









Treatment of class III malocclusion in growing subjects is a challenging part of contemporary orthodontic practice. Many treatment approaches can be found in the literature regarding orthopedic, orthodontic treatment or even surgery for class III malocclusions. We present a case report of a 12-year-old male patient, skeletal class III who was treated with Edge-Wise appliances. Treatment was successful with the need of neither extractions nor surgery. There was a tooth transposition of a premolar and maxillary canine. We used intermaxillary elastics to correct the anterior crossbite. The objective of this clinical case is to demonstrate the importance of knowledge in the management of the patient at appropriate ages, as well as of the apparatology and auxiliaries in orthodontics for each particular case. Favorable results were obtained, obtaining bilateral class I molar and canine, as well as complete uncrossing of the anterior bite assisted with dental camouflage.
El tratar una maloclusión clase III en pacientes que se encuentran en crecimiento es un gran reto en la práctica ortodóntica contemporánea. Se encuentran varias formas de tratar una maloclusión clase III que incluyen tratamientos ortopédicos, ortodónticos o incluso cirugía ortognática. A continuación se presenta un caso clínico de un paciente de 12 años de edad, clase III dentoesqueletal que se trató con aparatología de ortodoncia Edge-Wise, se trató el caso sin extracciones y sin cirugía ortognática. Se realizó la transposición de primer premolar con canino superior derecho, y se implementó el uso de elásticos intermaxilares para el descruzamiento de mordida anterior. El objeto de la presentación de este caso clínico es demostrar la importancia del conocimiento en el manejo del paciente a edades oportunas, así mismo de la aparatología y auxiliares dentro de la ortodoncia aplicable a cada caso particular. Se obtuvieron resultados favorables, obteniendo una clase I molar y canina bilaterales, así como el descruzamiento completo de la mordida anterior auxiliada con camuflaje dental.
Malocclusion, in spite of being a multifactorial condition, in almost all cases is not due to a syndrome or pathological process but to an alteration of growth and development. However, in certain cases it is possible to identify a specific cause that produces the condition. Heredity plays an important role in the development of malocclusion.1
It should be considered that some of the factors associated with malocclusion are the persistence of the deciduous incisors, which cause the eruption of the permanent teeth towards lingual thus producing an edge-to-edge occlusion and by accommodation the patient protrudes the mandible to occlude, producing a pseudo-class III which will subsequently be defined as a true class III or a compensation. Also known as etiological factors are bad mandibular posture habits, oral breathing, tongue malposition and genetic factors.2
Orthodontic camouflage began to develop in the years 1930-1940. Camouflage treatment is the displacement of the teeth in relation to its supporting tissues to compensate for a maxillomandibular discrepancy.3 From 1930, treatments involving dental camouflage in orthodontics began. In a class III malocclusion compensation upper incisor proclination and lower incisor retroclination is performed.4
DIAGNOSIS AND TREATMENTThe treatment of crossbites in patients with primary or mixed dentition consists in the elimination of etiologic factors as soon as possible to allow growth of the maxilla then continue the stimulation to promote occlusion stability and correct function.5
Interceptive treatment mainly involves the prevention of progressive and irreversible changes of the soft or bony tissues. When the anterior crossbite is not corrected it may produce abnormal attrition of the lower incisors leaving a very thin labial alveolar bone or gingival recessions.6 When an intraoral examination of the patient was made, a functional deviation was detected thus indicating that the nature of the malocclusion was of dental origin. Crossbites with functional displacement must be corrected as soon as they are detected.
CASE REPORTA male patient of 12 years 8 months of age attended the Orthodontics Clinic of the Division of Postgraduate Studies and Research in the Faculty of Dentistry of the National Autonomous University of Mexico (UNAM). The patient's reason for consultation was to «fix his teeth». He referred no pathologic data however on his father's family there was a history of prognathism.
