












A clinical case of a ten-year-old female patient is hereby presented. She had multiple dental inclusions (#13, 11, 23, 33, 34) as well as the maxillary right canine out of its eruption place: it was in the place of the maxillary right central incisor. Teeth #12 and 22 were abnormally shaped. It was chosen to perform orthodontic treatment with extraction of teeth #11, 23, 33 and pull the maxillary right canine in place of the maxillary right central incisor, maintaining both temporary teeth #53 and 63. A correct functional-occlusion was achieved with anterior guidance and group function at laterality movements.
Caso clínico de paciente femenino de 10 años de edad que presenta varias inclusiones dentales OD 13, 11, 23, 33, 34, entre los cuales el OD 13 se encuentra fuera de su sitio de erupción en la zona anterior del maxilar a nivel del OD 11. Los OD 12 y 22 pre- sentan anomalía de forma. Se realiza tratamiento ortodóntico con extracción de OD 11, 23, 33, y tracción del OD 13 en posición del OD 11, conservando los órganos dentarios temporales 53 y 63. Se logró obtener una adecuada oclusión funcional con guía anterior y función de grupo en movimientos de lateralidad.
Dental transposition occurs when a permanent tooth develops in the position that should be occupied by another tooth. The term transposition is commonly used to define a position exchange of two teeth within the same quadrant of the dental arch.
It is classified in: incomplete when one of the two structures (crown or root) is in its original position and complete when both crown and root of the tooth are in the position of another tooth of the same quadrant.1
The etiology of dental transposition is unknown; however several factors have been associated with the development of this anomaly such as: genetic factors, exchange of position of the dental germ, retention of primary teeth, deviated eruption path, abnormality of the eruption sequence, mechanical interference, trauma and early loss of primary teeth.2
