




The COVID-19 pandemic created a backlog in colorectal cancer (CRC) screening and surveillance colonoscopies. The real impact in Argentina is not fully known.
GoalTo estimate the impact of the COVID-19 pandemic on CRC prevention by comparing the number of CRC screening and surveillance consults in a clinical decision support-tool used in Argentina before, during and after pandemic lockdown.
MethodsWe analyzed data from May 2019 to December 2021 from CaPtyVa, a clinical decision support tool for CRC screening and surveillance. Queries were divided in pre-pandemic (May 2019 to March 2020), lockdown (April 2020 to December 2020), and post-lockdown (January 2021 to December 2021). The number of CRC monthly screening and surveillance visits were compared among the three periods and stratified according to CRC risk.
ResultsOverall, 27,563 consults were analyzed of which 9035 were screening and 18,528 were surveillance. Pre-pandemic, the median number of screening consults was 346 per month (IQR25–75 280–410). There was a decrease to 156 (80–210)/month (p<0.005) during lockdown that partially recovered during post-lockdown to 230 (170–290)/month (p=0.05). Pre-pandemic, the median number of surveillance consults was 716 (560–880)/month. They decreased to 354 (190–470)/month during lockdown (p<.05) and unlike screening, completely recovered during post-lockdown to 581 (450–790)/month.
ConclusionsThere was a >50% decrease in the number of CRC screening and surveillance consults registered in CaPtyVa during lockdown in Argentina. Post-lockdown, surveillance consults recovered to pre-pandemic levels, but screening consults remained at 66% of pre-pandemic levels. This has implications for delays in CRC diagnoses and patient outcomes.
La pandemia de COVID-19 provocó atraso en las colonoscopias de detección y vigilancia del cáncer colorrectal (CCR).
ObjetivoEstimar el impacto de la pandemia de COVID-19 en la prevención del CCR comparando el número de consultas de pesquisa y vigilancia del CCR en una herramienta digital de apoyo a la decisión clínica utilizada en Argentina antes, durante y después del confinamiento.
MétodosAnalizamos datos entre mayo 2019 a diciembre 2021 de CaPtyVa, una herramienta digital de apoyo a la toma de decisiones clínicas para la pesquisa y vigilancia del CCR. Las consultas se dividieron en prepandemia (mayo 2019- marzo 2020), confinamiento (abril 2020- diciembre 2020) y post-confinamiento (enero 2021-diciembre 2021). El número de visitas mensuales de pesquisa y vigilancia de CCR se comparó entre períodos y se estratificó según riesgo de CCR.
ResultadosPrepandemia, la mediana de consultas de detección fue 346 mes (IQR25-75 280-410). Hubo una disminución a 156 (80-210)/mes (p<0,005) durante el confinamiento que ascendió a 230 (170-290)/mes (p=0,05) en el post-confinamiento. Prepandemia, la mediana de consultas de vigilancia fue 716 (560-880)/mes. Disminuyeron a 354 (190-470)/mes durante el confinamiento (p<0,05) y se recuperaron por completo durante el post-confinamiento.
ConclusionesHubo una disminución >50% en el número de consultas de detección y vigilancia de CCR registradas en CaPtyVa durante el confinamiento en Argentina. Post-confinamiento, las consultas de vigilancia se recuperaron a niveles prepandemia, pero las consultas de detección se mantuvieron en el 66 % de niveles históricos. Esto tendría implicaciones en los diagnósticos y pronósticos de CCR.
Globally, the COVID-19 pandemic has had a significant impact on healthcare systems.1 Because of events that took place during the evolution of the pandemic at its different stages, healthcare systems and practices experienced major adaptations. Most non-urgent medical visits were deferred or moved to virtual encounters and many of the health, human and technical resources were redirected to assist the ongoing health crisis. As an example, screening procedures aiming to prevent neoplastic conditions suffered a profound backlog.2,3 There have been reports of significant delays in colorectal cancer (CRC) screening and surveillance.4 This may lead to a future rise in the cases of potentially preventable CRC.5 In addition, it is not well known if the backlog of care has been addressed and case volumes have recovered to pre-pandemic levels as we move forward to the stage of “living with the pandemic”. This estimation is difficult to perform accurately and to date, only indirect data from a handful of centres worldwide have been published.6
CRC is one of the leading causes of cancer death in Argentina.7 Despite this, there is scarce data limited to referral centres showing the impact of screening colonoscopy on CRC incidence in the country.8–10 The lack of a unified healthcare system, including public, private, and social insurance subsectors, and the geographic variation in health services by province all make it difficult to estimate trends in screening procedures across the country.
In 2019, a mobile application, Captyva designed to offer evidence-based guidance on appropriate screening and surveillance for CRC was launched in Argentina. Captyva serves as an electronic clinical decision support system for healthcare providers and is adapted to local practice guidelines issued by the National Cancer Institute.11 This application is endorsed by both the Argentinean Society of Gastroenterology and the Argentinean Society of Gastrointestinal Endoscopy and had a high acceptance among physicians throughout the country- from general practitioners to gastroenterologists.
For every encounter in which it is used, Captyva records and stores the query and the main clinical features. Due to the widespread acceptance since its launching, the data stored in the app can provide a surrogate measure of changes in CRC screening and surveillance consults in areas where it is used. The aim of this study is to assess changes in the number of screening and surveillance consults recorded by Captyva during the different phases of COVID-19 pandemic and whether volume of consults returns to baseline after re-opening after the pandemic lockdown.
The secondary outcome is to assess the differences in the characteristics of patients that were assessed.
Materials and methodsCaPtyVa mobile applicationThe CaPtyVa Mobile app was custom developed with joined efforts of the Endoscopic Society of Buenos Aires (ENDIBA) and the National Institute of Cancer (INC). The purpose of its creation is to improve physician knowledge about CRC screening and surveillance and adherence to clinical practice guidelines. The app stores information about all the current local clinical practice guidelines related to CRC screening and surveillance. Through its decision-making algorithms, artificial intelligence assists physicians in the screening process recommendation. In the screening function, the app helps physicians to easily classify patients according to their individual CRC risk and to determine how and when to start screening tests. In the surveillance function, the app assists physicians in determining when to repeat the next colonoscopy based on risk and polyp history, according to guideline recommendations. Captyva utility has been previously described in a study published by Pereyra et al.11 Briefly, endoscopy specialists were asked to complete a questionnaire which included standardized case-problems to determine when and how should CRC screening and surveillance be performed, with and without the use of Captyva. There was a significant increase in the number of correct answers when these specialists used Captyva to answer the questions provided.
