | 2 (1.5) | 30 (16.6) | |||
| Bone | 2 (1.0) | 10 (5.5) | ||||
| Prostate | 10 (5.0) | 5 (3.6) | 12 (6.6) | |||
| Uterus | 10 (5.0) | 2 (1.4) | 20 (11.1) | |||
| Pancreatic | 2 (1.0) | 2 (1.5) | 3 (1.6) | |||
| Stomach | 5 (2.5) | 8 (5.8) | 6 (3.3) | |||
| Thyroid | 1(0.5) | 7 (5.1) | 2 (1.1) | |||
| Liver | 2 (1.1) | |||||
| Lymphoma | 1 (0.5) | |||||
Reliability for the Arabic version of QONCS (QONCS-Ar) was evaluated. Cronbach alpha and McDonald's omega coefficients value were calculated. The results indicated that the total QONCS-Ar was reliable with Cronbach's alpha 0.88 and 0.84, 0.87, 0.83, 0.89 and 0.86 (omega=0.85 for total QONCS-Ar, 0.81, 0.84, 0.79, 0.86 and 0.83) for being supported and confirmed, religious and spiritual care, belonging, being valued and being respected domains respectively.
Content validity of the QONCS-Ar was evaluated in the current study. Three experts in nursing (holding PhD in nursing) rated the scale's items according to the degree of clarity, using simple language and opacity criteria. Content validity index (CVI) was calculated and the results showed that all the scale's items had CVI of more than 0.84. Furthermore, the results during pilot testing indicated that the participants (N=50) agreed (κ=0.832) that the scale's items were simple, easy to understand, clear and in logical flow.
Convergent validityConvergent validity was checked in the current study. Relationship between QONCS-Ar (total and subscales) and PSNCQQ-Ar was explored by using Pearson correlation test. In addition, the relationship between QONCS-Ar (total and subscales) and Arabic version of FACT-G was tested. Positive relationships were found between QONCS-Ar (Total scale) and sub-domains with the quality of life as measured by FACT-G. In addition, positive relationships were found between QONCS-Ar (Total scale) and sub-domains and PSNCQQ-Ar (total scale). Results are detailed in Table 2.
Pearson correlation coefficients between the QONCS-Ar and PSNCQQ-Ar and FACT-G (N=571).
| Total QONCS-Ar | 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|---|
| FACT-G | 0.81* | 0.77* | 0.73* | 0.71* | 0.83* | 0.79* |
| PSNCQQ-Ar | 0.78* | 0.71* | 0.69* | 0.79* | 0.80* | 0.77* |
1=Being Supported and Confirmed, 2=Religious and Spiritual Care, 3=Belonging, 4=Being Valued and 5=Being Respected.
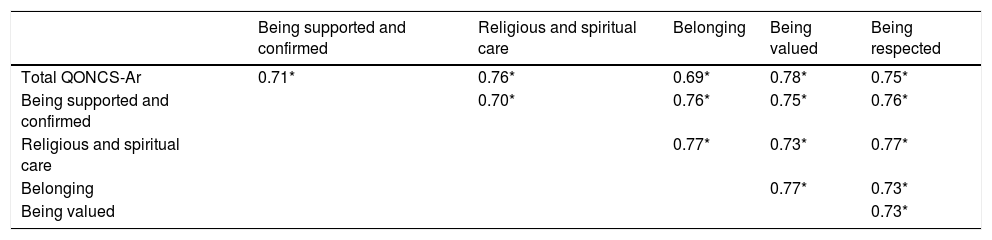
Bivariate correlation utilizing Pearson correlation was used to explore the relationships among the 5 QONCS-Ar domains; strong positive relationships between total QONCS-Ar and being supported and confirmed, religious and spiritual care, belonging, being valued and being respected domains (r=0.71, 0.76, 0.69, 0.78, and 0.75, p<0.001 respectively). Positive relationships between the 5 QONCS-Ar domains were found. Table 3 details these results.
Pearson correlation coefficients for the five domains of the QONCS-Ar (N=517).
