







Evaluar el valor pronóstico de valores extremos de la N-terminal pro-brain natriuretic peptide (NT-proBNP, «porción amino-terminal de la prohormona del péptido natriurético cerebral») obtenido en cualquier momento de un ingreso por insuficiencia cardíaca (IC).
Materiales y métodosEstudio de cohortes retrospectivo que incluyó pacientes ingresados por IC en un hospital de segundo nivel con al menos un valor de NT-proBNP. Se definieron 2 grupos: pacientes con NT-proBNP extremo (>50.000pg/ml) y pacientes con NT-proBNP elevado (>1.800pg/ml y <20.000pg/ml). El suceso de interés primario fue el compuesto por: 1) muerte intrahospitalaria; 2) reingreso por IC, y 3) muerte a los 6 meses. Se realiza un análisis mediante modelos de supervivencia de Cox.
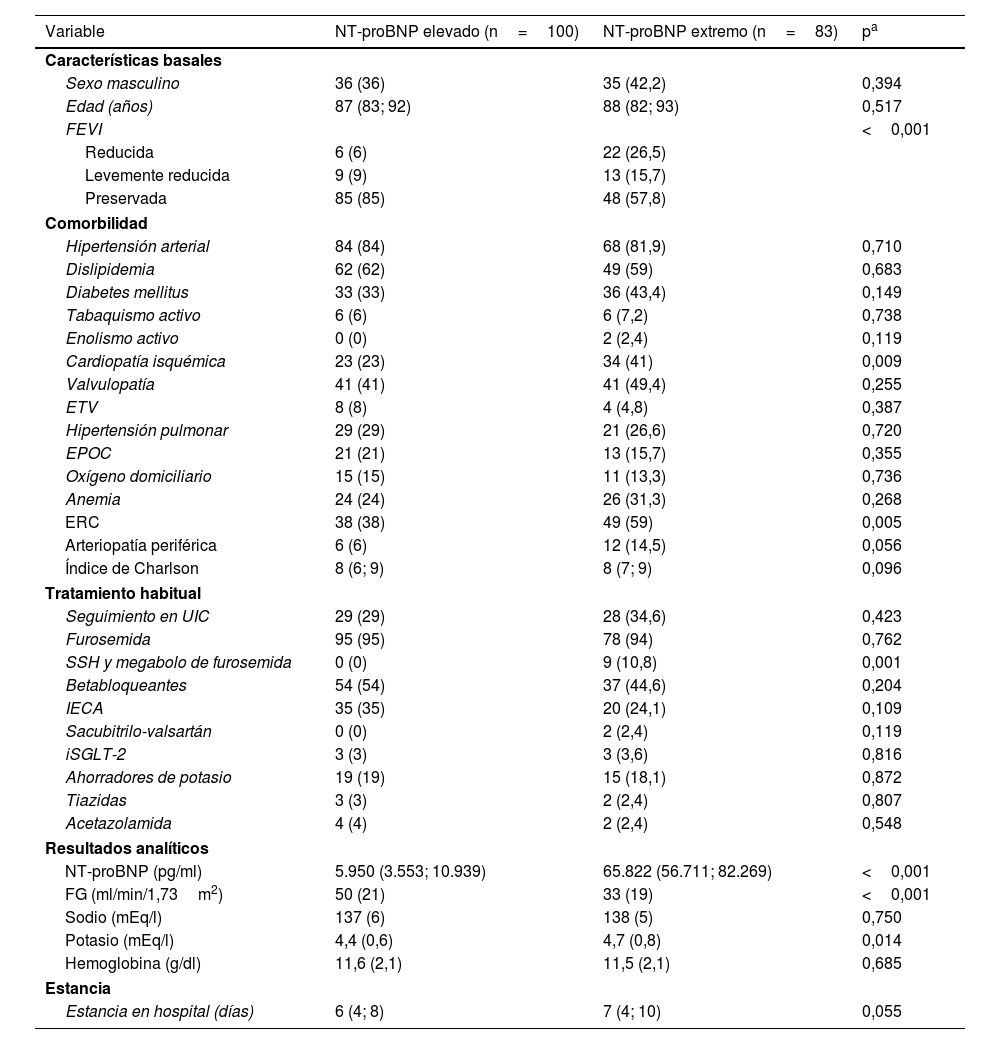
ResultadosSe incluyeron 83 pacientes con NT-proBNP extremo y 100 con NT-proBNP elevado, 61% mujeres, con una edad mediana de 87 años. La comorbilidad fue elevada y similar en ambos grupos (índice de Charlson mediano de 8). El suceso de interés primario fue más frecuente en pacientes con NT-proBNP extremo: 25,02 vs. 10,53 sucesos por cada 100 pacientes y mes (HR 2,07; IC 95%: 1,37, 3,14). Tanto la mortalidad intrahospitalaria como la mortalidad a los 6 meses fueron significativamente mayores en el grupo del NT-proBNP extremo; los reingresos por IC también fueron numéricamente mayores, aunque de manera no significativa. Estos resultados se mantuvieron tras ajuste multivariable.
ConclusionesLos pacientes ingresados por IC con valores de NT-proBNP>50.000pg/ml tienen peor pronóstico que aquellos con NT-proBNP<20.000pg/ml, constituyendo un subgrupo con alta mortalidad a corto plazo.
To evaluate the prognostic value of extreme levels of the N-terminal pro-brain natriuretic peptide (NT-proBNP) measured at any time during hospitalization for heart failure (HF).
Materials and methodsA retrospective cohort study including patients hospitalized for HF in a secondary-level hospital with at least one NT-proBNP measurement. Two groups were defined: patients with extreme NT-proBNP levels (>50,000pg/mL) and those with elevated NT-proBNP levels (>1800pg/mL and <20,000pg/mL). The primary outcome was a composite of (1) in-hospital mortality; (2) HF readmission, and (3) 6-month mortality. Cox survival models were used for analysis.
ResultsA total of 83 patients with extreme NT-proBNP levels and 100 with elevated NT-proBNP levels were included; 61% were women, with a median age of 87 years. Comorbidity burden was high and similar between groups (median Charlson index: 8). The primary outcome was more frequent in patients with extreme NT-proBNP levels: 25.02 vs. 10.53 events per 100 patient-months (HR 2.07; 95% CI: 1.37-3.14). Both in-hospital and 6-month mortality were significantly higher in the extreme NT-proBNP group, while HF readmissions were numerically higher but not statistically significant. These results remained consistent after multivariable adjustment.
ConclusionsPatients hospitalized for HF with NT-proBNP levels>50,000pg/mL have a worse prognosis than those with NT-proBNP<20,000pg/mL, representing a high-risk subgroup with short-term mortality.