Captyva is endorsed by the most important local scientific societies: the Argentinean Gastroenterology Society, Argentinean Gastrointestinal Endoscopy Society, Argentinean Internal Medicine Society as well as the Argentinean Family Medicine Society. It has had a widespread acceptance among internal medicine, surgeons and gastroenterologists in Argentina and since its beginning in 2019 it has received and stored more than 35,000 medical queries; in addition, it has exhibited stable use since its launch with a median retention rate of 18.2%. Captyva database keeps a real-time record of all the visits regarding both functions – CRC screening and surveillance. This database was used for the purpose of this study.
Study design and populationIn this retrospective, cross-sectional study using the Captyva database, we included screening and surveillance consults in adults >17 years old from May 2019 to January 2022. We chose May 2019 as the start date for this study because that is when Captyva was reliably capturing data.
From March 2020 to December 2020, a strict lockdown was implemented in Argentina due to the COVID-19 pandemic. This had a significant impact on the national healthcare system and how resources were allocated.12 Following the lockdown, during 2021 there was a slow but steady normalization of medical assistance and healthcare-resource allocation. Hence, for comparative purposes we divided the study population into three groups, according to the following periods of time: from May 2019 to March 2020 (pre-pandemic baseline period), from April 2020 to December 2020 (lockdown period) and from January 2021 to January 2022 (post-lockdown period).
Outcomes and variables of studyThe main outcome was the number of consults registered during the three periods of time.
The secondary outcome was the comparison of physician and patients characteristics in the different periods. The following variables were recorded: state and city, physician's specialty, patient's age and gender, risk of CRC according to local guidelines (average, moderate or high), history of hereditary CRC syndromes (i.e., Lynch Syndrome, Peutz-Jeghers Syndrome, Familiar Adenomatous Polyp Syndrome), history of inflammatory bowel disease, familiar history of digestive and extra-digestive neoplasia. In the case of surveillance consults, the following variables were also recorded: previous colonoscopy bowel cleansing quality, colonic examination completeness, prior history of colorectal adenoma and/or CRC, characteristics of colorectal adenomas: histology, size, history of piecemeal resection of colorectal adenoma, history of serrated polyps.