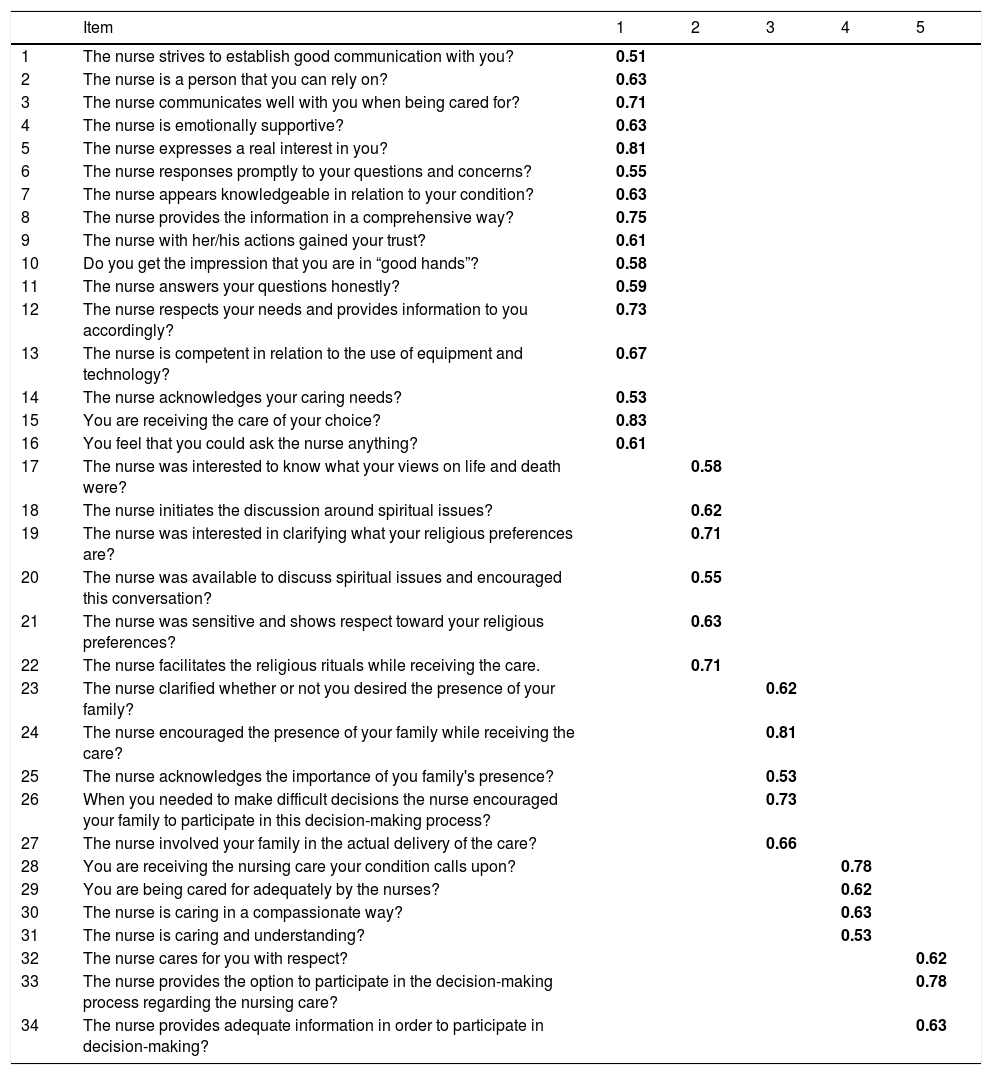
Scale structure was evaluated by using exploratory factor analysis (EFA), principle components analysis with Varimax rotation was also performed. The standard item's loading 0.40 was used as a cutoff point.25 The results showed all items on the scale Being supported and confirmed domain (16 items) had factor loadings ranging from 0.51 to 0.83, all items on Religious and spiritual care domain (6 items) had loading factors ranging from 0.55 to 0.71. Furthermore, Belonging domain's items (5 items) had loading factors ranging from 0.53 to 0.81, all items on Being valued domain (4 items) had loading factors ranging from 0.53 to 0.78, and factors load for Being respected domain (3 items) were between 0.62 and 0.78. Kaiser–Meyer–Oklin (KMO) was 0.872 and Bartlett's Test of Sphericity was significant (significant (p<0.001) (Table 4).
