




Editado por: Dr. Calos Cerdán
Cirugía General y Aparato Digestivo. Unidad de Cirugía Digestiva. Hospital Universitario de la Princesa. Madrid
Dr. Matteo Frasson
Cirugía general. Hospital Universitario y Politécnico La Fe. Valencia
Última actualización: Septiembre 2025
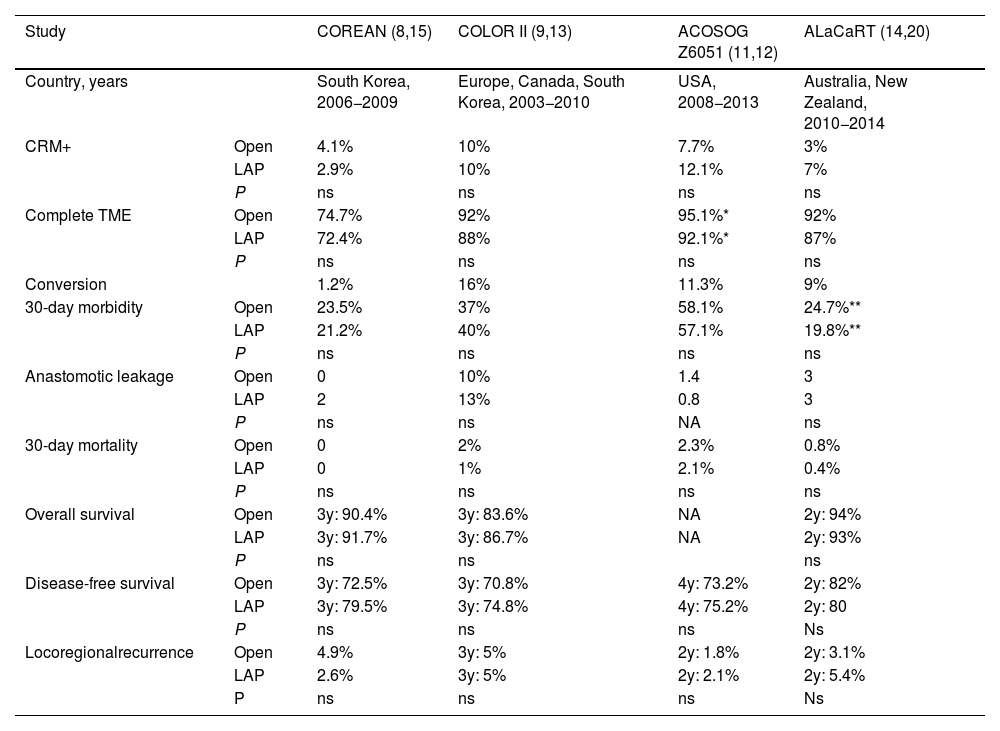
Más datosThe role of laparoscopy in rectal cancer surgery has evolved considerably since the early 2000s. Initial randomized trials, such as COLOR II and COREAN, indicated that laparoscopic approaches offered similar pathological outcomes with better postoperative recovery than open surgery. In contrast, trials like ACOSOG Z6051 and ALaCaRT suggested noninferiority could not be established. Variability in trial outcomes, focusing on either disease-free survival or pathological measures, initially hindered consensus. Long-term analyses have shown no significant difference in disease-free survival between laparoscopic and open approaches. Meta-analyses have reinforced the benefits of laparoscopic surgery, with reduced mortality and similar oncologic effectiveness to open surgery. However, new techniques like transanal TME (TaTME) and robotic approaches have introduced alternatives, though each presents unique challenges, from recurrence rates in TaTME to costs in robotics. While laparoscopy remains the preferred method due to accessibility and outcomes, robotic surgery is expected to gain traction in high-volume centers.
El papel de la laparoscopia en la cirugía del cáncer de recto ha evolucionado considerablemente desde principios de la década de 2000. Los ensayos clínicos iniciales, como COLOR II y COREAN, indicaron que el abordaje laparoscópico ofrecía resultados patológicos similares con una mejor recuperación posoperatoria que la cirugía abierta. Por el contrario, ensayos como ACOSOG Z6051 y ALaCaRT sugirieron que no se podía establecer la no inferioridad. La variabilidad en los resultados de los ensayos, centrados en la supervivencia libre de enfermedad o en medidas patológicas, inicialmente obstaculizó la aceptación de la laparoscopia en cirugía rectal. Los análisis a largo plazo no han mostrado diferencias significativas en la supervivencia libre de enfermedad entre los abordajes laparoscópicos y abiertos. Los metanálisis han reforzado los beneficios de la cirugía laparoscópica, con una mortalidad reducida y una eficacia oncológica similar a la de la cirugía abierta. Sin embargo, nuevas técnicas como Transanal TME (TaTME) y los enfoques robóticos han introducido alternativas, aunque cada una presenta desafíos únicos, desde las tasas de recurrencia en TaTME hasta los costos en robótica. Si bien la laparoscopia sigue actualmente siendo el método preferido en cirugía rectal, debido a su accesibilidad y resultados, se espera que la cirugía robótica gane terreno en los centros con mayor volumen.