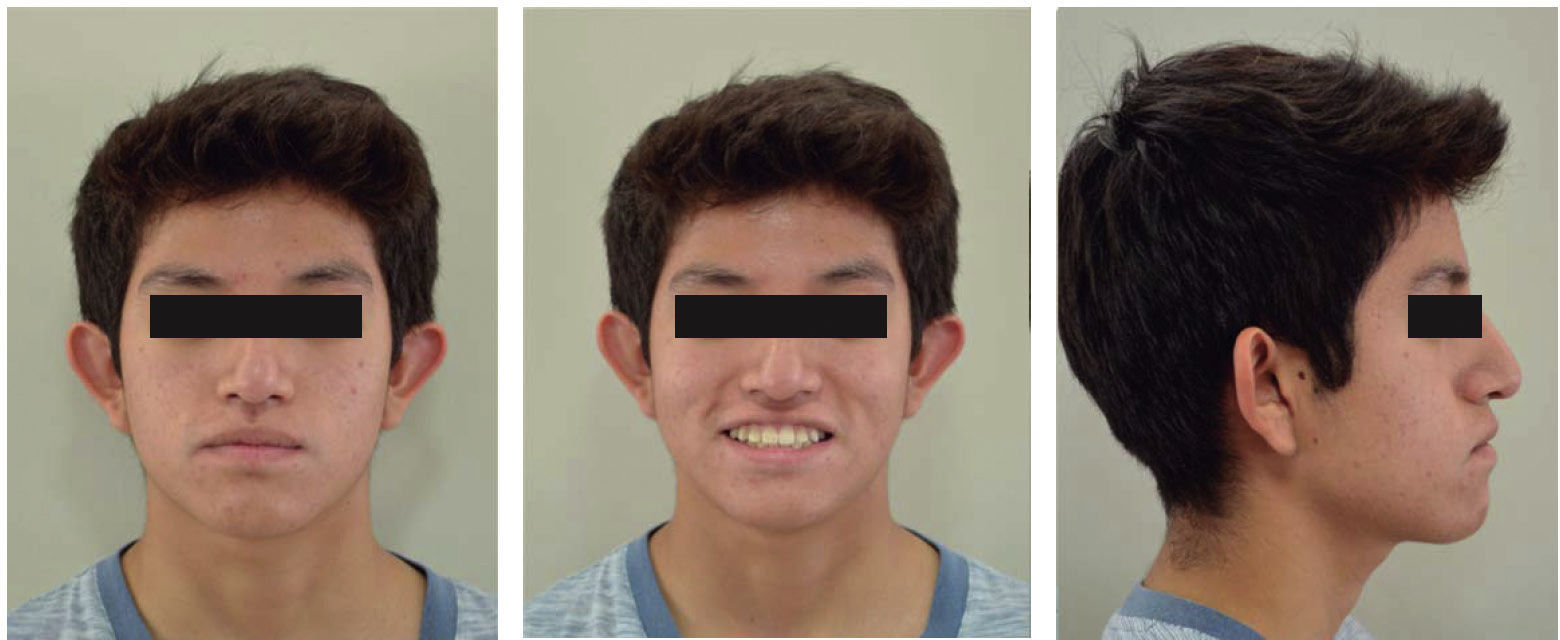
An extraoral examination was performed, revealing a dolichocephalic patient, with an increase in proportion of the middle third (37.7%), as well as a capillary normal insertion, normally inserted auricular pavilions, a straight facial profile with a straight nose and presence of the mentolabial fold. On the basis of the Ricketts aesthetic line upper retrocheilia was noted (Figure 1).

Regarding the arches, the presence of tooth #53 was observed, rotation of teeth #14, 11, 21, 22, 24 and 25; the upper left lateral incisor was palatally displaced and canines were in supra-occlusion. With regard to the lower arch tooth #37 was rotated and the presence of macroglossia was observed (Figure 2). From a sagittal plane, there was an anterior cross bite with a 5.5-mm overbite and an overjet of -3mm. In the models analysis the patient presented a negative tooth-bone discrepancy in the upper arch (Figure 3).