Factor loadings of the exploratory factor analysis results for QONCS-Ar (N=517).
| Item | 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|---|
| 1 | The nurse strives to establish good communication with you? | 0.51 | ||||
| 2 | The nurse is a person that you can rely on? | 0.63 | ||||
| 3 | The nurse communicates well with you when being cared for? | 0.71 | ||||
| 4 | The nurse is emotionally supportive? | 0.63 | ||||
| 5 | The nurse expresses a real interest in you? | 0.81 | ||||
| 6 | The nurse responses promptly to your questions and concerns? | 0.55 | ||||
| 7 | The nurse appears knowledgeable in relation to your condition? | 0.63 | ||||
| 8 | The nurse provides the information in a comprehensive way? | 0.75 | ||||
| 9 | The nurse with her/his actions gained your trust? | 0.61 | ||||
| 10 | Do you get the impression that you are in “good hands”? | 0.58 | ||||
| 11 | The nurse answers your questions honestly? | 0.59 | ||||
| 12 | The nurse respects your needs and provides information to you accordingly? | 0.73 | ||||
| 13 | The nurse is competent in relation to the use of equipment and technology? | 0.67 | ||||
| 14 | The nurse acknowledges your caring needs? | 0.53 | ||||
| 15 | You are receiving the care of your choice? | 0.83 | ||||
| 16 | You feel that you could ask the nurse anything? | 0.61 | ||||
| 17 | The nurse was interested to know what your views on life and death were? | 0.58 | ||||
| 18 | The nurse initiates the discussion around spiritual issues? | 0.62 | ||||
| 19 | The nurse was interested in clarifying what your religious preferences are? | 0.71 | ||||
| 20 | The nurse was available to discuss spiritual issues and encouraged this conversation? | 0.55 | ||||
| 21 | The nurse was sensitive and shows respect toward your religious preferences? | 0.63 | ||||
| 22 | The nurse facilitates the religious rituals while receiving the care. | 0.71 | ||||
| 23 | The nurse clarified whether or not you desired the presence of your family? | 0.62 | ||||
| 24 | The nurse encouraged the presence of your family while receiving the care? | 0.81 | ||||
| 25 | The nurse acknowledges the importance of you family's presence? | 0.53 | ||||
| 26 | When you needed to make difficult decisions the nurse encouraged your family to participate in this decision-making process? | 0.73 | ||||
| 27 | The nurse involved your family in the actual delivery of the care? | 0.66 | ||||
| 28 | You are receiving the nursing care your condition calls upon? | 0.78 | ||||
| 29 | You are being cared for adequately by the nurses? | 0.62 | ||||
| 30 | The nurse is caring in a compassionate way? | 0.63 | ||||
| 31 | The nurse is caring and understanding? | 0.53 | ||||
| 32 | The nurse cares for you with respect? | 0.62 | ||||
| 33 | The nurse provides the option to participate in the decision-making process regarding the nursing care? | 0.78 | ||||
| 34 | The nurse provides adequate information in order to participate in decision-making? | 0.63 |
1=being supported and confirmed, 2=religious and spiritual care, 3=belonging, 4=being valued and 5=being respected.
Bolded numbers mean that items have adequate loading. Kaiser–Meyer–Olkin was 0.872. Bartlett test of sphericity was significant (p<0.001).
In the Arab region, cancer as elsewhere, is a common life-threatening disease, with the number of patients diagnosed with and treated for cancer increasing annually.26 Worldwide, continuous assessment and monitoring of cancer care has been increased by health researchers and clinical practitioners to improve patient's outcomes such as patient satisfaction.27 Recently, cancer patients’ perception about oncology nursing care is becoming an area of interest for nursing researchers, administrators and clinical practitioners.27 However, little is known about the perception of cancer patients about oncology nursing care in the Arab world. This is mainly because there is no short, valid, reliable and easy to use instrument that can be used with all types of cancer. Therefore, the current study responded to this critical issue and important demand and was conducted to translate and validate the QONCS.