Secondary outcomes included change in proportion of low-, average-, and high-risk consults. Risk definitions were taken from the Argentinean National Institute of Cancer. recommendations issued in 2015.13 Briefly, low-risk patients refers to subjects with history of 1–2 tubular adenomas <10mm of diameter and with low-grade dysplasia. Average or intermediate-risk refers to subjects with a history of 3–10 adenomas or at least one adenoma >10mm of diameter, or predominant villous component and/or high-grade dysplasia. High-risk patients refer to subjects with a history of more than 10 adenomas, or at least one with more than 20mm of diameter or one or more serrated polyps with dysplasia.
Statistical analysisStata software was used for the analysis (v11.1, Statacorp, College Station, Texas USA). Median number of consults for CRC screening and surveillance were compared among the pre-pandemic baseline, lockdown and post-lockdown periods, respectively. Categorical variables were described as percentages; numerical variables were described as median along with their 25–75% interquartile range or mean with their standard deviation in the case of normally distributed variables. We used Kruskal–Wallis test or one-way analysis of variance for the comparison of numerical non-parametric or parametric variables, respectively and chi-square test for the comparison of categorical variables. Analysis of the modification in the number of consults according to the risk of patients in the screening and surveillance consults was made. Analysis of covariance was done to determine if changes in the number of consults may have been influenced by potential confounding factors identified in univariate analysis. A p value of less than 0.05 was considered as statistically significant.
ResultsOverallDuring the study period, 27,563 consults were included for analysis.
CRC screeningNumber of consultations in relation with the blacklog.
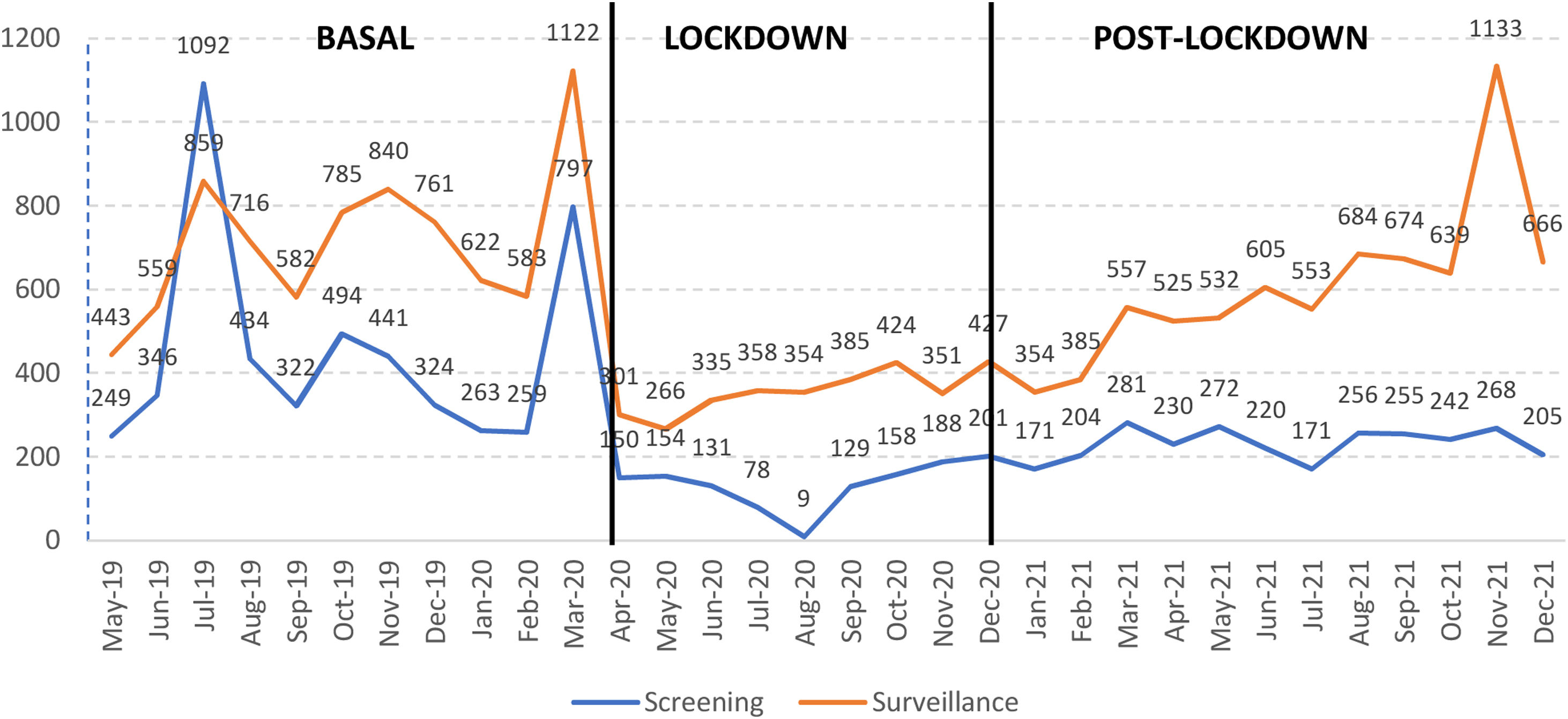
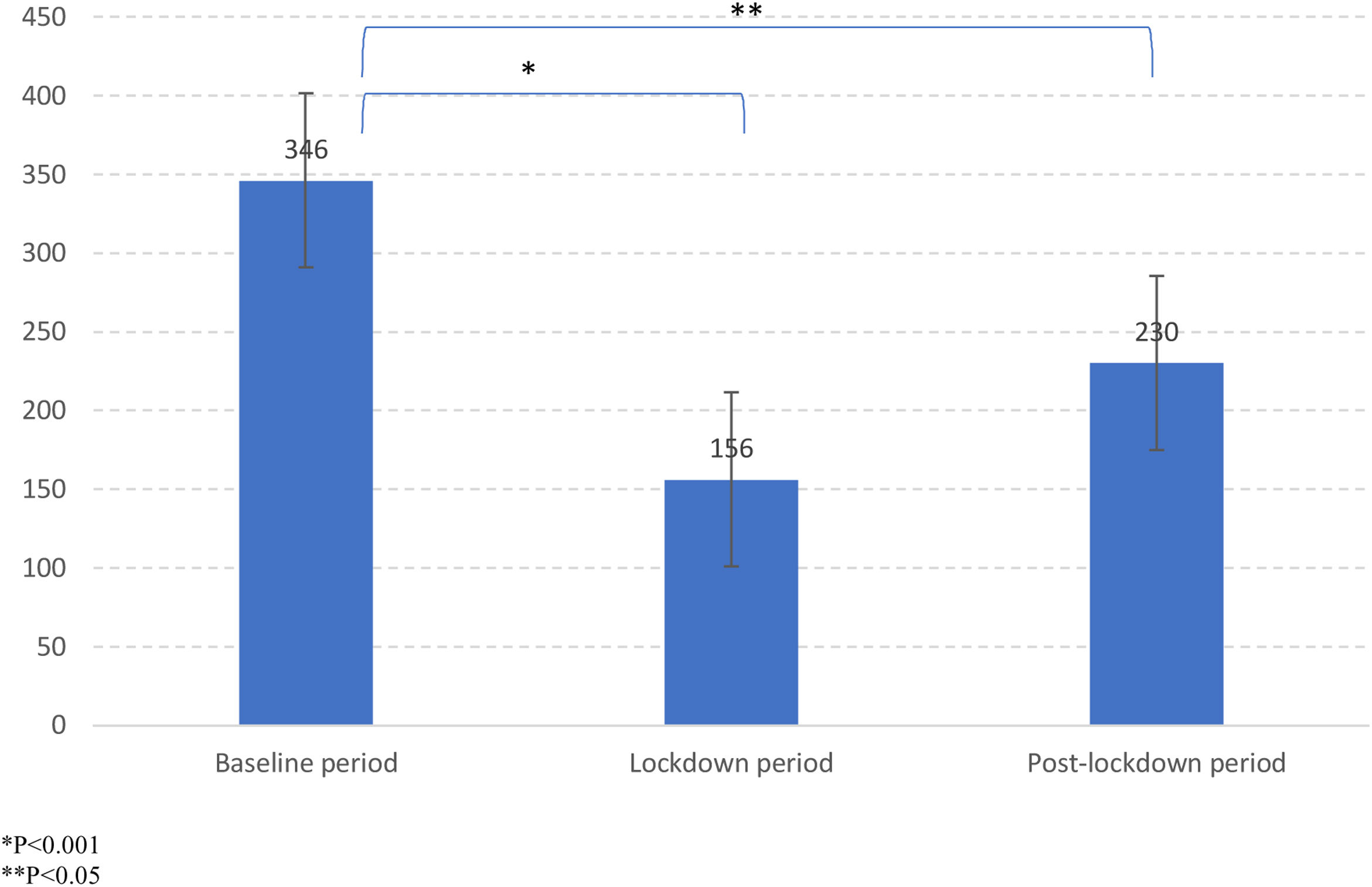
Overall, there were 9035 CRC screening consults available for analysis. Chart 1 shows the monthly progression of the number of consults from May 2019 to January 2022. A steep decrease is observed in April 2020, when strict lockdown due to COVID-19 pandemic was implemented, with a progressive increase observed throughout the rest of the study period. Chart 2 shows the results of the main outcome. During the pre-pandemic baseline period, there were 5021 registered screening consults, with a median of 346 (280–410) monthly visits. There was a significant drop in monthly visits to a median of 156 (80–210) (p<0.005) during the lockdown period. Even though there was an increase in the number of consults during the post-lockdown period [monthly median of 230 (170–290)], this was still significantly lower when compared to the baseline period (p<0.05), with a difference of 32.6%).