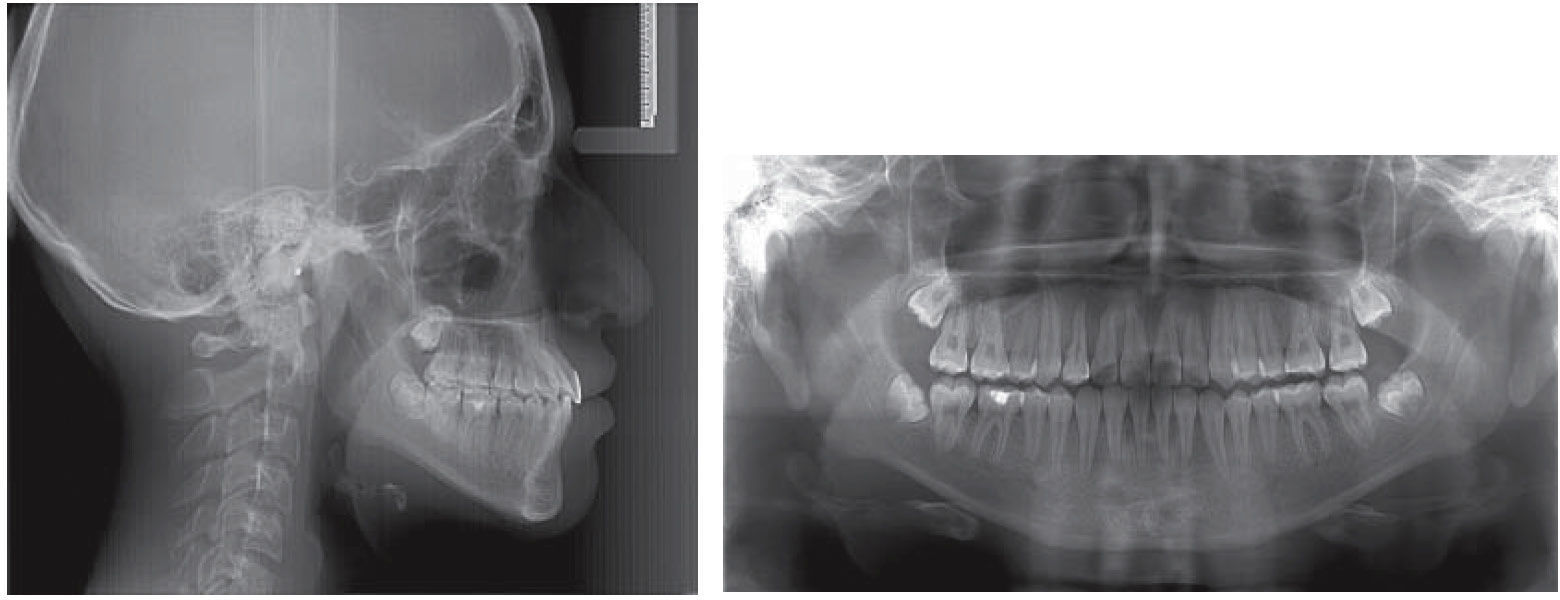
The patient had an angle molar class III and a non-assessable canine class relationship (Figure 4). A growth analysis was performed on a hand-wrist radiograph that revealed a 4th growth stadium thus indicating a peak in the patient's growth.

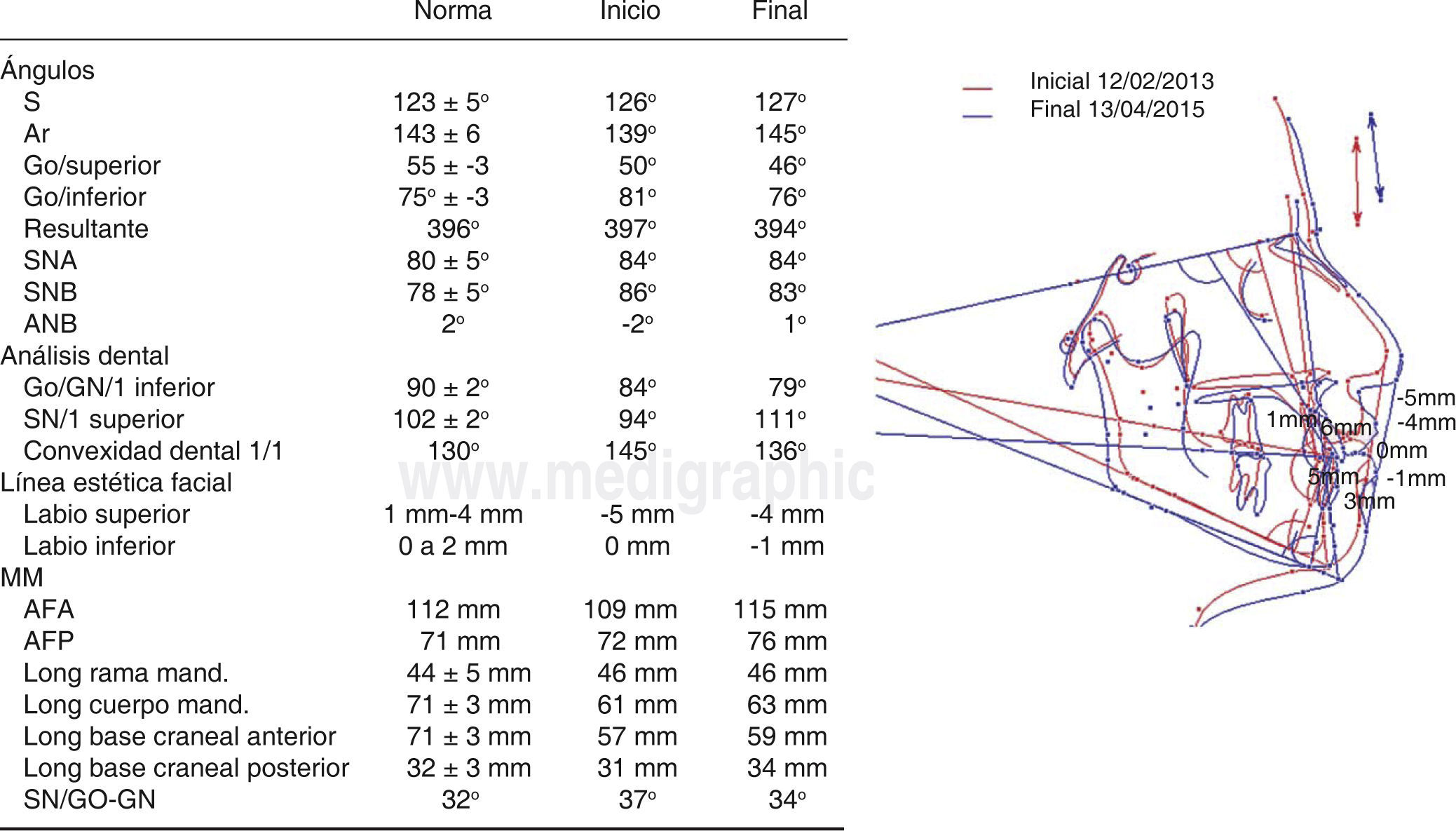
Jarabak, Steiner, Ricketts, Downs, McNamara, and UNAM cephalometric analysis were conducted. Some of the data obtained were: SNA; 84, SNB; 86, ANB, -2 degrees thus indicating a class III patient due to prognathism. A mandibular plane/SN of 37 degrees was shown indicating a hyperdivergent patient; GoGN/L1: 84; SN/U1: 94 degrees, reflecting dental retroclination (Figure 5). The diagnosis was a dentoskeletal class III patient due to prognathism, vertical growth, straight profile with upper retrocheilia, upper and lower incisor retroclination, increased overbite, negative overjet and maxillary canines in supraocclusion.
Treatment goals
The facial aim was to improve the profile and lip position. Regarding the functional aspect, the goal was to maintain TMJ health. In the dental goals, the following were included: correct the anterior crossbite, achieve class I molar and canine relationship, correct dental rotations and inclinations, correct the dental midlines, decrease the overbite, obtain arch coordination and maintain the results.
Treatment planGiven the patient's background, an Edge-Wise orthodontic treatment was performed, in which phase I involved: leveling and alignment with 0.012”, 0.014” and 0.016” NiTi upper and lower archwires. Phase II consisted in: correcting the cross bite using a 0.016” x 0.16” SS archwire with class III intermaxillary elastics and occlusal stops. Phase III involved midline correction with the use of crossed elastics and interproximal stripping. Finally, phase IV consisted in: re-leveling (with brackets), ideal archwires and retention.