With regard to incidence, it has been reported more commonly in women than in men, showing more frequency in the maxillary arch than in the mandibular. Unilateral transpositions have prevalence over the bilateral ones with the left side being the most common side. The predominant transpositions are the ones in which the maxillary canines are involved; the maxillary canine in place of the first premolar comprises 71 per cent of the reported cases.3
DIAGNOSISA female patient of 10 years of age attended the Orthodontics clinic of the Division of Postgraduate Studies and Research of the UNAM due to a lack of eruption of the upper right central incisor, multiple dental inclusions and dental transposition of the tooth #13 in place of the 11. Pathological hereditary and personal information was denied. She was diagnosed as an apparently healthy patient.
Clinical evaluation- a)
Frontal facial analysis
Brachycephalic patient with square-shaped symmetrical face, parallel sub nasal and commissural planes, competent lips, slightly wider interalar distance than the intercanthal, downward direction of the lip commissures at rest.
- b)
Facial profile analysis
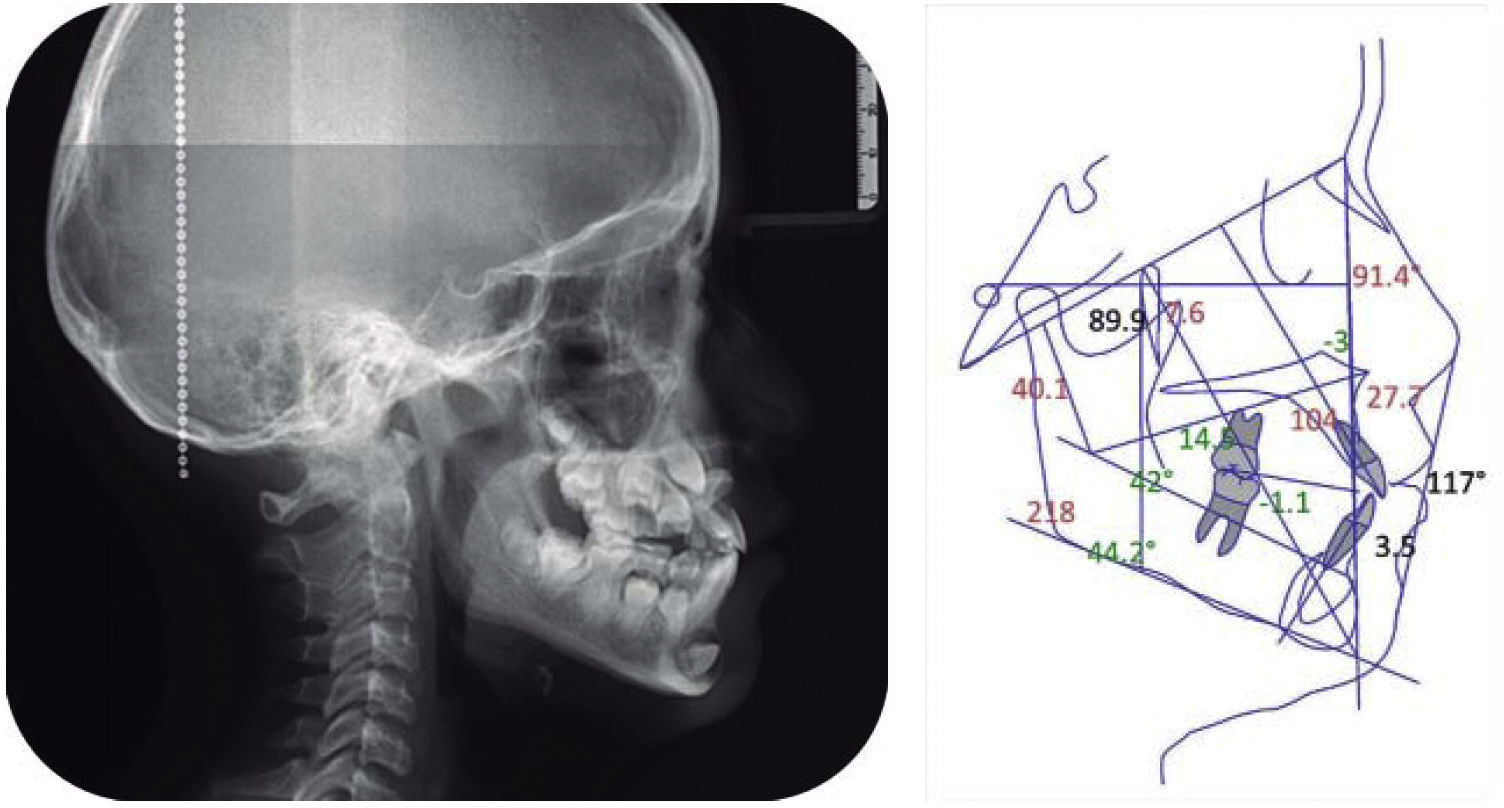
Straight profile with slight malar depression, straight nasal dorsum, depressed paranasal area, 90ª nasolabial angle, negative labial step, deep mentholabial fold and competent lips (Figure 1).
- c)
Intraoral features
Mixed dentition with clinical absence of teeth #11, 23, 33, 43. The patient presented temporary canines (53, 63, 73) and a shape abnormality of the teeth #12 and 22. Bilateral molar class I and non-assessable canine class. Arch form was ovoid. The overjet was 2mm and the overbite, 1mm (Figure 2).
- d)
Ortopantomography
Multiple included dental organs were observed. Tooth #11 was retained with an eruption direction towards the root apex, tooth #13 was impacted between teeth #11 and 12; tooth #23 was found at the level of the root apex of tooth #12, #33 was retained in a horizontal position at the level of the root apices of the incisors and #34 was in a horizontal position with the crown impacted on the crown of #35 (Figure 3).
- e)
Cephalometric analysis