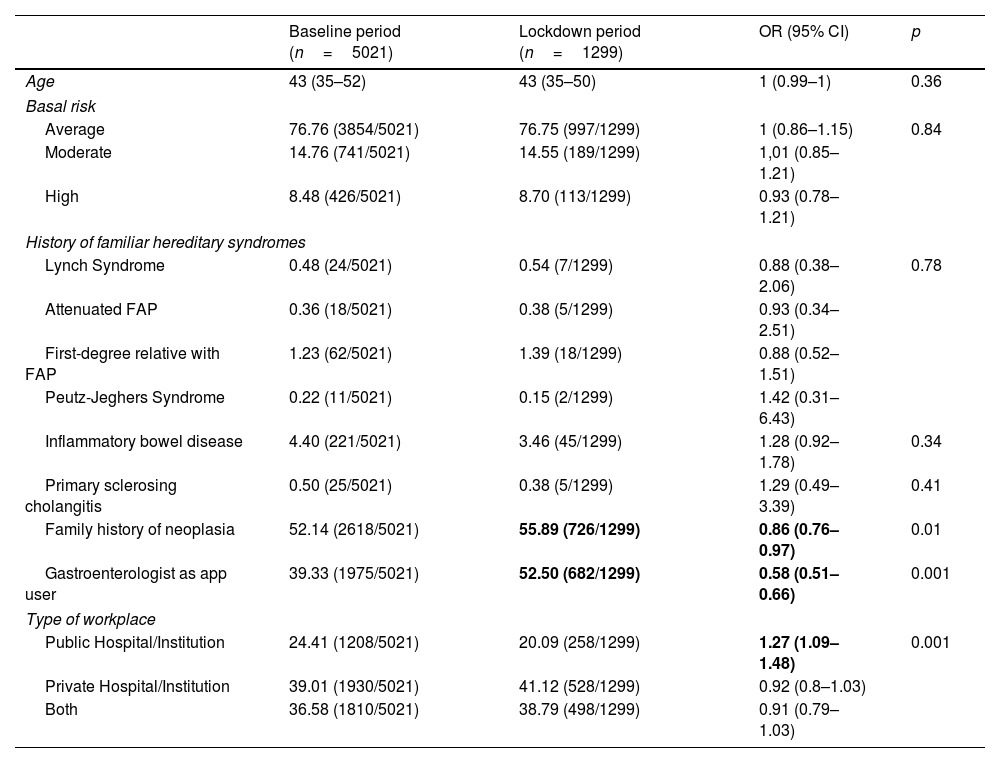
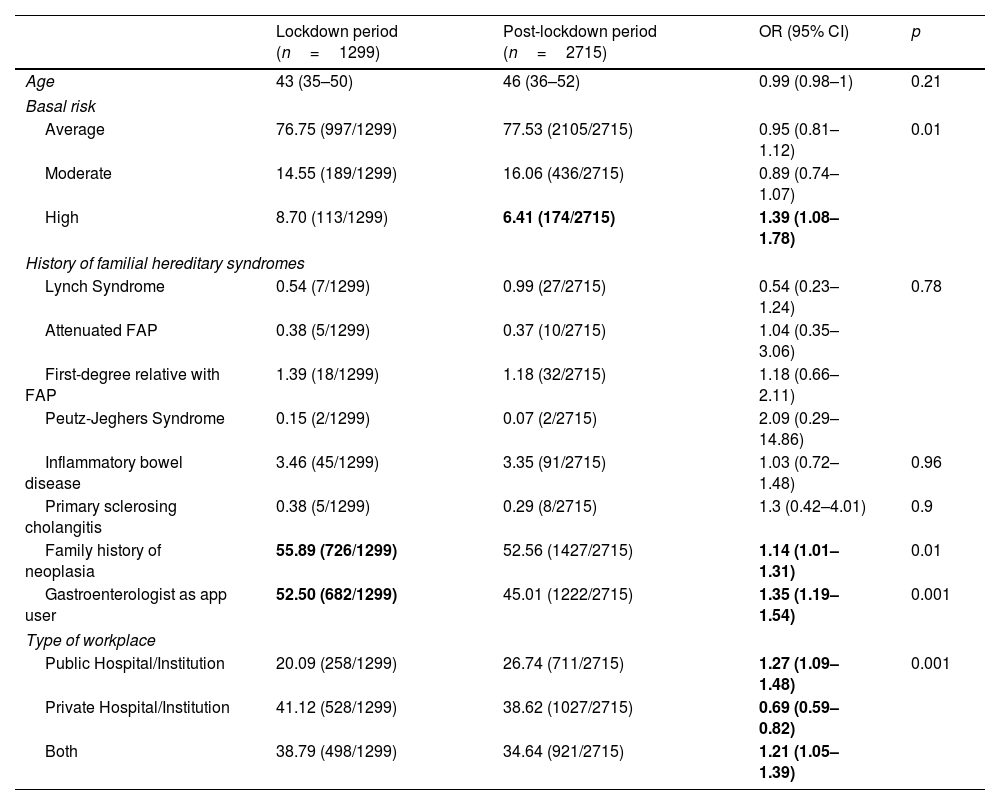
Tables 1 and 2 compare the major characteristics of the consults. Among users of the app, 42.9% were gastroenterologists, followed by surgeons (15.9%) and internal medicine specialists (11.21%). In terms of CRC risk, 77% of visits were average risk for CRC, 15.12% moderate risk for CRC, and 52.8% reported family history of CRC. The majority of queries happened in the Buenos Aires metropolitan area. During the period of strict lockdown, there was a relatively higher proportion of screening consults on patients with higher-risk due to familiar history of neoplasia when compared to baseline (55.9% vs. 52.1%, p=0.05). Additionally, there was an increase in the proportion of visits made by gastroenterologists during this period (52.5% vs. 39.3%, p=0.001).
Comparison of characteristics of the screening consults during baseline and lockdown periods.
| Baseline period (n=5021) | Lockdown period (n=1299) | OR (95% CI) | p | |
|---|---|---|---|---|
| Age | 43 (35–52) | 43 (35–50) | 1 (0.99–1) | 0.36 |
| Basal risk | ||||
| Average | 76.76 (3854/5021) | 76.75 (997/1299) | 1 (0.86–1.15) | 0.84 |
| Moderate | 14.76 (741/5021) | 14.55 (189/1299) | 1,01 (0.85–1.21) | |
| High | 8.48 (426/5021) | 8.70 (113/1299) | 0.93 (0.78–1.21) | |
| History of familiar hereditary syndromes | ||||
| Lynch Syndrome | 0.48 (24/5021) | 0.54 (7/1299) | 0.88 (0.38–2.06) | 0.78 |
| Attenuated FAP | 0.36 (18/5021) | 0.38 (5/1299) | 0.93 (0.34–2.51) | |
| First-degree relative with FAP | 1.23 (62/5021) | 1.39 (18/1299) | 0.88 (0.52–1.51) | |
| Peutz-Jeghers Syndrome | 0.22 (11/5021) | 0.15 (2/1299) | 1.42 (0.31–6.43) | |
| Inflammatory bowel disease | 4.40 (221/5021) | 3.46 (45/1299) | 1.28 (0.92–1.78) | 0.34 |
| Primary sclerosing cholangitis | 0.50 (25/5021) | 0.38 (5/1299) | 1.29 (0.49–3.39) | 0.41 |
| Family history of neoplasia | 52.14 (2618/5021) | 55.89 (726/1299) | 0.86 (0.76–0.97) | 0.01 |
| Gastroenterologist as app user | 39.33 (1975/5021) | 52.50 (682/1299) | 0.58 (0.51–0.66) | 0.001 |
| Type of workplace | ||||
| Public Hospital/Institution | 24.41 (1208/5021) | 20.09 (258/1299) | 1.27 (1.09–1.48) | 0.001 |
| Private Hospital/Institution | 39.01 (1930/5021) | 41.12 (528/1299) | 0.92 (0.8–1.03) | |
| Both | 36.58 (1810/5021) | 38.79 (498/1299) | 0.91 (0.79–1.03) | |
FAP: familiar adenomatous polyposis.
Bold: Confidence Intervals and Pvalues indicate strong evidence against the Null Hypothesis of no difference, rejecting it.