RESULTSTreatment was finished, restoring full functionality to the patient and correcting the crossbite completely. Likewise, a normal overbite was obtained (Figure 6). Functional movements such as a canine guidance and movements of protrusion and posterior disocclusion were restored. The skeletal class III of the patient was camouflaged by proclining the upper incisors and retroclining the lower. Compensation of the skeletal class III was also favored by the use of class III intermaxillary elastics producing a downward and backwards rotation of the mandible thus obtaining a final SNB of 83 degrees.

A transposition of the upper right canine and the upper right first bicuspid was performed successfully. A class I molar and canine relationship (replacing the tooth #13 by tooth #14) were achieved (Figure 6) in the final panoramic radiograph a good root parallelism may be observed (Figure 7). The patient at the end of treatment had a harmonious profile (Figure 8). An Essix-type retainer was placed on the lower arch due to hygiene issues and in the upper arch, a circumferential retainer was indicated.
DISCUSSION

The goals were achieved successfully, restoring a functional occlusion, correcting completely the anterior crossbite by means of a mandibular rotation through the use of occlusal stops and intermaxillary elastics.
The use of a facial mask may protrude the maxilla in patients 8 years of age or younger. The age limit to obtain favorable outcomes is 10 years of age.7 In patients older than 10 years the expected orthopedic result is almost none, obtaining only tooth movement so in this case, it was decided not to use facial mask.
It is important to distinguish between a case with orthodontic limitations, that is, between a skeletal class III patient in whom an orthodontic camouflage may be performed and one in which the only treatment option is orthognathic surgery. There are certain soft tissue limits in a treatment of orthodontic camouflage. The camouflage treatment is the dental displacement in conjunction with its supporting tissues to compensate for a maxillomandibular discrepancy.2
The treatment must be planned adequately, based on the required orthodontic movements, the stability of the produced changes and if the likely aesthetic result is going to be acceptable according to the patient's expectations.
In this case our patient showed a discrepancy between maxilla and mandible of -2 degrees (ANB). The advantage of this particular case is that the upper incisor with respect to the cranial base had an angle of 94 degrees which allowed us to procline it more while the lower presented a IMPA of 84 degrees, which also allowed us a slight retroclination thus correcting this way the anterior crossbite (Figure 9).
; cephalometric superimposition.")
The use of class III elastics in stages of maximum growth provides very favorable results for the patient. In this case there was a downwards and backwards mandibular rotation, modifying point B. The patient's cooperation in the treatment is essential: using the elastics the hours and the shape that the doctor indicates.
Transposition is a rare type of ectopia in which two adjacent teeth change position in the arch. The transposition may be complete, with both the tooth crown and root transpositioned and parallel; or incomplete, with a trans positioned crown and the root apices in a relatively normal position.8,9 The prevalence of transpositions in the general population is 0.4%,10,11 and are more frequent in the maxilla and unilateral.11–14 Root resorption of both trans positioned teeth has been reported when tried to be moved to their corresponding place in the arch, as well as resorption of the buccal cortex.15 The transposition was performed according to the fact that initially, the upper right cuspid was in a distal position relative to the upper right first bicuspid, so it was decided to bring the canine to the place of the premolar and mesialize the premolar. If we had tried to move the canine to its correct location in the arch, a reabsorption of the buccal cortical may have occurred. The shift in the teeth position was performed in order to achieve stability. This kind of treatment is commonly performed in cases of anomaly of tooth positions as it was in this present case.
At the end of treatment, a correct dental intercuspation, compensation in dental inclinations, a normal overjet and overbite, as well as a molar and canine class I were obtained (Figure 10).
CONCLUSIONS
It is important to determine the ideal time to treat a class III malocclusion, since treatment options vary depending on the age of the patient and the severity of the malocclusion. It is necessary to perform an individualized diagnosis and treatment plan. This case report shows that a patient treated in not-too-late stages, that is, at his growth peak, obtained quite favorable results and in some cases, it may even be possible to avoid surgical procedures at more advanced ages.
In cases where a dental compensation will be performed with the use of intermaxillary elastics or any removable device, it is very important to have complete patient cooperation in order to obtain favorable results. Likewise, it is of the utmost importance that growing patients are monitored through their growth and undergo a post-treatment control over the years.