Cephalometric diagnosis showed a skeletal class I, biprotrusive, brachyfacial with upper and lower dental proclination (Figure 4).
Treatment goals
Cephalometric:
- •
To maintain skeletal class.
- •
To improve the axial axis of the teeth.
Facial:
- •
Maintain profile.
Dental:
- •
Maintain molar class I.
- •
Tooth # 13 will remain in position of the #11.
- •
To correct overbite and overjet.
- •
To correct upper dental midline.
Roth 0.022 system.
Surgical removal of tooth #33.
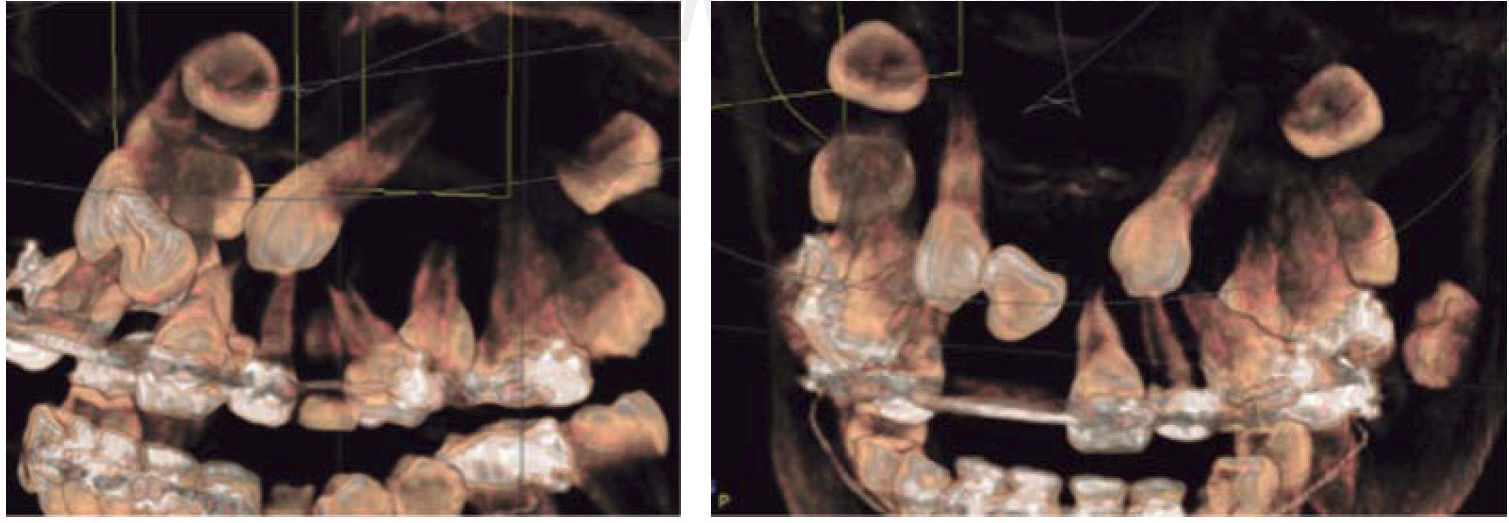
Phase I: leveling and alignment was conducted with 0.014” to 0.016” SS utility arch wires and NiTi open- coil to create space for tooth #11. Bands with double tubes were placed on upper 6's and single tubes on the lower. Once space was obtained for tooth #11, the patient was referred to the Department of Surgery for assessing the dental organs #11, 13 and 23. To that end a Cone beam CT scan was obtained (Figure 5) to serve as diagnosis auxiliary.