Comparison of characteristics of the screening consults during lockdown and post-lockdown periods.
| Lockdown period (n=1299) | Post-lockdown period (n=2715) | OR (95% CI) | p | |
|---|---|---|---|---|
| Age | 43 (35–50) | 46 (36–52) | 0.99 (0.98–1) | 0.21 |
| Basal risk | ||||
| Average | 76.75 (997/1299) | 77.53 (2105/2715) | 0.95 (0.81–1.12) | 0.01 |
| Moderate | 14.55 (189/1299) | 16.06 (436/2715) | 0.89 (0.74–1.07) | |
| High | 8.70 (113/1299) | 6.41 (174/2715) | 1.39 (1.08–1.78) | |
| History of familial hereditary syndromes | ||||
| Lynch Syndrome | 0.54 (7/1299) | 0.99 (27/2715) | 0.54 (0.23–1.24) | 0.78 |
| Attenuated FAP | 0.38 (5/1299) | 0.37 (10/2715) | 1.04 (0.35–3.06) | |
| First-degree relative with FAP | 1.39 (18/1299) | 1.18 (32/2715) | 1.18 (0.66–2.11) | |
| Peutz-Jeghers Syndrome | 0.15 (2/1299) | 0.07 (2/2715) | 2.09 (0.29–14.86) | |
| Inflammatory bowel disease | 3.46 (45/1299) | 3.35 (91/2715) | 1.03 (0.72–1.48) | 0.96 |
| Primary sclerosing cholangitis | 0.38 (5/1299) | 0.29 (8/2715) | 1.3 (0.42–4.01) | 0.9 |
| Family history of neoplasia | 55.89 (726/1299) | 52.56 (1427/2715) | 1.14 (1.01–1.31) | 0.01 |
| Gastroenterologist as app user | 52.50 (682/1299) | 45.01 (1222/2715) | 1.35 (1.19–1.54) | 0.001 |
| Type of workplace | ||||
| Public Hospital/Institution | 20.09 (258/1299) | 26.74 (711/2715) | 1.27 (1.09–1.48) | 0.001 |
| Private Hospital/Institution | 41.12 (528/1299) | 38.62 (1027/2715) | 0.69 (0.59–0.82) | |
| Both | 38.79 (498/1299) | 34.64 (921/2715) | 1.21 (1.05–1.39) | |
Bold: Confidence Intervals and Pvalues indicate strong evidence against the Null Hypothesis of no difference, rejecting it.
As observed in Table 2, there was a significant increase in the proportion of screening consults during post-lockdown period among subjects with moderate and/or high risk of CRC. This remained significant after adjusting for familiar history of CRC and history of hereditary syndromes [OR 1.12 (1.01–1.65)].
SurveillanceNumber of consultations in relation with the blacklog.
During the study period, 18,528 surveillance consults were registered for analysis. Chart 1 shows the monthly modifications in the number of surveillance consults throughout the study period. As observed in the case of screening consults, surveillance consults experienced a significant drop after the implementation of lockdown in 2020, with a progressive recovery in number in the post-lockdown period.
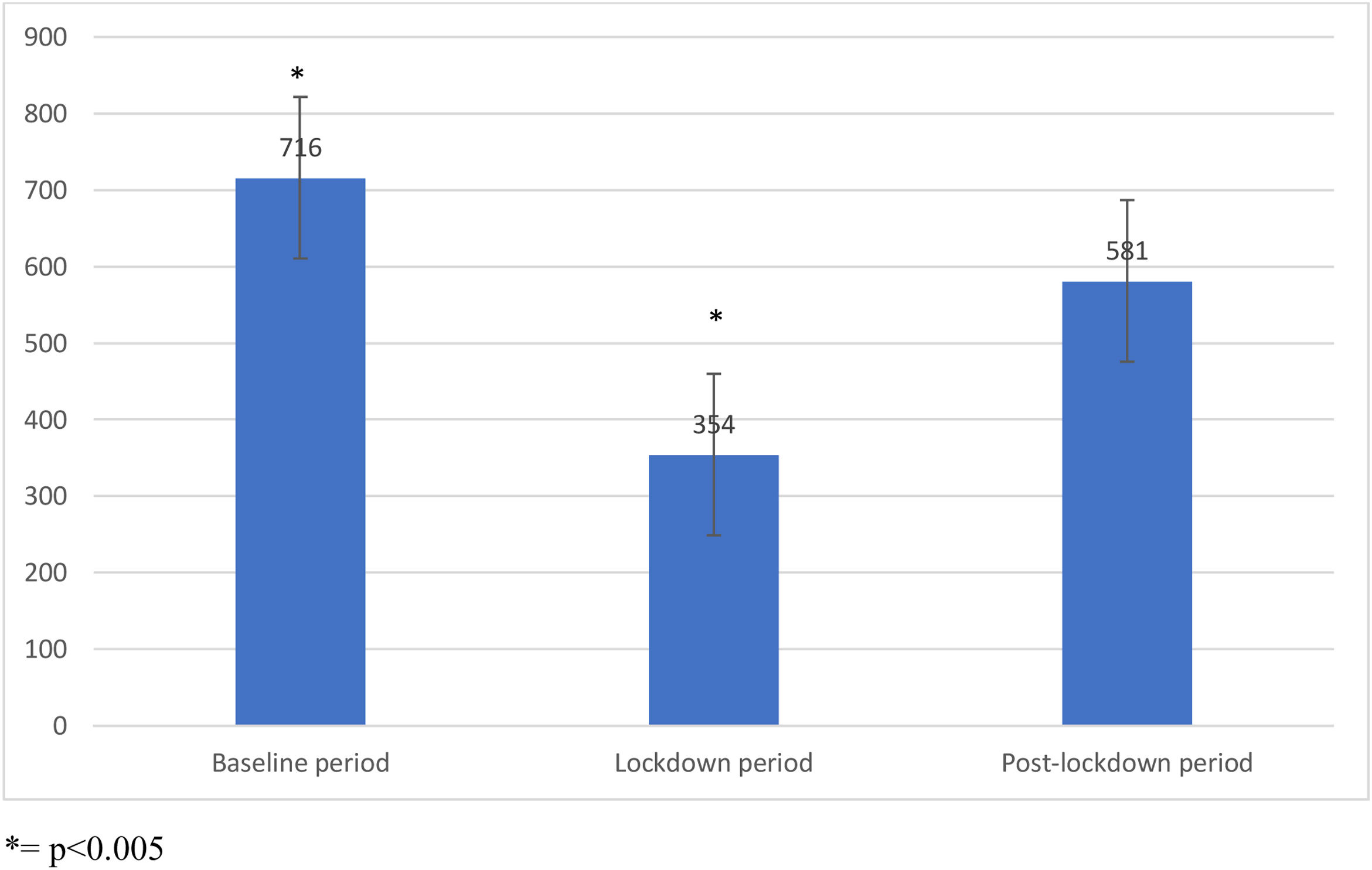
Chart 3 shows the difference in the monthly median surveillance consults in the three periods of time. During the pre-pandemic baseline period, there were 7873 surveillance consults with a monthly median of 716 (560–880). Monthly surveillance consults decreased to a monthly median of 354 (190–470) during lockdown period (p<0.005). However, during post-lockdown period, the number of consults increased up to a monthly median of 581 (450–790), which was not significantly different from the number observed during pre-pandemic period (p=0.12). The proportion of surveillance consults during the post-lockdown period was significantly higher among subjects with a history of high-risk adenomas and remained significantly higher after adjusting for surveillance interval and previous colonoscopy characteristics [OR 1.34 (1.09–1.56)].