Quality of oncology nursing care scale (QONCS) is a relatively short, valid, reliable, specific and easy to use scale that was developed to measure the patients’ satisfaction with oncology nursing care. The scale has five domains including being supported and confirmed, religious and spiritual care, belonging, being valued and being respected.20 The scale is available in the original English and Chinese languages.28 To the research teams’ knowledge, this is the first study aimed to translate and validate the QONCS in an Arabic region. The results of the current study could increase our understanding about the patient's perception of provided care.
The reliability analysis indicated that the total QONCS-Ar was reliable with Cronbach's alpha was of 0.88 comparing to 0.95 of the original English language scale20 and 0.946 for the Chinese version of the QONCS.28 Furthermore, the results indicated that the five domains were reliable with Cronbach's alpha for being supported and confirmed 0.84, religious and spiritual care 0.87, belonging 0.83, being valued 0.89 and being respected domains 0.86 domains respectively. These results are congruent with the reliability results of the original scale (Cronbach's alpha being 0.83 for being supported and confirmed, 0.90 for religious and spiritual care, 0.90 for belonging, 0.91 for being valued and 0.86 for being respected domains.20 In addition, these current results support the results of the Chinese version as the reliability results of the QONCS domains ranged between 0.735 and 0.928.28 In addition, the dimensional structure of the QONCS-Ar was evaluated. Bivariate correlation analysis was performed to explore the relationships between the QONCS-Ar domains. Significant correlations among the five domains ranged from 0.69 to 0.78. These findings supported the dimensional structure of the translated scale.
Convergent validity was checked in the current study, positive relationships between QONC-Ar (total scale/domains) and quality of life as measured by FACT-G were reported. These findings supported the previous literature; high quality of care was associated positively with the QOL status among patients with cancer,29 reducing the pain and enhancing the prognosis.30,31 Furthermore, positive relationships were found between QONC-Ar (total scale/domains) and PSNCQQ-Ar. These associations indicate that PSNCQQ-Ar is a valid and reliable tool that can be used to determine the convergent validity of the QONC-Ar. Additionally, both scales can be used to measure patient's satisfaction with the oncology nursing care, however, as discussed early, QONCS-Ar is a more comprehensive tool and addresses the main nursing care domains.
Exploratory factor analysis was used to evaluate the structure of the QONCS-Ar (34 items). The results supported the dimensional structure of the original scale and the Chinese version of QONCS.20,28 The results showed that Kaiser–Meyer–Olkin was 0.872, and Bartlett test of sphericity was significant (p<0.001) comparing to Kaiser–Meyer–Olkin (0.913) for the original scale. Furthermore, the results showed that all items on the Being supported and confirmed domain (16 items) had factor loadings ranging from 0.51 to 0.83, all items on Religious and spiritual care domain (6 items) had loading factor ranging from 0.55 to 0.71. Furthermore, belonging domain's items (5 items) had a loading factor ranging from 0.53 to 0.81, all items on being valued domain (4 items) had loading factors ranging from 0.53 to 0.78, and factors load for being respected domain (3 items) were between 0.62 and 0.78. These findings supporting the development structure of the original scale and Chinese version of QONCS.20,28
Although the current study successfully translated and validated a specific and essential instrument to evaluate the cancer patient's satisfaction with oncology nursing care in Arabic countries, some limitations should be acknowledged. The current study was cross-sectional, this decreased the ability to evaluate the tool over the time, and therefore, future research with repeated measures is recommended.
ConclusionArabic version of QONCS (QONCS-Ar) is a valid, reliable, easy to use and practical instrument for measuring the quality of oncology nursing care from the patient's perception. The scale provides pivotal information about the main nursing care domains. These results could be helpful for nursing researchers, administrators and clinical practitioners to plan and allocate resources at the institutional level to increase the quality of oncology nursing care, and increase patients’ satisfaction.
Conflicts of interestThe authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
FundingThe author(s) received no financial support for the research, authorship, and/or publication of this article.
The authors thank the participants for their effort.