Extraction of teeth #11 and 23 was performed because #11 had no root at all and #23 was at the level of the apex of #22. A button was placed in #13 for traction to the place of #11, since it was between #12 and 11 (Figure 6).
Treatment progress
Traction of tooth #13 in the place of #11 was begun, maintaining teeth #53, 63, and 73 in the arch.
The case was re-assessed and removal of OD 73 was decided to obtain a normal overbite (Figure 7).

Retraction of the lower anterior segment was performed with a DKL arch wire and in the upper arch; an expansion arch wire was placed. Brackets were placed in teeth #53 and 63 to align them and improve arch form (Figure 8).
Treatment results
Treatment time was 51 months. The upper right canine was successfully placed in the arch, a normal overjet and overbite was achieved, teeth #53 and 63 were aligned and maintained in the arch for their eventual prosthetic rehabilitation (Figure 9). A functional occlusion was obtained with group function during left and right lateral movements (Figure 10).


Facially, the profile was maintained, upper lip projection was improved and a positive smile was obtained (Figure 11).

Upper and lower circumferential retainers were placed (Figure 12).

The patient was then referred to the Advanced Restorative Dentistry Department for prosthetic assessment of the upper anterior segment.
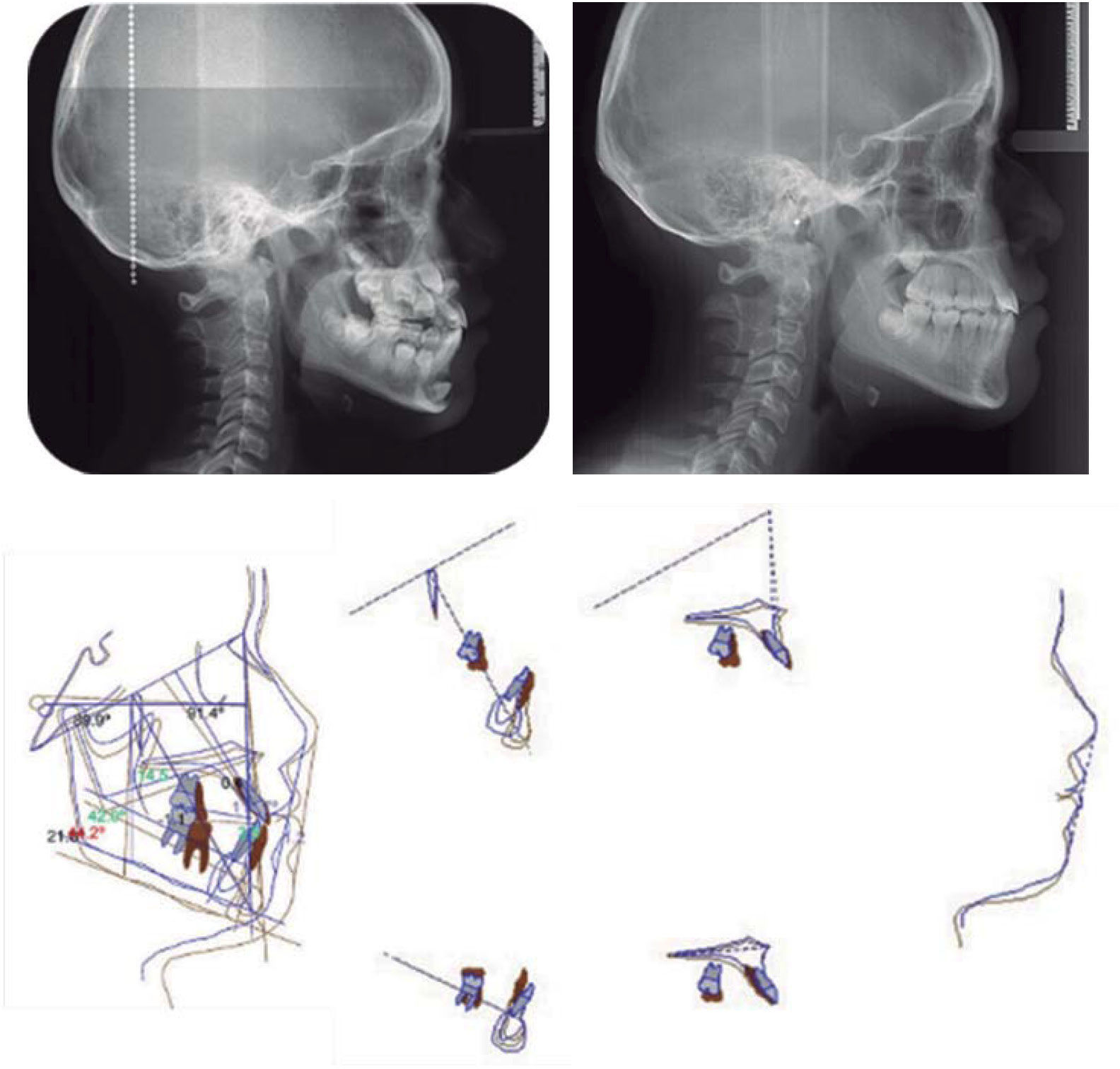
Cephalometrically, the skeletal class remained and there was a slight increase in the upper dental proclination (Figure 13).
DISCUSSION
There are few cases reported in regard to dental transposition, since its incidence is 0.4%. The maxillary canine is the one involved in 71% of cases.4
The etiology of dental transposition remains unknown, but associated factors have been reported: genetic factors, injuries, early loss of temporary teeth, abnormalities of the sequence of eruption and mechanical interferences.
Peck and Peck5 examined 77 publications of dental transposition in which only 4 cases (2%) was the canine in the place of the central incisor. Shapira and Kuftinec suggested that the transposition of the canine and the central incisor must be classified as an ectopic eruption.4
There are several options as treatment alternatives for dental transpositions. Among them we have the alignment of the dental organ in the transposed position, the removal of transposed tooth and orthodontic movement to place them in their normal position. The decision of treatment will depend on the position and the conditions of the transposed teeth.6,7
In this case, it was decided to place tooth #13, which was transposed, in place of tooth #11, which was removed due to the fact that its conditions were less favorable since it presented no root.
CONCLUSIONEarly detection of dental inclusions provides better alternatives for treatment and allows it to be more conservative, whether it is by positioning the included tooth in the arch or by extracting it if its position is not favorable thus preventing damage to adjacent teeth or the formation of cysts.
Dental transposition is a good alternative for the treatment of included teeth that are in a position away from their original site, allowing us to preserve the largest number of teeth on the arch.