Characteristics of users and patients
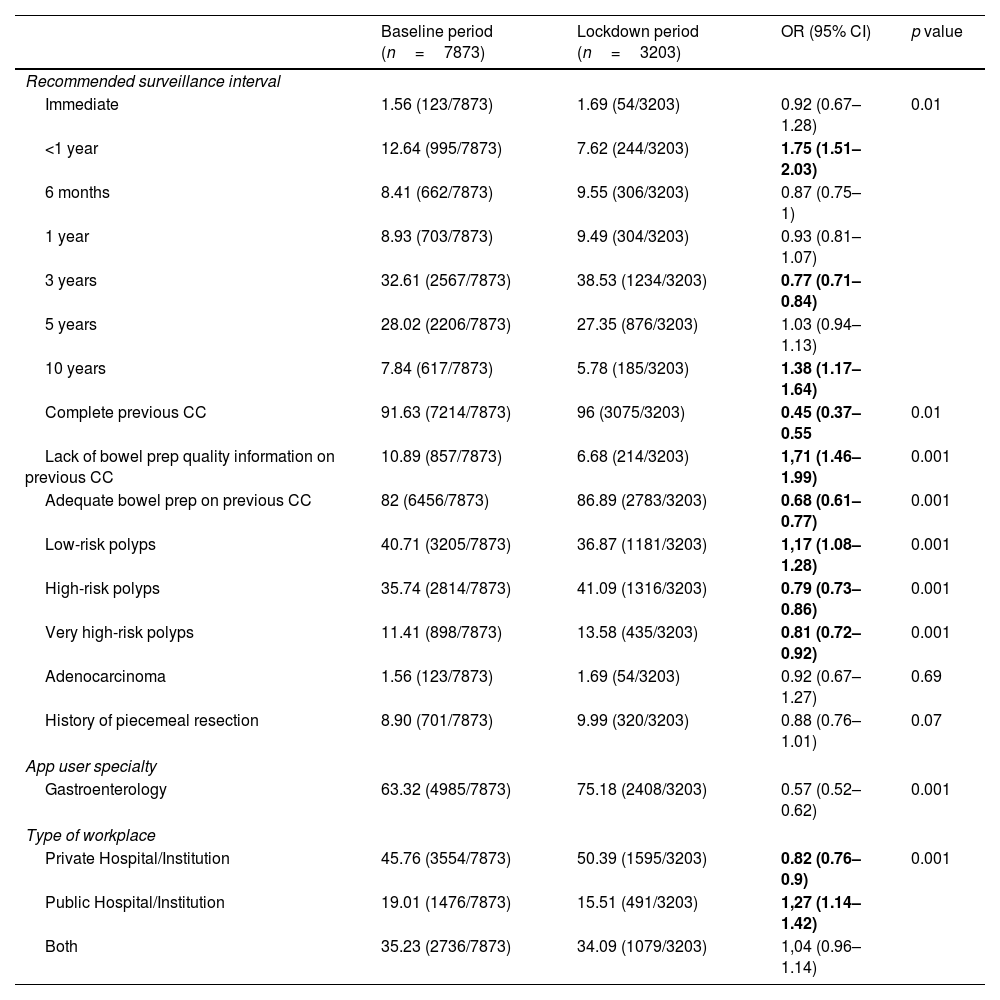
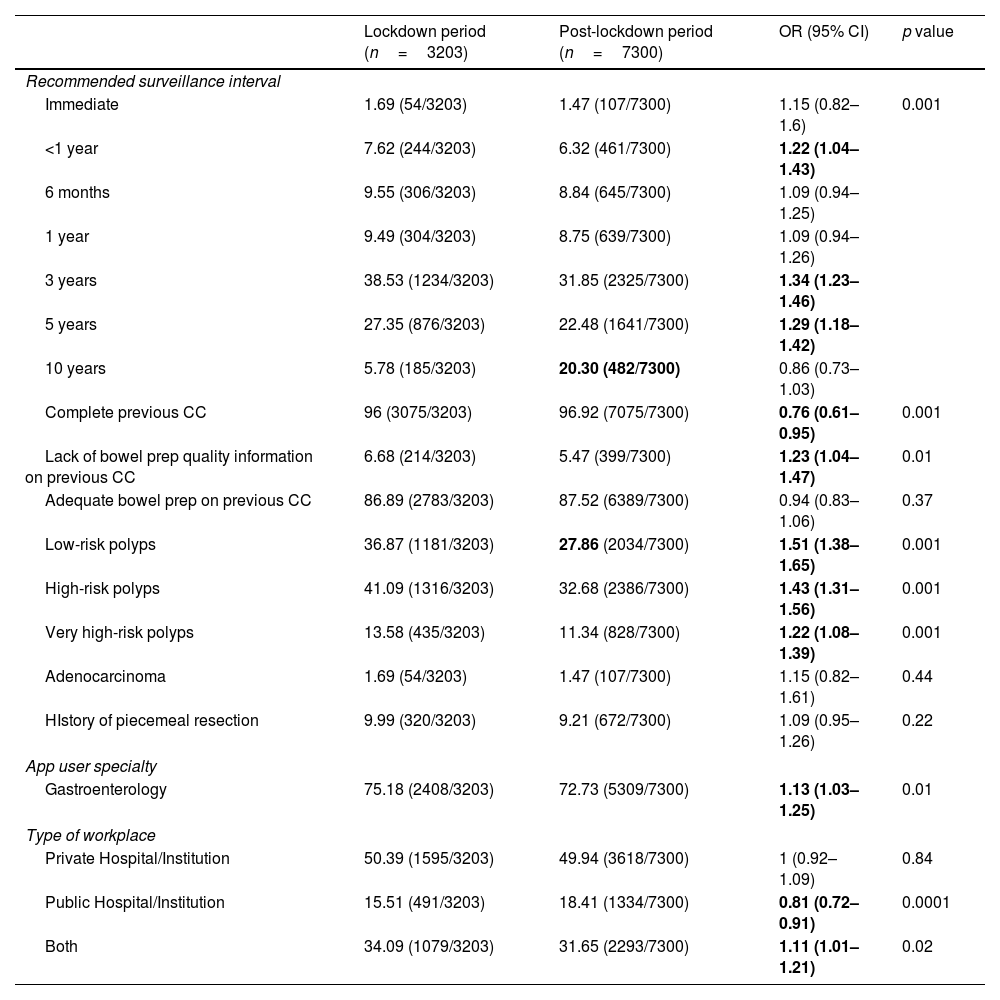
Tables 3 and 4 compares the major features of surveillance consults. Once again, surveillance consults were more frequently performed by gastroenterologists. The proportion of surveillance on subjects with low-risk adenomas significantly decreased during lockdown and during post-lockdown periods (40.7% vs 36.9% vs 27.9% respectively). Consults on subjects with personal history of high-risk adenomas remained stable throughout the study period.
Comparative features of surveillance consultations between baseline and lockdown periods.
| Baseline period (n=7873) | Lockdown period (n=3203) | OR (95% CI) | p value | |
|---|---|---|---|---|
| Recommended surveillance interval | ||||
| Immediate | 1.56 (123/7873) | 1.69 (54/3203) | 0.92 (0.67–1.28) | 0.01 |
| <1 year | 12.64 (995/7873) | 7.62 (244/3203) | 1.75 (1.51–2.03) | |
| 6 months | 8.41 (662/7873) | 9.55 (306/3203) | 0.87 (0.75–1) | |
| 1 year | 8.93 (703/7873) | 9.49 (304/3203) | 0.93 (0.81–1.07) | |
| 3 years | 32.61 (2567/7873) | 38.53 (1234/3203) | 0.77 (0.71–0.84) | |
| 5 years | 28.02 (2206/7873) | 27.35 (876/3203) | 1.03 (0.94–1.13) | |
| 10 years | 7.84 (617/7873) | 5.78 (185/3203) | 1.38 (1.17–1.64) | |
| Complete previous CC | 91.63 (7214/7873) | 96 (3075/3203) | 0.45 (0.37–0.55 | 0.01 |
| Lack of bowel prep quality information on previous CC | 10.89 (857/7873) | 6.68 (214/3203) | 1,71 (1.46–1.99) | 0.001 |
| Adequate bowel prep on previous CC | 82 (6456/7873) | 86.89 (2783/3203) | 0.68 (0.61–0.77) | 0.001 |
| Low-risk polyps | 40.71 (3205/7873) | 36.87 (1181/3203) | 1,17 (1.08–1.28) | 0.001 |
| High-risk polyps | 35.74 (2814/7873) | 41.09 (1316/3203) | 0.79 (0.73–0.86) | 0.001 |
| Very high-risk polyps | 11.41 (898/7873) | 13.58 (435/3203) | 0.81 (0.72–0.92) | 0.001 |
| Adenocarcinoma | 1.56 (123/7873) | 1.69 (54/3203) | 0.92 (0.67–1.27) | 0.69 |
| History of piecemeal resection | 8.90 (701/7873) | 9.99 (320/3203) | 0.88 (0.76–1.01) | 0.07 |
| App user specialty | ||||
| Gastroenterology | 63.32 (4985/7873) | 75.18 (2408/3203) | 0.57 (0.52–0.62) | 0.001 |
| Type of workplace | ||||
| Private Hospital/Institution | 45.76 (3554/7873) | 50.39 (1595/3203) | 0.82 (0.76–0.9) | 0.001 |
| Public Hospital/Institution | 19.01 (1476/7873) | 15.51 (491/3203) | 1,27 (1.14–1.42) | |
| Both | 35.23 (2736/7873) | 34.09 (1079/3203) | 1,04 (0.96–1.14) | |
Bold: Confidence Intervals and Pvalues indicate strong evidence against the Null Hypothesis of no difference, rejecting it.
Comparative features of surveillance consultations between lockdown and post-lockdown periods.
| Lockdown period (n=3203) | Post-lockdown period (n=7300) | OR (95% CI) | p value | |
|---|---|---|---|---|
| Recommended surveillance interval | ||||
| Immediate | 1.69 (54/3203) | 1.47 (107/7300) | 1.15 (0.82–1.6) | 0.001 |
| <1 year | 7.62 (244/3203) | 6.32 (461/7300) | 1.22 (1.04–1.43) | |
| 6 months | 9.55 (306/3203) | 8.84 (645/7300) | 1.09 (0.94–1.25) | |
| 1 year | 9.49 (304/3203) | 8.75 (639/7300) | 1.09 (0.94–1.26) | |
| 3 years | 38.53 (1234/3203) | 31.85 (2325/7300) | 1.34 (1.23–1.46) | |
| 5 years | 27.35 (876/3203) | 22.48 (1641/7300) | 1.29 (1.18–1.42) | |
| 10 years | 5.78 (185/3203) | 20.30 (482/7300) | 0.86 (0.73–1.03) | |
| Complete previous CC | 96 (3075/3203) | 96.92 (7075/7300) | 0.76 (0.61–0.95) | 0.001 |
| Lack of bowel prep quality information on previous CC | 6.68 (214/3203) | 5.47 (399/7300) | 1.23 (1.04–1.47) | 0.01 |
| Adequate bowel prep on previous CC | 86.89 (2783/3203) | 87.52 (6389/7300) | 0.94 (0.83–1.06) | 0.37 |
| Low-risk polyps | 36.87 (1181/3203) | 27.86 (2034/7300) | 1.51 (1.38–1.65) | 0.001 |
| High-risk polyps | 41.09 (1316/3203) | 32.68 (2386/7300) | 1.43 (1.31–1.56) | 0.001 |
| Very high-risk polyps | 13.58 (435/3203) | 11.34 (828/7300) | 1.22 (1.08–1.39) | 0.001 |
| Adenocarcinoma | 1.69 (54/3203) | 1.47 (107/7300) | 1.15 (0.82–1.61) | 0.44 |
| HIstory of piecemeal resection | 9.99 (320/3203) | 9.21 (672/7300) | 1.09 (0.95–1.26) | 0.22 |
| App user specialty | ||||
| Gastroenterology | 75.18 (2408/3203) | 72.73 (5309/7300) | 1.13 (1.03–1.25) | 0.01 |
| Type of workplace | ||||
| Private Hospital/Institution | 50.39 (1595/3203) | 49.94 (3618/7300) | 1 (0.92–1.09) | 0.84 |
| Public Hospital/Institution | 15.51 (491/3203) | 18.41 (1334/7300) | 0.81 (0.72–0.91) | 0.0001 |
| Both | 34.09 (1079/3203) | 31.65 (2293/7300) | 1.11 (1.01–1.21) | 0.02 |
Bold: Confidence Intervals and Pvalues indicate strong evidence against the Null Hypothesis of no difference, rejecting it.
Our results describe the impact on CRC screening and surveillance experienced during the different phases of COVID-19 pandemic when compared to pre-pandemic baseline months. The number of Captyva consults decreased notably during the lockdown months for both screening and surveillance visits when compared to pre-pandemic baseline period. Data shows an increase for both types of consults during 2021, that was greater among surveillance visits than screening visits. The decrease in the number of monthly consults or queries for CRC screening was expected during the lockdown period.14 This has been previously reported for CRC screening and neoplastic screening in general – but previous results are heterogeneous, depending on the country, the type of disease and the type of lockdown implemented. Jidkova et al.15 reported that during shutdown, there was a minor impact on the willingness to adhere to breast cancer screening programme in Netherlands, with a backlog in terms of the number of invitations sent to the population that was easily recovered after shutdown.
As Puricelli Perin et al.16 stated, the impact of the backlog in the screening procedures should be mitigated by means of adaptive use of healthcare resources. A noteworthy finding of our study is that even after the lockdown and after resuming screening activities, the number of queries did not recover to pre-pandemic levels with the median amount of screening consults during 2021 still 33% lower than the number of consults before the pandemic outbreak. This differs from what was observed in other published studies. Vives et al.17 reported a 43% decrease in the number of invitations for CRC screening during 2020 in Catalonia along with a decrease in patients’ adherence to colonoscopy; however, the authors reported a recovery to 2019 levels once screening activities were restarted. We hypothesize that this difference can be mainly related to two situations. First, the strict lockdown period in Argentina was one of the most prolonged in the world.18 This would encourage patients to avoid procedures regarded as “non-urgent”, such as screening colonoscopy. On the other hand, Argentina had a high incidence of COVID-19 despite the strict lockdown.19 This placed unprecedented, high demand on utilization of hospital resources, reducing the available supplies and human resources to maintain less acute medical care, including screening procedures of any type.
It is worth mentioning that Argentina, unlike many countries in the world such as Spain or other Western Europe countries, does not have a unified national programme for CRC screening. The initiative depends on the healthcare physicians who evaluate patients in both public or private healthcare institutions. A majority of the population in Argentina (approximately 60%) relies on public healthcare system, whereas the rest relies on private institutions through private or semi-private healthcare insurances. The latter have developed policies to encourage CRC screening, like campaigns to provide adequate information on the importance of CRC screening as well as the different procedures available for this matter. This is why, even though our study reflects indirect measures of the local CRC screening situation, it is to date the largest study to be performed on CRC screening and surveillance in Argentina. Captyva does not belong nor was developed by a government agency. However, it has been endorsed by the National Cancer Institute and the most relevant local scientific societies. Although it is reasonable that a proportion of consults made could be the result of user's “gaming” with the app, we consider that this bias is completely avoided by the fact that more than 25,000 consults were included for analysis.
Surveillance visits during the 2020 lockdown showed a similar trend to screening visits with a significant decrease when compared to pre-pandemic levels. Nevertheless, we observed a recovery to pre-pandemic numbers during 2021. This finding is replicated in other studies, such as the study published by Walker et al.20 The discrepancy observed in 2021 between the increase in the number of surveillance and screening consults could be explained by the fact that, given the limited healthcare resources (both human and technical) during the 2020 lockdown, there was a logical tendency from both physicians as well as patients to prioritize the performance of colonoscopy in situations with a short-term higher risk of cancer development. This phenomenon follows a logic which can be related to the limited healthcare resources in developing countries.21 Under such circumstances, it seems reasonable that physicians would prioritize colonoscopy access to patients with a history of high-risk colonoscopy adenomas and/or CRC.
ConclusionOur findings show the impact that the COVID-19 pandemic has had in prevention of common neoplastic disease such as CRC. The interruption of screening procedures is inevitably associated with an expected increase in CRC incidence as well as CRC mortality rate. However, the backlog in endoscopic procedures may not be the problem per se, but the time elapsed in the recovery of screening-procedure volume. According to our findings, the number of CRC screening consults registered by Captyva during 2021 – though higher than those reported in 2020 – were still lower than the number of screening consults in 2019.
The implementation of alternative approaches, such as faecal immunochemical test (FIT) could help to curb the negative impact of future healthcare crisis in CRC screening. FIT has shown to have an acceptable diagnostic efficacy and it is an affordable approach.22,23 In addition, patients can perform FIT safely in their homes, avoiding unnecessary exposure to hospital-based procedures. Regardless of the method of choice, it is of utmost importance that CRC screening procedures do not remain unattended. A correct diagnosis of the reasons for screening backlog is fundamental to developing an adequate plan to increase such procedures.
This study has several limitations. First, other factors that were not measured may have exerted some influence in the amount of Captyva consults throughout time; when analyzing the monthly use trends (Chart 1), some spikes in the amount of consults were observed that cannot be explained by COVID-19 pandemic. For example, in July 2019, Captyva was declared as an “element of national interest” by the Senate and this may explain the spike in usage seen. Similarly, in March 2020, Captyva had media coverage in the context of CRC awareness day, which may also explain the spike in usage at that time. We do not have a ready explanation for the spike observed in November 2021. In addition, the number of Captyva consults may not accurately resemble the amount of CRC screening procedures performed in Argentina, so our results should be understood as an indirect measure of CRC screening in Argentina. Nevertheless, it must be highlighted that Captyva was widely accepted before COVID-19 pandemic and its utilization is broadly ongoing to date. Therefore, we believe that the screening consults of Captyva may reflect the changes in screening tendencies suffered throughout the pandemic. Another aspect of our results that should be highlighted is that the majority of consults were made by healthcare professionals in the city of Buenos Aires; hence, the results would not be representative of the situation of the whole country. However, we believe that this may be caused by a characteristic of the Argentinean healthcare system, in which a vast majority of patients – even those living in other cities – seek for healthcare in Buenos Aires. Buenos Aires city and its surroundings concentrate 25% of the country's population and the majority of healthcare resources (human and technological resources) are located in this city. One of the strengths of our study is that Captyva allows to register relevant clinical characteristics of subjects with risk of CRC. That data has been used to assess how of the backlog observed during the pandemic showed differences in basal risk of subjects, as well as the history of colorectal neoplasia and endoscopic findings in the case of surveillance consults. Another relevant strength of our study is that it depicts a real-life clinical scenario: data is derived from anonymous app users distributed throughout our country with heterogeneous backgrounds in terms of specialty and work environment. Real-world evidence has the potential benefit of identifying downsides or flaws of health interventions that controlled trials performed in referral centres may be unable to detect.
In conclusion, we report a major decrease in the number of CRC screening and surveillance consults associated with the COVID-19 pandemic in Captyva – a clinical decision support system widely used in Argentina. A recovery to pre-pandemic volume of surveillance consults was observed during 2021; however, this pattern was not seen in the screening queries. This may reflect a persistent deficit in the number of screening procedures after lockdown that needs to be studied and addressed. This deficit may result in long term consequences, such as delay in colorectal cancer diagnoses, later stage at diagnoses, and potentially poor prognosis.24 Future longitudinal follow-up studies could address these questions.
FundingThis research has not received specific support from public sector agencies, the commercial sector, or non-profit entities.
Conflicts of interestsNone declared.
The following are the supplementary data to this article:

