





The Airway Management section of the Spanish Society of Anesthesiology, Resuscitation, and Pain Therapy (SEDAR), the Spanish Society of Emergency Medicine (SEMES), and the Spanish Society of Otorhinolaryngology and Head and Neck Surgery (SEORL-CCC) present the Guide for the comprehensive management of difficult airway in adult patients. Its principles are focused on the human factor, cognitive processes for decision-making in critical situations, and optimization in the progression of strategies application to preserve adequate alveolar oxygenation in order to enhance safety and the quality of care. The document provides evidence-based recommendations, theoretical-educational tools, and implementation tools, mainly cognitive aids, applicable to airway management in the fields of anesthesiology, critical care, emergencies, and prehospital medicine. For this purpose, an extensive literature search was conducted following PRISMA-R guidelines and was analyzed using the GRADE methodology. Recommendations were formulated according to the GRADE methodology. Recommendations for sections with low-quality evidence were based on expert opinion through consensus reached via a Delphi questionnaire.
La sección de Vía Aérea de la Sociedad Española De Anestesiología, Reanimación y Terapéutica del Dolor (SEDAR), la Sociedad Española de Medicina de Urgencias y Emergencias (SEMES) y la Sociedad Española de Otorrinolaringología y Cirugía de Cabeza y Cuello (SEORL-CCC) presentan la Guía para el manejo integral de la vía aérea difícil en el paciente adulto. Sus principios están focalizados en el factor humano, los procesos cognitivos para la toma de decisiones en situaciones críticas y la optimización en la progresión de la aplicación de estrategias para preservar una adecuada oxigenación alveolar con el objeto de mejorar la seguridad y la calidad asistencial. El documento proporciona recomendaciones basadas en la evidencia científica actual, herramientas teórico-educativas y herramientas de implementación, fundamentalmente ayudas cognitivas, aplicables al tratamiento de la vía aérea en el campo de la anestesiología, cuidados críticos, urgencias y medicina prehospitalaria. Para ello se realizó una amplia búsqueda bibliográfica según las directrices PRISMA-R y se analizó utilizando la metodología GRADE. Las recomendaciones se formularon de acuerdo con la metodología GRADE. Las recomendaciones de aquellas secciones con evidencia de baja calidad se basaron en la opinión de expertos mediante consenso alcanzado a través de un cuestionario Delphi.
Awake management is the preferred option for securing the known or anticipated difficult airway (DAW) (expert statement [E.S.] 85.7%)1 because it (1) preserves airway (AW) patency and spontaneous ventilation, increases respiratory reserve, and confers protection against aspiration by preserving laryngeal reflexes,1,2 (2) allows a gradual transition to positive pressure ventilation (PPV) and a slow induction of general anaesthesia (GA) given the risk for haemodynamic collapse,3,4 (3) facilitates the procedure, because it inhibits soft tissue collapse, dilates peritracheal structures, allows for better location of the glottis by preventing the larynx from taking a more anterior position, and allows visualisation of air bubbles in the case of distorted anatomy, (4) allows the patient to remain in a sitting position, and cooperate, and enables assessment of their neurological status, and (5) allows all treatment options to remain open and decisions to be made according to the findings.1,5–8
A known or anticipated DAW requires a team-based strategy with thorough multidisciplinary discussion of sequential plans (primary and alternative) to achieve oxygenation, ventilation, and protection against aspiration.1,7,9,10
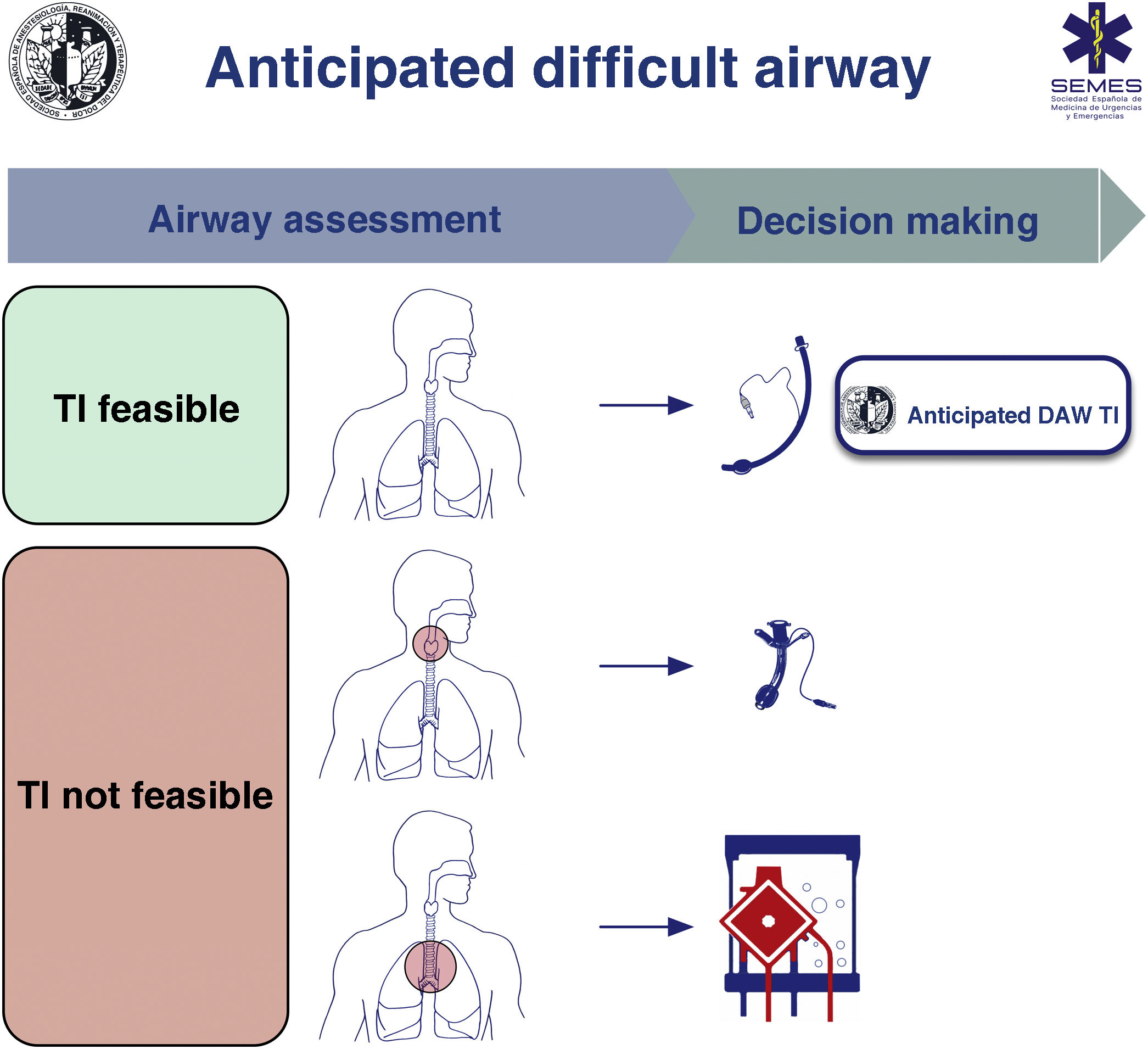
Safe management of DAW secondary to obstructive disease requires consideration of respiratory status, cause, location, and degree of obstruction (greater or less than 50%) through clinical signs and symptoms, imaging, and fibronasolaryngoscopy (FNL).1,7,10,11 The risks and benefits of each approach should be carefully considered and the decision agreed by the medical and surgical team.1Fig. 1 shows a cognitive decision aid for the treatment of an anticipated DAW. The lower plans act as rescue strategies in the event of failure of the upper plan, which should be selected as the primary plan. Awake AW management is recommended in all cases. (1) Supraglottic lesions causing mild obstruction that can be overcome with an endotracheal tube (ETT) allow tracheal intubation (TI), usually with fibrobronchoscopy (FOB). (2) Obstructive supraglottic lesions with stenosis greater than 50% (or with inspiratory stridor at rest 50%),7 non-obstructive supraglottic lesions that prevent TI (or associate TI with unacceptable morbidity), and glottic or subglottic lesions make tracheostomy or cricothyrotomy advisable as the primary approach.10 (3) Lower tracheal obstructive lesions not salvageable with an ETT or tracheal cannula require extracorporeal membrane oxygenation (ECMO).10

Active oxygenation strategies should be implemented throughout the procedure. High-flow nasal oxygen therapy (HFNO), although it requires further validation in this setting, may be the technique of choice. HFNO is recommended over conventional low-flow nasal cannula (E.S. 91.4%).
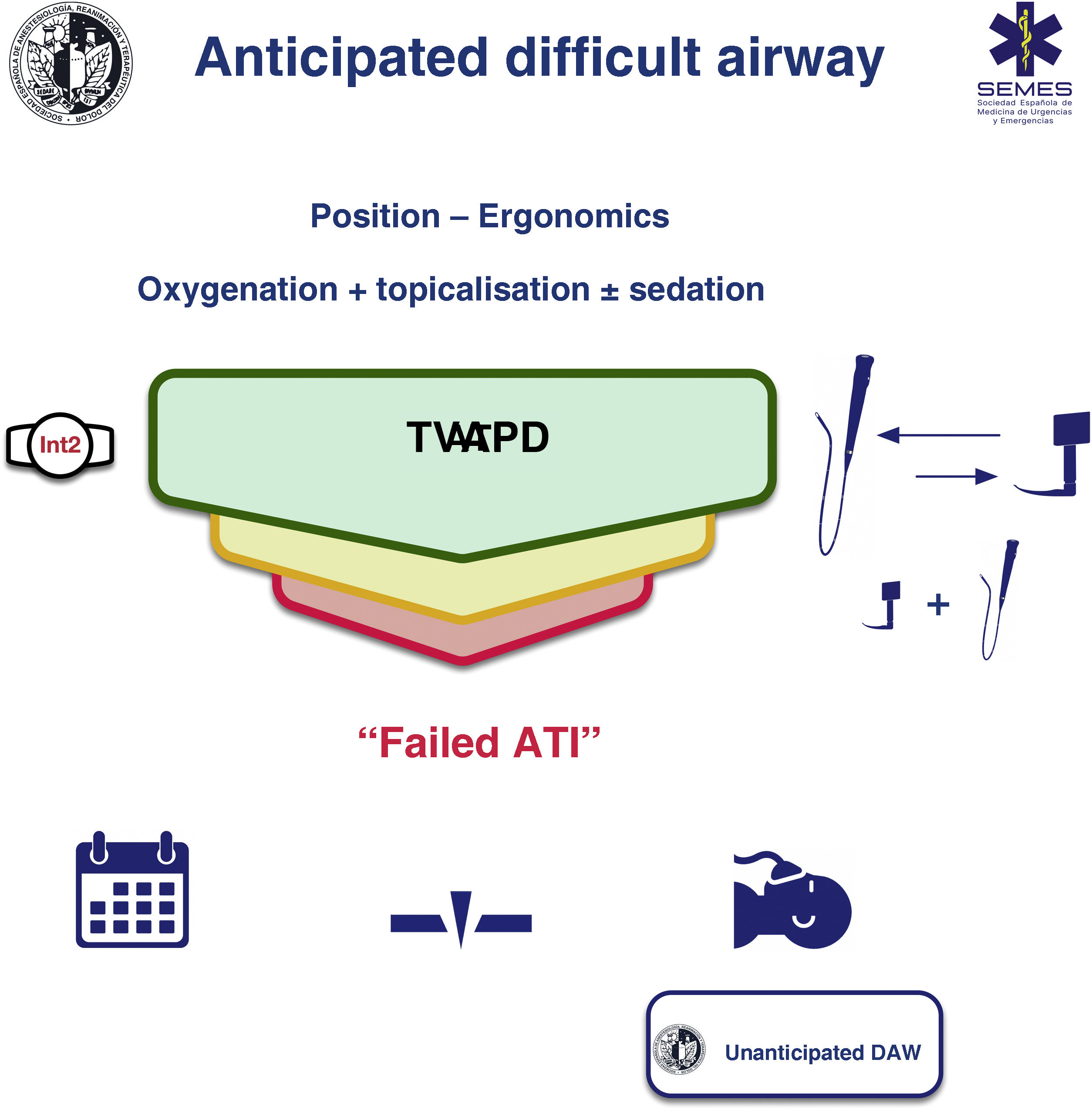
Awake tracheal intubationWhen it is feasible to secure the AW non-invasively, awake TI is still the gold standard for DAW management3,12,13 because it is safe and reliable.14,15 Four elements are critical to the success of the procedure: continuous oxygenation, topicalization of AW, sedation (optional), and selection, experience, and appropriate management of the TI device and technique. The ideal protocol in terms of efficacy and safety is unknown, and therefore the most appropriate protocol must be chosen according to the clinical context and individual patient characteristics, and the operator's experience and preferences.16–18Fig. 2 shows the aid proposed by the Spanish Society of Anaesthesiology, Reanimation and Pain Therapy (SEDAR) Spanish Society of Emergency and Emergency Medicine (SEMES), and Spanish Society of Otolaryngology, Head and Neck Surgery (SEORL-CCC) for TI of the anticipated DAW.

Continuous oxygenation increases safety by preventing or minimising hypoxaemia.12,19 Conventional methods may be insufficient to prevent desaturation.20 HFNO allows longer tolerance of potential AW obstruction, hypoventilation, or apnoea period.20–23 Therefore, although the evidence is incipient, it is becoming the method of choice.13,24
Non-invasive ventilation (NIV) with endoscopic mask may have a role in IT of critically ill patients with severe hypoxaemia (E.S. 82.9%).25
TopicalisationTopical anaesthesia of the AW is the key element of the procedure, because it is the main determinant of its success.1 With its good cardiovascular and systemic toxicity risk profile, lidocaine (2%–4%) is the most widely used local anaesthetic (LA).12,19,26–28 The maximum total dose should not exceed 9 mg/kg.13,29 The minimum dose necessary should be used.
The "spray-as-you-go" (SAYGO) technique, using an epidural catheter or atomisers, and regional blocks (glossopharyngeal, superior laryngeal, transtracheal injection) are the most commonly used methods for topical anaesthesia of the respiratory mucosa.2,12,27 They are usually used in combination.28 There is no evidence as to which method is superior,16 although nerve blocks are more invasive, require multiple bilateral injections, require experience, and are associated with a higher incidence of complications.2,13,16 Transtracheal block (lidocaine 4%, 4 mL) is perhaps the most useful invasive method as (1) it provides anaesthesia of the subglottic larynx, upper trachea, and even supraglottic structures,30 (2) its success rate is greater than 95%,12 and (3) complications are rare (1:10,000), although they can be significant.28,31
The SAYGO technique can minimise the risk of aspiration, as laryngeal reflexes are maintained until just before passing the ETT.2 Premedication with an antisialogogue is recommended to optimise LA efficacy and field of view, glycopyrrolate (3 μg/kg) being the antisialogogue of choice (E.S. 80%) due to its rapid onset of action, nil effect on the central nervous system (CNS), and moderate vagolytic effect.2,12,32 Its administration 15−20 min beforehand reduces the dilution and oesophageal elimination of LA by secretions.1
Regardless of the method used, topicalisation should include the oral cavity, nasal cavity if nasotracheal intubation is planned, oropharynx, periglottic area, larynx, and trachea.1,30 Otherwise, device insertion and TI trigger reflex responses of the AW, such as cough or laryngospasm, as well as a cardiovascular response mediated by the sympathetic nervous system.33
SedationSedation is an optional adjunct to adequate topical anaesthesia in awake airway management (ATI) (E.S. 88.6%)16 because awake TI with prior psychological preparation can be safely and effectively performed without it.19,28,34 It should never compensate for poor topicalisation. While very high levels of anxiety may increase the physiological stress response and reduce tolerance, over-sedation may cause loss of cooperation, respiratory depression, hypoxia, hypercapnia, AW obstruction, aspiration, or cardiovascular instability.19,35,36 Therefore, the administration of sedation must be justified through a thorough risk-benefit analysis. The objectives to be achieved are (E.S. 94.3%),1,19,35 (1) effective anxiolysis and amnesia while maintaining patient cooperation ("conscious sedation", Ramsay sedation score 2–3)28,37 and (2) analgesia to suppress cough and gag reflex, and reduce haemodynamic response while preserving AW patency, spontaneous ventilation, and avoiding aspiration. Careful monitoring is required to avoid overdosing and it is recommended that a second anaesthetist be exclusively responsible for injecting and monitoring the effects of sedation.13,19
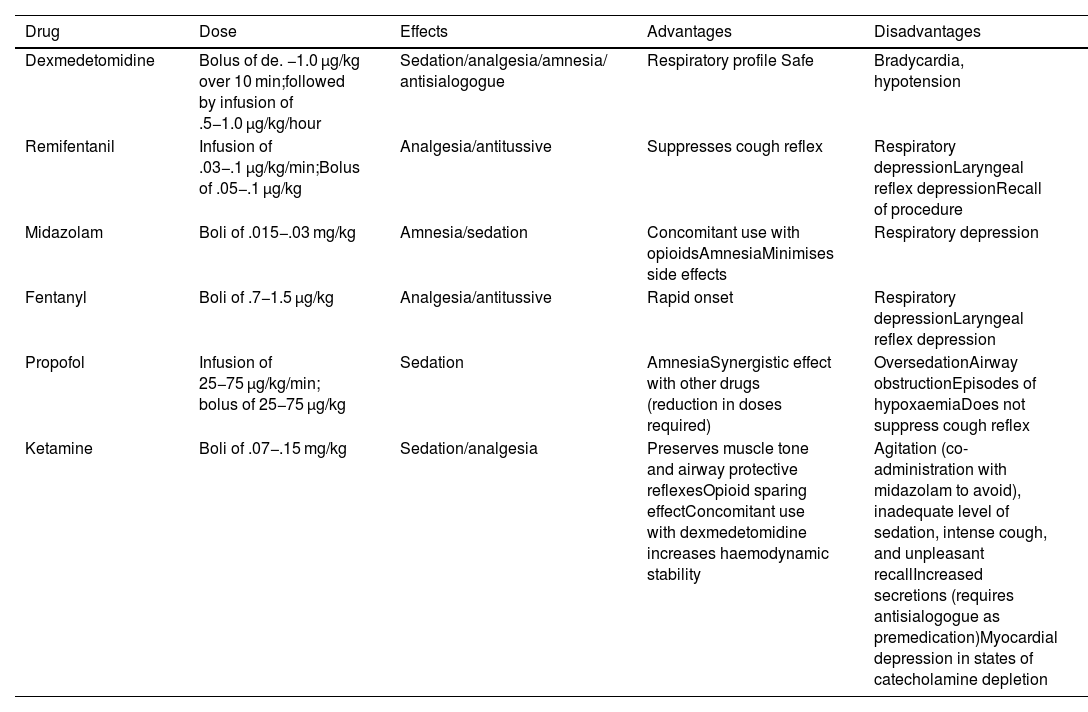
The different sedation regimens have shown a satisfactory level of efficacy and safety.16 Dexmedetomidine, with its anxiolytic, sedative, analgesic, and sympatholytic properties, may have a better efficacy and safety profile by producing fewer episodes of apnoea and desaturation, and is well tolerated and associated with better TI conditions and lower recall compared to other drugs,16,38–40 although it may cause episodes of severe bradycardia and hypotension.35 Its ability to maintain the integrity of respiratory function, even with deep levels of sedation, makes it a good choice for patients at risk of AW obstruction and/or respiratory failure.35 Opioids, particularly remifentanil, attenuate cough and gag reflex, although they may increase the incidence of chest rigidity and laryngospasm6,13,19 and are linked to a high incidence of recall when used as a single drug, requiring administration with a benzodiazepine such as midazolam.19,28 In general, monotherapy is more predictable and reliable, although its safety is enhanced with the availability of specific opioid and benzodiazepine antagonists. Remifentanil is a good option when topical anaesthesia is not possible.35,41 Propofol is associated with a low incidence of recall at the expense of an increased risk of excessive sedation, AW obstruction, and cough.13,35,42Table 1 shows the main drugs used for sedation.
Main drugs used for sedation in awake airway management.
| Drug | Dose | Effects | Advantages | Disadvantages |
|---|---|---|---|---|
| Dexmedetomidine | Bolus of de. −1.0 μg/kg over 10 min;followed by infusion of .5−1.0 μg/kg/hour | Sedation/analgesia/amnesia/ antisialogogue | Respiratory profile Safe | Bradycardia, hypotension |
| Remifentanil | Infusion of .03−.1 μg/kg/min;Bolus of .05−.1 μg/kg | Analgesia/antitussive | Suppresses cough reflex | Respiratory depressionLaryngeal reflex depressionRecall of procedure |
| Midazolam | Boli of .015−.03 mg/kg | Amnesia/sedation | Concomitant use with opioidsAmnesiaMinimises side effects | Respiratory depression |
| Fentanyl | Boli of .7−1.5 μg/kg | Analgesia/antitussive | Rapid onset | Respiratory depressionLaryngeal reflex depression |
| Propofol | Infusion of 25−75 μg/kg/min; bolus of 25−75 μg/kg | Sedation | AmnesiaSynergistic effect with other drugs (reduction in doses required) | OversedationAirway obstructionEpisodes of hypoxaemiaDoes not suppress cough reflex |
| Ketamine | Boli of .07−.15 mg/kg | Sedation/analgesia | Preserves muscle tone and airway protective reflexesOpioid sparing effectConcomitant use with dexmedetomidine increases haemodynamic stability | Agitation (co-administration with midazolam to avoid), inadequate level of sedation, intense cough, and unpleasant recallIncreased secretions (requires antisialogogue as premedication)Myocardial depression in states of catecholamine depletion |
Doses taken from Gil K, et al.6.
FOB-guided TI is classically considered the method of choice in the awake patient2,17,37,43 because of its versatility and unique combinability with other devices in any treatment plan,44 and its efficacy and safety.16,45 However, it is a complex skill that require regular practice, is fallible, and is not available for all patients.37,46
Elective awake TI with video laryngoscopy (VL) may be faster than FOB-guided, which may decrease the risk of aspiration, and be associated with equivalent success rates, safety profile, and patient and operator satisfaction.17,43,47,48 Furthermore, the competence required for its use is easy to acquire and maintain.46,47 It is therefore a valid alternative technique as a first-line treatment.13,17,46–49 The video laryngoscopes indicated for this context are those with a hyperangulated blade, with or without a guide channel. In certain circumstances, VL offers additional advantages over FOB.17,37,43 It also allows an ETT of any diameter to be selected,37 it can be changed without removing the device,47 and its passage through the vocal cords can be observed, unlike advancing blind with FOB, which reduces the risk of injury from the ETT and associated trauma.37,50,51 However, unlike FOB, its use is not feasible with a buccal opening of less than 18−20 mm or a space-occupying lesion in the oral cavity, 37 and may result in increased cervical spine movement in patients with instability without manual stabilisation,52 although the results appear similar.53,54 Therefore, VL cannot completely replace FOB-guided TI.37,43
There is insufficient evidence as to which technique is ideal, and therefore selection of the device must be context-sensitive.43,48 The two approaches are virtually equivalent and complementary43; a failed attempt of one can be rescued with the alternative and both can be used in combination, primarily to treat very difficult AW.2,17,37
Single-use flexible FOBs have a similar safety profile to reusable FOBs,55,56 although they may be associated with benefits in terms of cost-effectiveness, cross contamination, infection, and resource utilisation.57,58
ProcedureThe conditions of all four components should be optimal from the first attempt to maximise the likelihood of success and minimise the number of attempts. If the selected primary technique (FOB or VL) fails, the alternative technique should be used (E.S. 80%). A third attempt may benefit from a multimodality approach consisting of the combination of VL + FOB (E.S. 100%), therefore using the advantages of both devices.59 This combination may improve the first attempt success rate, reduce TI time, reduce morbidity,60,61 and could be the approach of choice in AWs with severely distorted anatomies.
The combination of a supraglottic airway device (SAD) and FOB may be useful as a rescue technique to maintain oxygenation, maintain AW patency, and perform TI through the SAD (E.S. 100%).62,63 The SAD acts as a conduit to for an FOB-guided TI, maintaining oxygenation and AW patency and isolating the periglottic structures from any secretions or blood. At the same time, it facilitates locating the glottis and decreases the difficulty of advancing the ETT over the FOB,51 while the latter allows the SAD to be placed in the correct location. The new laryngeal video masks could simplify this technique.65,66
The total number of attempts should be limited to three (E.S. 88.6%) because repeated attempts increase the risk of oedema, laryngeal bleeding, and complete obstruction of the AW.51 It is especially important in the presence of a pre-existing obstruction because it can rapidly progress to a can’t intubate-can’t-oxygenate (CICO) situation.9,67 Each failure should be followed by an assessment of each of the four components of the technique to determine whether optimisation is feasible.
Factors such as surgical approach, anatomical features, extubation plan, and operator preference determine the choice of TI route.68
The inability to advance the ETT over the FOB, stylet, or an exchanger through the vocal cords due to impingement upon periglottic structures, primarily the right arytenoid cartilage,2,50 is one of the main reasons for TI failure,19,51 and glottic or subglottic damage.50,69 ETTs with a conical opening made of silicone such as LMA Fastrach™ (Teleflex Medical, Dublin, Ireland),70 those with a central opening and posterior facing bevel such as the Parker Flex-Tip™ (Parker Medical, Highlands Ranch, CO USA),71–74 LMA Fastrach™,75 and BlockBuster (Tuoren Medical Instrument co, Ltd, Changyuan city, China),69 and flexible material and reduced or no anterior curvature such as the reinforced LMA Fastrach™ and flexometalic ETTs69,76 reduce the incidence of this complication.50,69,72,76,77 The Parker Flex ETT is recommended over conventional ETT for FOB-guided TI in the general population (1 B), posterior placement of the bevel or 90 ° anti-clockwise rotation so that the bevel faces posteriorly facilitate its advancement.78–80 Other useful manoeuvres include cervical spine flexion and release of jaw thrust or cricoid pressure.51,80 It is recommended to decrease the difference between the external diameter of the FOB and the internal diameter of the ETT to facilitate FOB-guided TI (E.S. 85.7%),2,51,81 or to use an intubation catheter between the FOB and the ETT (e.g. Aintree catheter, AIC, Cook Critical Care, Bloomington, IN, USA). Similarly, a device-specific ETT is recommended facilitate VL-guided TI.82 Parker Flex ETT rather than conventional ETT is suggested for FOB and laryngoscopy in the general population to reduce complications (1 C).
Smaller sized ETTs allow a better laryngeal view during laryngoscopy and facilitate TI by reducing the impact on periglottic structures.51,83,84 Also, large ETTs are associated with increased morbidity.83,85–90 ETTs up to 6.0 mm internal diameter allow access for intubation devices, suction devices, and small-calibre FOB. PPV can be performed without increasing the risk of ventilator-induced lung injury or air trapping,91,92 even when high minute volumes (MV) are required. There is also no demonstrable increased risk of aspiration or cuff pressure damage when smaller ETTs are used; they may even provide a better seal than the larger ETTs.93 Smaller ETTs may not be safe in all cases, such as in patients with heavy secretions or limited airflow. Therefore, a smaller ETT than usual is recommended with VL and FOB (D.E. 85.7%) for safe treatment performing a risk-benefit analysis according to the clinical context.83,84,90,94
After visual confirmation of TI (passage of the ETT through the glottis with VL and identification of the carina and advancement of the ETT over FOB to two to three tracheal rings above the carina) it is recommended to induce GA after establishing cuff pressure and capnographic confirmation of TI (E.S. 94.3%).2
Alternative techniques and approaches should be planned in advance and applied without delay after failure of the primary approaches (E.S. 100%).12,67 In the event of failed awake TI, there are three alternative plans: (1) postponement of the procedure unless the situation requires immediate treatment, (2) awake front-of-neck access (FONA), or emergency FONA in case of obstruction and loss of AW control, (3) GA induction with complete neuromuscular blockade (NMB) and follow-up of the unexpected DAW algorithm. This is a high-risk option. Deep sedation or GA with spontaneous ventilation induced with ketamine might be a more favourable preliminary step than the establishment of apnoea 95 (Fig. 2).
Given the high likelihood of awake TI failure, it is recommended to prepare the FONA plan in parallel ("double configuration") to treat a potential total obstruction (E.S. 88.6%)96; the incision line is anticipated by marking the cricothyroid membrane (CTM),3 the neck and material are prepared with the surgical team present.9 Multidisciplinary management and coordination with ENT is essential.1,97
RecommendationA Parker Flex ETT is recommended over conventional ETT for FOB-guided TI in the general population.
Strong recommendation; moderate level of evidence (⊕⊕⊕⊝)
A Parker Flex ETT is recommended over conventional ETT for FOB-guided TI in the general population.
Strong recommendation; low level of evidence (⊕⊕⊝⊝)
Awake tracheostomy under local anaesthesia is recommended in the presence of pre-existing critical AW compromise (E.S. 82.9%). In the upper AW with significant distortion or obstruction due to neoplasia, haematoma, severe oedema, bilateral vocal cord paralysis, or haemorrhage, awake FONA under local anaesthesia as the primary plan may be the safest option to secure the AW,67,98–102 because, (1) instrumentation of the upper AW may precipitate bleeding, oedema, increased occlusion, and even distal seeding of a tumour,7,9 (2) topical anaesthesia may exacerbate a pre-existing occlusion,1,103 or cause laryngospasm,1,9 and (3) FOB can cause a "cork in a bottle" effect7 with complete collapse. Multidisciplinary DAW teams are associated with better first attempt success rates and faster time to securing a DAW.104
The recommended technique is tracheostomy performed by a trained professional.105 Sedation should be avoided if possible. HFNO appears to be effective in extending safe apnoea time,106 although extreme caution should be exercised and the use of electrical instruments should be limited at the time of tracheal opening.107 The procedure requires the patient's cooperation as supine decubitus and cervical spine extension is often poorly tolerated.106 Once a capnographic record is available, anaesthetic induction is performed.108 The full moon view of the wall of trachea with FOB confirms correct cannula location. A crescent image indicates the need to reposition or change the cannula.
Awake cricothyrotomy would be the most indicated technique for emergent critical airway compromise (D.E. 91,4%) as it enables a surgical AW to be established more rapidly.109
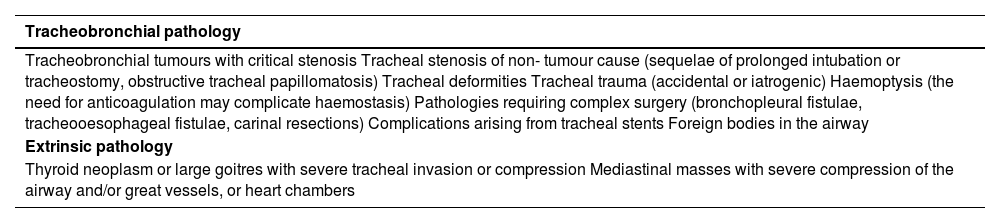
Extracorporeal membrane oxygenationECMO under local anaesthesia in the awake patient may be the safest option when all four conventional plans are expected to be impossible, unsuccessful, or ineffective with risk of complete obstruction of the AW (E.S. 90.6%). Technological advances have made it possible to incorporate ECMO in AW management in these situations to ensure adequate oxygenation.110,111 This is the case of tracheobronchial or extrinsic pathologies, such as anterior cervical spine pathology, which result in a critical central airway obstruction or prevent the performance of an FONA.67,110 In these cases, elective ECMO under local anaesthesia in the awake patient may be the safest option.67,112,113 Once a controlled environment is achieved, the AW is secured to prevent aspiration. Table 2 shows the main indications for ECMO.
Main indications for extracorporeal membrane oxygenation (ECMO).
| Tracheobronchial pathology |
|---|
| Tracheobronchial tumours with critical stenosis Tracheal stenosis of non- tumour cause (sequelae of prolonged intubation or tracheostomy, obstructive tracheal papillomatosis) Tracheal deformities Tracheal trauma (accidental or iatrogenic) Haemoptysis (the need for anticoagulation may complicate haemostasis) Pathologies requiring complex surgery (bronchopleural fistulae, tracheooesophageal fistulae, carinal resections) Complications arising from tracheal stents Foreign bodies in the airway |
| Extrinsic pathology |
| Thyroid neoplasm or large goitres with severe tracheal invasion or compression Mediastinal masses with severe compression of the airway and/or great vessels, or heart chambers |
Given the cost and its potential complications,111,114–116 ECMO must be supported by a careful multidisciplinary decision-making process.116 In uncertain indications, a system prepared with cannulated vessels may be possible and a perfusionist present prior to AW management.116
The respiratory support provided by veno-venous ECMO is associated with fewer complications, does not require therapeutic levels of anticoagulation, and allows the use of a single double-lumen cannula, making it the technique of choice in these situations.110,111 In cases with associated haemodynamic compromise requiring cardiorespiratory support, such as large mediastinal masses, veno-arterial ECMO, or even a conventional cardiopulmonary bypass circuit may be necessary.110
In extreme cases such as massive haemoptysis or central foreign bodies, ECMO may be a last resort.64,117 However, setting it up can be complicated and requires considerable time, so it cannot currently be considered a rescue technique for a CICO situation after GA induction, although several published cases have described its use in this context.
Unanticipated difficult airwayPeri-procedural oxygenationCovered in the relevant section.
Airway managementTI is associated with more complications than other non-invasive plans, and therefore it should not be a "rash act", but an active decision and should be only performed when truly indicated.118
Any approach to the AW should aim to minimise the number of attempts to avoid a CICO situation and the need for FONA. Planning and optimisation play a key role.119
Given the unreliability of predictors,120,121 planning should be geared towards managing a potentially difficult AW.122 Decision-making should be context-sensitive, rather than focussed on specific devices and techniques.8,123
The first attempt should be under a priori optimal conditions (E.S. 100%) to maximise the probability of success ("make your first attempt your best attempt").119,122,124–126 Additional attempts are only justified when there is room for improvement and involve the summative effect of optimisation, or allow substantial improvement in the likelihood of success (e.g., change the size, type of device, adjuvant, or operator as needed).119,127
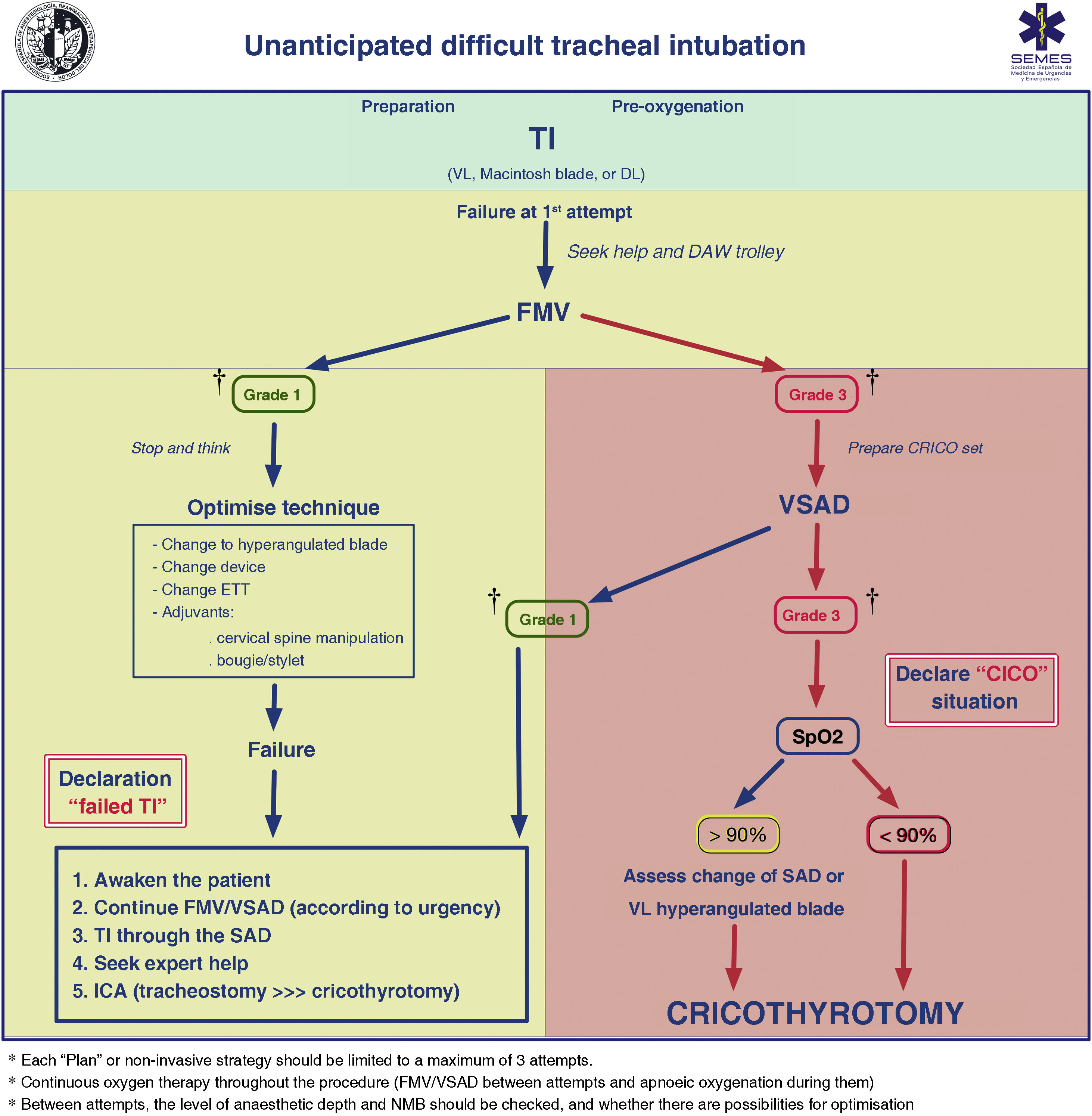
Between attempts, face mask ventilation (FMV), and anaesthetic depth and NMB should be checked. Adequate ventilation between attempts with face mask (FM) or second-generation SAD (2 GSAD) provides an opportunity to "stop and think" to reformulate the strategy, or deploy new resources while maintaining first principles. Fig. 3 shows the treatment algorithm for unexpected TI.
. *Between attempts, the level of anaesthetic depth and NMB should be checked, and whether there are possibilities for optimization.")
Treatment algorithm for unanticipated tracheal intubation.
† Ventilation grades according to capnography waveform; CRICO: cricothyrotomy; DAW: difficult airway; DL: direct laryngoscopy; FONA: front-of-neck access; ETT: endotracheal tube; FMV: face mask ventilation; SAD: supraglottic airway device; SpO2: peripheral oxygen saturation; TI: tracheal intubation; VSAD: ventilation with supraglottic airway device; VL: videolaryngoscopy.
*Each “Plan” or non-invasive strategy should be limited to a maximum of 3 attempts.
*Continuous oxygen therapy throughout the procedure (FMV/VSAD between attempts and apnoeic oxygenation during them).
*Between attempts, the level of anaesthetic depth and NMB should be checked, and whether there are possibilities for optimization.
Failure of non-invasive plans requires declaration of a CICO situation, ensuring adequate NMB, and immediate FONA regardless of peripheral oxygen saturation value (SpO2).
Tracheal intubationVideolaryngoscopyFailure of the first attempt at TI implies a lower probability of success in subsequent attempts.60,119,128 Multiple attempts may result in trauma, oesophageal intubation, hypoxaemia, cardiovascular events, a CICO situation, unexpected admission to the critical care unit, or death.129–134 In addition, up to 93% of difficult TIs are unanticipated.121 Therefore, the most appropriate primary technique should be the one that offers the highest guarantee of a first-attempt TI (E.S. 94.3%).119,122,124–126
Most meta-analyses, despite great heterogeneity135,136 suggest the superiority of VL (Appendix A, supplementary material 4). Overall, VL compared to direct laryngoscopy (DL) increases success at the first attempt,137–150 improves visualisation of the glotis,140,141,143,145–148,150–158 and decreases complications, primarily trauma, and the incidence of oesophageal intubation141,142,144–147,149,152,155–157,159–162 by as much as 50%.150
The emergence of the COVID-19 pandemic,135,163–167 the reduction in costs18 and widespread availability, and incipient positive data on cost-effectiveness,168,169 quality of care,129 teaching, documentation, teamwork (it favours the shared mental and human factors [HF] model),122,167,170–173 and mastery of the technique with regular practice129 have overcome resistance to change,174,175 making VL practically the gold standard for laryngoscopy and DAW.171
In view of the above, SEDAR SEMES SEORL-CCC recommends the routine use of VL over DL as the primary device for TI (1 B). Devices with standard Macintosh-type blades (allowing direct and indirect laryngoscopy) are appropriate for AW management without predictors of difficulty, while those with hyperangulated blades (with or without guide channel) are indicated for known or anticipated DAW (E.S. 94.3%).120,135,176,177 The latter are the devices of choice for rescue after a first unsuccessful attempt.14,178–180 It is therefore recommended that VL and the necessary competence be available in any location where the AW is managed.
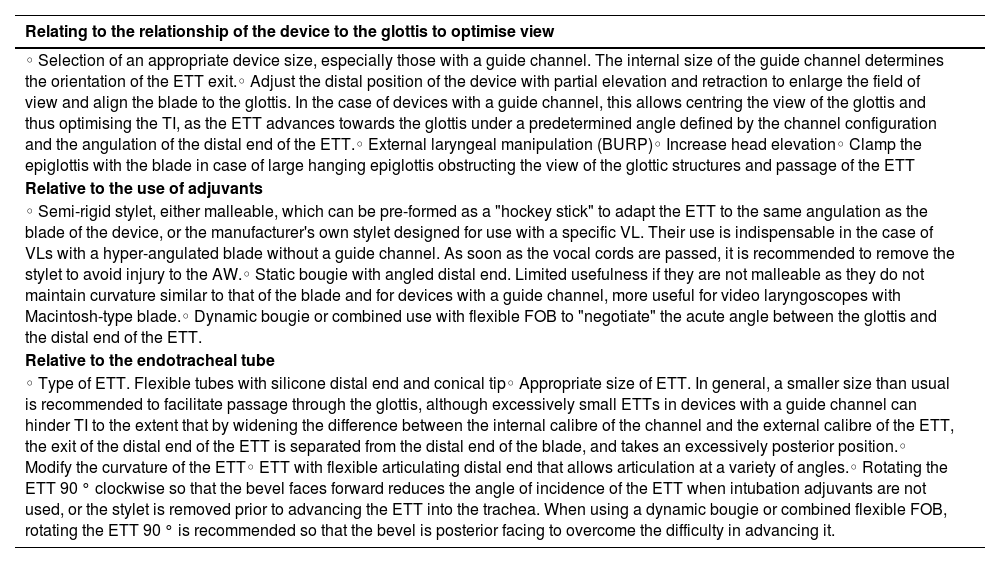
Inability to pass the ETT through the glottis is the most common cause of failed TI with VL.166,172,173,181,182 However, with adequate competence it is rare for this problem not to be overcome.171 The recommended manoeuvres to overcome this difficulty are shown in Table 3.182–186
Manoeuvres to overcome difficult tracheal intubation with video laryngoscopy.
| Relating to the relationship of the device to the glottis to optimise view |
|---|
| ◦ Selection of an appropriate device size, especially those with a guide channel. The internal size of the guide channel determines the orientation of the ETT exit.◦ Adjust the distal position of the device with partial elevation and retraction to enlarge the field of view and align the blade to the glottis. In the case of devices with a guide channel, this allows centring the view of the glottis and thus optimising the TI, as the ETT advances towards the glottis under a predetermined angle defined by the channel configuration and the angulation of the distal end of the ETT.◦ External laryngeal manipulation (BURP)◦ Increase head elevation◦ Clamp the epiglottis with the blade in case of large hanging epiglottis obstructing the view of the glottic structures and passage of the ETT |
| Relative to the use of adjuvants |
| ◦ Semi-rigid stylet, either malleable, which can be pre-formed as a "hockey stick" to adapt the ETT to the same angulation as the blade of the device, or the manufacturer's own stylet designed for use with a specific VL. Their use is indispensable in the case of VLs with a hyper-angulated blade without a guide channel. As soon as the vocal cords are passed, it is recommended to remove the stylet to avoid injury to the AW.◦ Static bougie with angled distal end. Limited usefulness if they are not malleable as they do not maintain curvature similar to that of the blade and for devices with a guide channel, more useful for video laryngoscopes with Macintosh-type blade.◦ Dynamic bougie or combined use with flexible FOB to "negotiate" the acute angle between the glottis and the distal end of the ETT. |
| Relative to the endotracheal tube |
| ◦ Type of ETT. Flexible tubes with silicone distal end and conical tip◦ Appropriate size of ETT. In general, a smaller size than usual is recommended to facilitate passage through the glottis, although excessively small ETTs in devices with a guide channel can hinder TI to the extent that by widening the difference between the internal calibre of the channel and the external calibre of the ETT, the exit of the distal end of the ETT is separated from the distal end of the blade, and takes an excessively posterior position.◦ Modify the curvature of the ETT◦ ETT with flexible articulating distal end that allows articulation at a variety of angles.◦ Rotating the ETT 90 ° clockwise so that the bevel faces forward reduces the angle of incidence of the ETT when intubation adjuvants are not used, or the stylet is removed prior to advancing the ETT into the trachea. When using a dynamic bougie or combined flexible FOB, rotating the ETT 90 ° is recommended so that the bevel is posterior facing to overcome the difficulty in advancing it. |
BURP: backward, upward, right lateral position; FOB: fibrobronchoscopy; TI: tracheal intubation; ETT: endotracheal tube; AW: airway; VL: videolaryngoscopy.
Bougies are associated with higher first-attempt success rates in elective and emergency TI, especially in patients with predictors of DAW or poor view of the glottis.187–190 It is recommended that a bougie be available in every location with AW management (E.S. 97.1%)191 and its use should be assessed from the first attempt.120,185,188,192 SEDAR SEMES SEORL-CCC recommend the use of a dynamic or articulated bougie versus a conventional stylet for TI in patients with DAW (1 C) because it improves the first-attempt TI rate and time to successful intubation, thus reducing instrumentation and the use of alternative adjuvants.60,69,186,193,194
RecommendationRoutine use of VL is recommended over DL as the primary device for TI.
Strong recommendation; moderate level of evidence (⊕⊕⊕⊝)
Aa dynamic or articulated bougie (flex-tip or FOB type) is recommended over a conventional stylet for TI in patients with DAW.
Strong recommendation; low level of evidence (⊕⊕⊝⊝)
FOB-guided TI in the patient, unconscious or under GA can be very effective in skilled hands,195–198 but is technically more difficult than in the awake patient, and it may fail and be associated with episodes of desaturation or complete obstruction of the AW.105 The presence of blood, emesis, or secretions in emergency TI further reduces the likelihood of success.
Manoeuvres such as lingual traction and jaw-thrust allow opening of the pharynx and larynx respectively, improving view and the success of the technique.197,199 Oral cannulae, anterior displacement of the base of the tongue with the laryngoscope or patient in the left semilateral position rotating their head to the left facilitate passage of the FOB and improve view.200 If there is resistance to ETT advancement, jaw-thrust and anticlockwise rotation of the ETT can facilitate its passage through the glottis.198
All the patients included in the 4th National Audit Project (NAP4) registry in whom FOB-guided TI was attempted after induction of GA as the primary technique or after failure of DL, failed and emergency FONA was required.
FOB is highly salvageable after failure of most devices, either alone or as a multimodal approach.6 In an emergency, its availability, preparation, and execution is more laborious and time-consuming than VL,43,47 and therefore it is less widely used as a rescue device.201
Confirmation of tracheal intubationOnce TI has been achieved, it is recommended to immediately rule out oesophageal intubation as this is a common complication with devastating consequences.167,202–204
No confirmatory technique is 100% reliable in all circumstances, and therefore a combination of methods is recommended.205,206
The capnography waveform is the gold standard for confirming TI (1 B) because it is the most accurate (sensitivity 98%–100% and specificity 100%) and rapid method.4,120,205,207–212 Therefore, despite persistent deficits in standardisation,204 capnography is mandatory to confirm ETT placement and should be present in all locations where AW management may be required.167,203,211,213–216 An absent trace (grade 3 ventilation) indicates failed TI until proven otherwise (E.D. 80%)211,217 and oesophageal intubation should be actively excluded.218 The capnography trace is present but attenuated (not flat) even in cardiac arrest.211,212,217–219 The positive predictive value of end-tidal carbon dioxide (EtCO2) is lower during cases of low or no perfusion212 and false positive readings are possible when the ETT tip is in the hypopharynx.205 In these cases, confirmation by ultrasound is a valid alternative as it has a sensitivity of 99% and specificity of 97%, is independent of pulmonary blood flow, is quick to perform (mean time of 13 seconds), and even allows real-time visualisation of the introduction of the ETT into the trachea or oesophagus.220,221 Presence of the "double tract sign" allows detection of oesophageal intubation before initiation of ventilation.216,222
Colorimetric capnometry should be limited to situations where a capnography waveform is not available, such as in pre-hospital or emergency settings.205
Clinical examination alone has too high a false positive rate,223 especially in an emergency setting,224 and confirmation bias can lead to seeing and hearing what one wants,225 although in combination with capnography it is useful. Ultrasound or fibrobronchoscopy examination via the ETT are alternative methods of confirming a TI. Other methods are oesophageal detector devices, transtracheal illumination, pulse oximetry, and chest radiography.205
Capnography waveform monitoring during maintenance of mechanical ventilation is highly recommended in all settings (E.S. 100%)207,209,211,226–230 because it allows continuous monitoring of the position of the ETT, confirmation of AW patency, and early diagnosis of inadvertent extubation or partial displacement of an artificial AW.211,218,227,229,231–233 The NAP4 registry found that lack of monitoring may have contributed to more than 70% of AW-related ICU deaths, 234 and therefore widespread use of capnography in critical care units and education of medical and nursing staff211,217,218 may be the single change with the greatest potential to prevent morbidity and mortality associated with TI or other artificial AW outside the operating theatre.211,234
RecommendationIn addition to their use as a primary technique in elective surgical procedures or cardiopulmonary resuscitation,235–237 SADS play an indispensable role in the rescue of difficult or failed TI as they allow ventilation and oxygenation, provide a patent AW with some degree of protection against aspiration, and act as conduits to facilitate FOB-guided TI.238–243 Anatomical and/or technical factors hindering FMV and IT usually do not influence the insertion and function of the SAD.239 Therefore, an SAD should be inserted without delay to preserve alveolar oxygenation in the event of difficult or failed TI (E.S. 85.7%).
2 G SADs have most of the ideal characteristics: easy insertion, high oropharyngeal sealing pressures, and they allow TI and gastric decompression.49,239,244 They have thus shown superior performance to first generation devices and are more suitable for advanced use and as rescue devices.244–246 Therefore, the immediate availability of an 2 G SAD is recommended, and to have the necessary competence to use it in all AW management sites (E.S. 100%).
The SAD to rescue a DAW should be selected prior to the procedure. Those with high first-attempt ventilation success and that allow IT through them238,247 are of first choice: i-gel™ (Intersurgical Ltd., Wokingham, UK), Ambu® AuraGain™ (Ambu A/S, Ballerup, Denmark), LMA® Protector™ (The Laryngeal Mask Company Limited, Mahé, Seychelles), and iLTS-D (VBM Medizintechnik GmbH, Sulz, Germany).
One optimal attempt or a maximum of three attempts before declaring plan failure is recommended as the success rate decreases significantly with successive attempts248,249 and these attempts increase trauma and delay transition between plans. During insertion of an SAD, cricoid pressure should be released if it is being used (E.S. 80%). Each attempt should include a change to improve the chances of success. Between and during attempts it is recommended to continue with peri-procedural oxygenation methods.
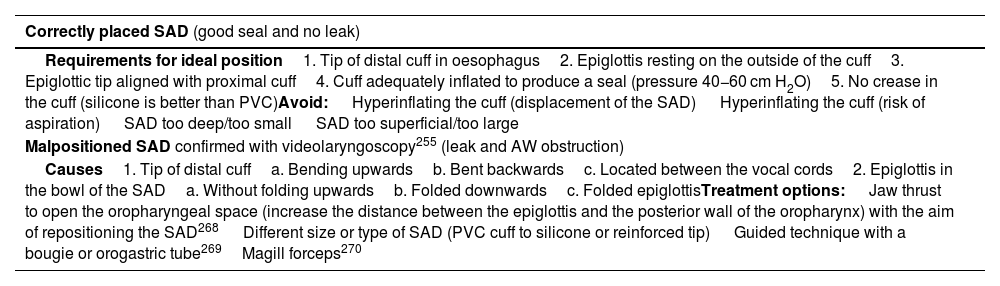
Rapid insertion and correct placement of the SAD are important to ensure the AW.250 Rotation of 90 °, jaw-thrust and the use of DL or VL (of choice) with the "insert-detect-correct-as-you-go" technique increase the efficacy and safety of the SAD by facilitating insertion, increase the first- attempt success rate and reduce pharyngeal trauma (E.S. 82.9%),246,250–257 and can prevent malpositioning.257,258 In contrast, "blind" insertion results in 50%–80% malpositioning246,256,257 associated with suboptimal AW control, leakage or obstruction, increased risk of further displacement and increased morbidity.251,255,259 Malpositioned SADs are 26 times more likely to cause gastric insufflation and subsequent aspiration.255Table 4 shows the requirements for ideal positioning of an SAD, causes of malpositioning, and treatment options.246,255 The recent videolaryngeal masks (VLM)259 allow placement under direct view and immediate corrective manoeuvres without the aid of an additional device,66 although there is still insufficient evidence.259–264
Requirements for ideal position of a supraglottic airway device, causes of malpositioning, and options for AW management.
| Correctly placed SAD (good seal and no leak) |
|---|
| Requirements for ideal position1. Tip of distal cuff in oesophagus2. Epiglottis resting on the outside of the cuff3. Epiglottic tip aligned with proximal cuff4. Cuff adequately inflated to produce a seal (pressure 40−60 cm H2O)5. No crease in the cuff (silicone is better than PVC)Avoid: Hyperinflating the cuff (displacement of the SAD) Hyperinflating the cuff (risk of aspiration) SAD too deep/too small SAD too superficial/too large |
| Malpositioned SAD confirmed with videolaryngoscopy255 (leak and AW obstruction) |
| Causes1. Tip of distal cuffa. Bending upwardsb. Bent backwardsc. Located between the vocal cords2. Epiglottis in the bowl of the SADa. Without folding upwardsb. Folded downwardsc. Folded epiglottisTreatment options: Jaw thrust to open the oropharyngeal space (increase the distance between the epiglottis and the posterior wall of the oropharynx) with the aim of repositioning the SAD268 Different size or type of SAD (PVC cuff to silicone or reinforced tip) Guided technique with a bougie or orogastric tube269Magill forceps270 |
SAD: supraglottic airway device.
Adapted from Van Zundert AA, et al.246
Correct placement of an SAD is clinically confirmed by a normal capnography waveform (ventilation grade 1) and maintenance of adequate alveolar oxygenation with peak inspiratory pressures of 20 cmH2O, oropharyngeal leak pressure >25 cmH2O, pulmonary auscultation, and passage of a tube through the gastric channel as complementary signs.259
Achieving effective ventilation and oxygenation provides time to stop and decide how to proceed according to the degree of urgency and type of procedure:
- 1
If the situation is non-urgent (e.g. elective surgical procedure), the safest option is to awaken the patient and perform surgery under regional anaesthesia or postpone the intervention to perform an ATI.
- 2
If the situation is an emergency in (a) urgent surgery: it may be decided to continue the procedure while maintaining the second-generation SAD, but this is a high-risk option because the AW patency may be compromised in the course of the surgery; (b) the critically ill patient: a definitive AW is likely to be required, and therefore a FONA (tracheostomy) may be performed in anticipation of life-threatening hypoxaemia.
- 3
In intermediate cases, FOB-guided TI via the SAD may be chosen if the situation is stable, under adequate NMB and if the operator is competent (E.S. 97.1%, success rates close to 100%238). Blind TI is not recommended as the success rate is low (10%–20%), repeated attempts are required, and may result in increased trauma and impaired oxygenation.265,266 The use of VLM allows TI without the help of FOB,66 and many therefore shorten the technique and be especially advantageous in settings where FOB is not available, such as pre-hospital care and emergency care.267
Grade 2–3 ventilation or ineffective oxygenation after exhausting attempts requires immediate progression to a new plan.
Face mask ventilationFMV is an essential transitional technique during induction and treatment of an emergency AW and an indispensable rescue plan when other techniques fail.271
The presence of predictors of difficult FMV, and its use during emergency AW or as rescue from failed plans, make it especially advisable to use the optimal technique for FMV (triple manoeuvre of full neck extension, anterior jaw thrust, and mouth opening) from the outset, oropharyngeal or nasopharyngeal cannula placement,272 and two-handed V-E technique,271,273 either with two operators or with pressure-controlled ventilation with ventilator or other device,274,275 in a patient with optimal positioning and intense NMB271,276–280) (E.S. 80%) in order to limit AW obstruction and optimise sealing to achieve grade 1 alveolar ventilation without causing gastric insufflation.126,275,281 This also speeds up the transition between plans and reduces peak ventilation pressure.282 Face mask ventilation with modified triple manoeuvre is recommended over the E-C technique for the general population (1 C).
An effective attempt should be defined, in addition to a stable or improved normal SpO2, an acceptable tidal volume and AW pressure (4−5 mL/kg−1 and <15−20 cmH2O, respectively273,275,283) and clinical criteria, by the presence of plateau phase on the capnography trace.284 The use of scales to stratify the difficulty of FMV objectively, such as that proposed by the Japanese Society of Anaesthesiologists (Fig. 2, Part I), is recommended. This allows early declaration of failed FMV before desaturation (late sign) occurs.275
FMV is a dynamic procedure that requires continuous assessment until the AW is assured.285 Declaration of failed FMV implies immediate transition to ventilation with SAD (E.S. 85.7%). Clinical deterioration and worsening oxygenation should prompt declaration of a CICO situation and immediate transition to FONA if ventilation with SAD has also failed.
A CICO situation should be declared using clear language that is easily understood by the entire team to create a shared model that facilitates an effective transition to FONA.119,286
RecommendationFront-of-neck access techniquesFailure of the three non-invasive supraglottic plans (primary and rescue) in the apnoeic patient requires declaration of a CICO situation and prompt FONA regardless of the SpO2 value (E.S. 90.6%) because, in these circumstances, deterioration will be imminent if it is not already apparent. In the hospital setting, SEDAR SEMES SEORL-CCC recommends requesting the presence of an ENT specialist (or surgeon trained in performing tracheostomy) as soon as a CICO situation has been declared, although no procedure should be delayed until such time.
Delay in FONA is a major cause of morbidity and mortality.99,234,247,287,288 Situational awareness and shared decision making, as well as good technical and HF training, can remove these psychological barriers to abandoning further attempts at non-invasive techniques.99,119,287,289–291 The use of cognitive aids speeds up the transition to FONA by mitigating stress292 (Fig. 1, Part I).
Psychological and technical preparation is recommended before declaring a CICO situation. A "double set-up" may be useful293: one team manages the AW conventionally while a second team is prepared and ready to perform a potential FONA. The multidisciplinary approach is associated with better first-attempt success rates and faster time to securing the DAW.104
It is recommended to continue 100% supraglottic oxygen delivery, ensure intense NMB127,294 and full neck extension for better laryngeal exposure.295
Emergency FONA encompasses three techniques: percutaneous cricothyrotomy, surgical cricothyrotomy, and surgical tracheostomy.
Cricothyrotomy is the technique of choice in a CICO situation (S.D. 91.4%) due to its relative simplicity, rapidity, high success rate, and low complication rate,100,296 although the presence of an experienced ENT specialist or surgeon ensures that tracheostomy is performed as effectively and safely as a scalpel cricothyrotomy,297,298 and therefore if the ENT specialist is present, they will lead the FONA using the technique they consider most appropriate.
The approach to a cricothyrotomy can be surgical or percutaneous. The evidence is limited as to which FONA approach is more appropriate in this setting. The few comparisons that have been made were in a simulation model and an animal model,99 and therefore no one technique can be identified as superior to the others.99,101,299–302 However, surgical access is successful in virtually 100% of cases.234,287,303
SEDAR SEMES SEORL-CCC recommend the scalpel-bougie-tube surgical cricothyrotomy method (E.S. 91.4%) for the following reasons98,234,247,287,291,294,301,304,305: (1) universality of the material, (2) it can be performed by a single operator, (3) technical competence is easy to acquire, (4) its execution, despite involving a greater psychological challenge,300,306,307 it is characterised by its simplicity and speed, (5) it allows insertion into the trachea of an ETT or cannula with balloon and sufficient internal diameter to definitively secure the AW, protect it against aspiration, and allow effective gas exchange by means of PPV with conventional equipment and confirmation with capnography, and (6) its safety and efficacy profile. The required equipment includes a scalpel with blade no. 10, 20, or 21, ETT, or cannula with an internal diameter of no more than 6 mm and a bougie.
Other cricothyrotomy methods are considered valid, provided the appropriate expertise and equipment are available. Percutaneous cricothyrotomy approaches that achieve re-establishment of oxygenation with adequate ventilation are those that allow the introduction of a tube or cannula with an internal diameter ≥ 4 mm and 15 mm connector, or wide cannula techniques.247,291,294,301,305,308 SEDAR SEMES SEORL-CCC leaves its use to the operator's discretion as first choice or as rescue due to failure of another method,309 and therefore recommends acquiring skills in more than one technique.300,302,310 Experience, availability of the equipment, and patient characteristics play a relevant role in the selection of technique.99,101,294,297,309,311 The percutaneous technique, because it is more familiar and less intimidating, could be initiated earlier.300
It is essential to identify the CTM for the success of the technique. Detection by palpation has a high error rate. The use of ultrasonography over palpation is recommended to identify the cricothyroid membrane (1 C), and therefore SEDAR SEMES SEORL-CCC recommends acquiring the necessary skills. The laryngeal handshake technique, although slightly more time-consuming than conventional techniques, has a higher success rate.312,313 For cervical spine anatomies with anatomical landmarks that are difficult to identify by palpation, a vertical skin incision of more than 4 cm in the midline of the neck in a distal-proximal direction above the sternal notch is suggested to find the relevant anatomy.98,247,314 Ultrasonography is superior to palpation in identifying the CTM and its immediate availability improves success.315–319 However, it can be time-consuming, and therefore in a CICO situation it is only recommended if there is immediate availability and sufficient training.
After ensuring FONA, correct ventilation and alveolar oxygenation should be verified by capnography waveform, clinical assessment, pulse oximetry, and arterial blood gases when indicated.294 A fibrobronchoscopy and radiological examination can complete the examination. Emergency cricothyrotomy should be converted to an ETT or tracheostomy as there is insufficient evidence as long-term treatment (E.S. 85.7%).296,320 Conversion within 72 h is recommended to avoid the development of subglottic stenosis.301,321
Failure of a cricothyrotomy makes tracheostomy by a skilled operator advisable (E.S. 94.3%).100
CICO situations accounted for 39% of critical events and 25% of all anaesthesia-related deaths in the NAP4.287 FONA is the last resort when non-invasive strategies have failed and is therefore of vital importance.322 It is recommended that every institution standardise the technique and have a commercial or pre-assembled cricothyrotomy kit99,247,311,323 with transparent packaging, which allows familiarisation with its contents and mental rehearsal of its use, and easy access, ideally located on the DAW trolley, available in every AW management site. All AW management professionals must acquire and maintain the necessary competence to perform a surgical or percutaneous cricothyrotomy with Seldinger's technique (E.S. 100%).99,101,119,247,291,298,301 FONA should be feasible in any AW management site (E.S. 100%).324
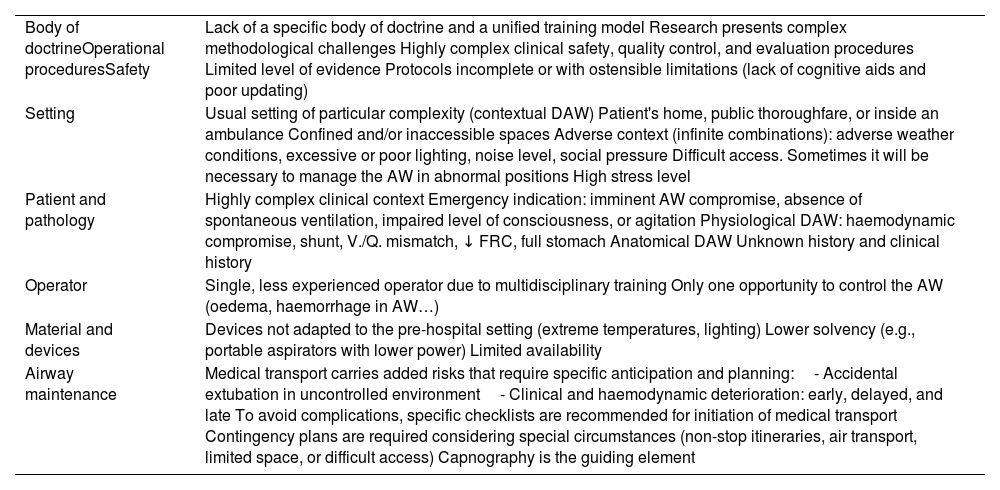
RecommendationPre-hospital settingAW management in the pre-hospital setting is critical to patient survival and represents a real challenge for the emergency medical services (EMS).325,326 In each scenario, different combinations of factors and constraints come together to create a high level of uncertainty that can turn any ordinary AW into a DAW.327 Also, patient and operator positions may not always conform to those described in the manuals (subject trapped, confined, crushed, buried or in a place with simply no space). Survival depends on the correct interlocking of the entire chain of care. Table 5 shows the differential characteristics of AW management in the pre-hospital setting.328,329
Differential characteristics of AW management in the prehospital setting.
| Body of doctrineOperational proceduresSafety | Lack of a specific body of doctrine and a unified training model Research presents complex methodological challenges Highly complex clinical safety, quality control, and evaluation procedures Limited level of evidence Protocols incomplete or with ostensible limitations (lack of cognitive aids and poor updating) |
| Setting | Usual setting of particular complexity (contextual DAW) Patient's home, public thoroughfare, or inside an ambulance Confined and/or inaccessible spaces Adverse context (infinite combinations): adverse weather conditions, excessive or poor lighting, noise level, social pressure Difficult access. Sometimes it will be necessary to manage the AW in abnormal positions High stress level |
| Patient and pathology | Highly complex clinical context Emergency indication: imminent AW compromise, absence of spontaneous ventilation, impaired level of consciousness, or agitation Physiological DAW: haemodynamic compromise, shunt, V./Q. mismatch, ↓ FRC, full stomach Anatomical DAW Unknown history and clinical history |
| Operator | Single, less experienced operator due to multidisciplinary training Only one opportunity to control the AW (oedema, haemorrhage in AW…) |
| Material and devices | Devices not adapted to the pre-hospital setting (extreme temperatures, lighting) Lower solvency (e.g., portable aspirators with lower power) Limited availability |
| Airway maintenance | Medical transport carries added risks that require specific anticipation and planning:- Accidental extubation in uncontrolled environment- Clinical and haemodynamic deterioration: early, delayed, and late To avoid complications, specific checklists are recommended for initiation of medical transport Contingency plans are required considering special circumstances (non-stop itineraries, air transport, limited space, or difficult access) Capnography is the guiding element |
AW: airway; DAW: difficult airway; FRC: functional residual capacity; V./Q. mismatch: ventilation/perfusion mismatch.
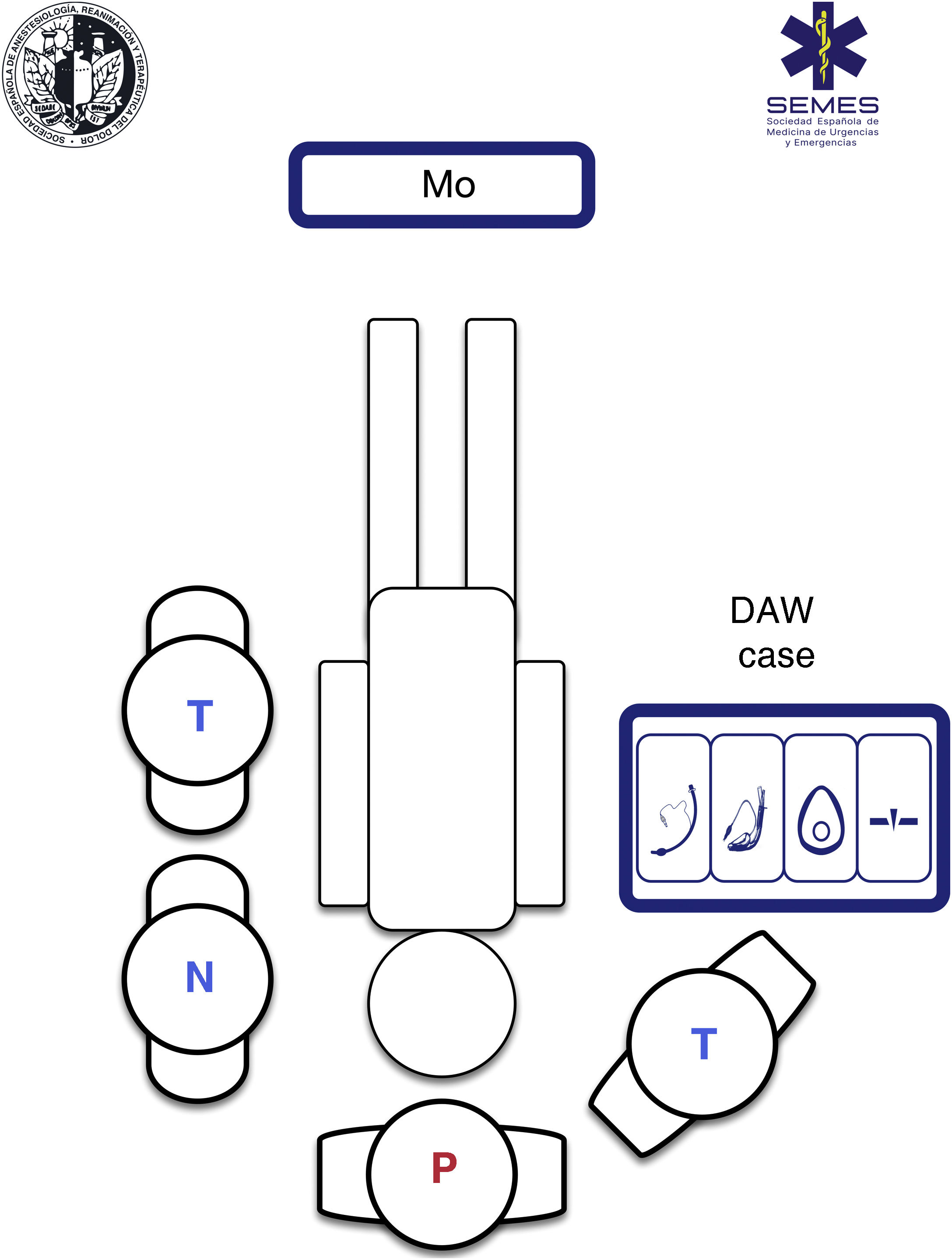
A standardised rapid sequence induction (RSI) procedure is recommended to optimise outcomes, alleviate cognitive load in high-pressure situations, and improve technical and non-technical performance. Therefore, it is desirable to standardise the AW bag, have an ergonomic layout, and a checklist.330Fig. 4 shows the bag and ergonomic layout suggested by SEDAR SEMES SEORL-CCC for the pre-hospital setting.
AW case/bag
Its objective is to store AW material in a standardised way, with a modular design, to keep it visible, accessible in less than a minute and organised in specific compartments for each of the four treatment plans, separated by Velcro® or zips, and marked with easily recognisable pictograms.331 There should be at least one device for each plan (Fig. 4)
For outdoor work, it shall be a transportable, non-rigid case, bag, or rucksack, of reasonable size and weight, labelled, and manufactured in a different colour with approved material that is waterproof, resistant to corrosive agents, and easy to wash and sterilise. It shall have both handles and shoulder straps to free the hands and allow unimpeded access to the patient. Equipment should preferably be checked daily and at shift changes against a checklist.
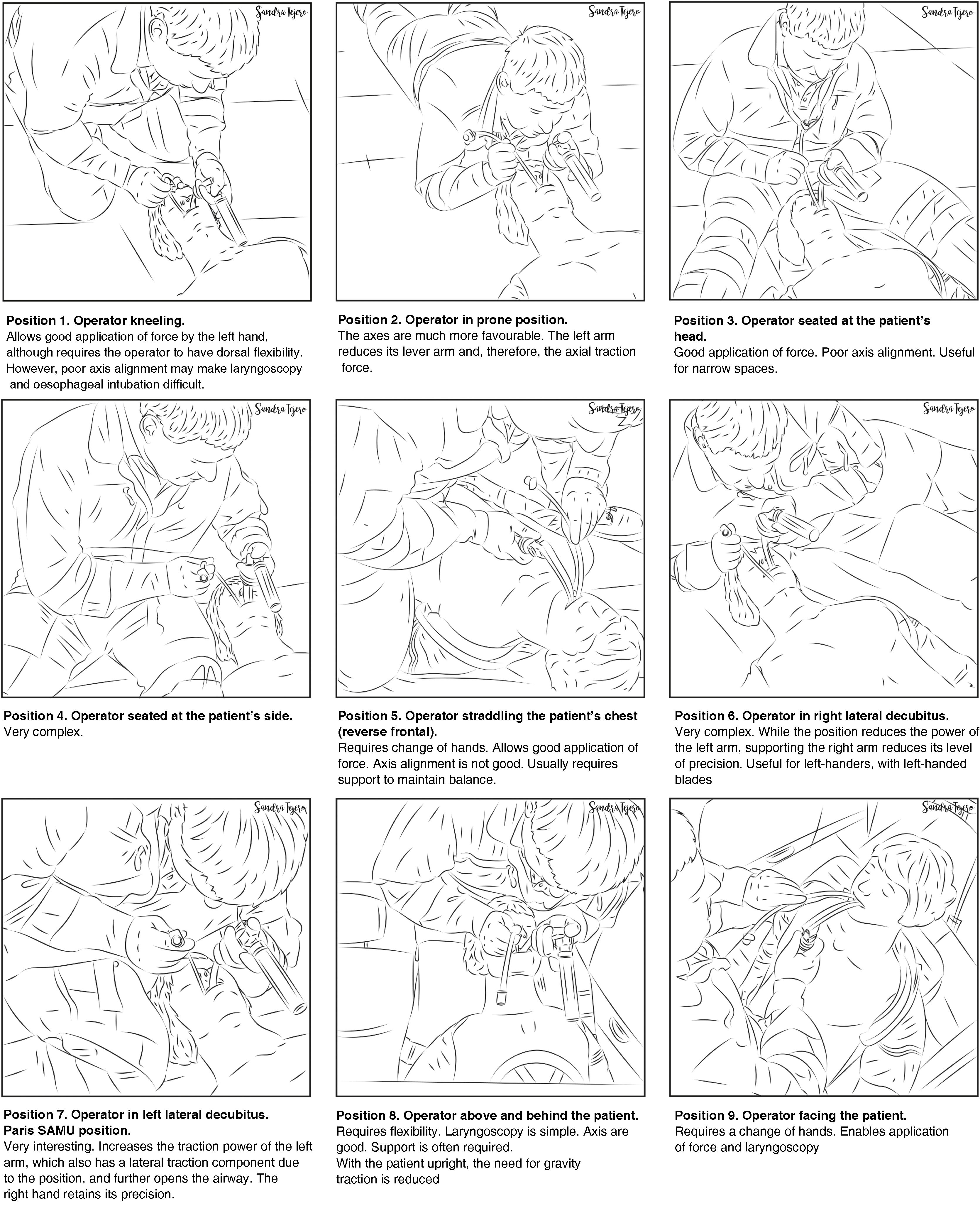
Ergonomics of positions during DAW managementCritical patient care in the pre-hospital environment is based on teamwork, the team usually consisting of a physician, a nurse, and one or more technicians. Therefore, there is usually only one operator.
The multiple scenarios, risks, patients, positions, and obstacles make it necessary to adapt to the setting. Each intervention is unique and unrepeatable. The situation requires accessing and controlling the scene and identifying the most serious subject, determining priorities, and establishing more than one approach plan. Most often the patient is found lying on the ground and a safety roll is possible, although not always. TI on the floor is a predictor of DAW.332 Abnormal positions generate varying degrees of difficult-to-access DAW/AW, necessitating awareness of the anatomical changes and pathophysiology involved (Fig. 5). However, in an ideal scenario, SEDAR SEMES SEORL-CCC suggests the arrangement of team members as shown in Fig. 4. The physician controls ventilation and AW at the patient's head with a technician on their right to support AW management (Sellick, "backward, upward, right lateral position" [BURP], AW enlargement hook, traction support, supply of material, etc.). The nurse and second technician are positioned next to the individual's left shoulder/arm; while the AW case is opened to the right, and the monitor at the feet for proper visualisation. In case of cardiorespiratory arrest (CRA) the monitor should be placed on the subject's left shoulder for better handling.
Pre-procedural assessment and planning
DAW is by definition not anticipated in the pre-hospital setting. However, pre-procedural assessment remains essential to anticipate potential difficulties and plan treatment.331 Predictive tests can be difficult to perform, and, in many cases, there is no time for more than "one second look". This rapid assessment can be useful but, where possible, should be combined with other tests.333
Different series have described as independent predictors of DAW: (1) AW obstruction, intubation, on the floor, and hyoid-mental distance less than three fingers,332 (2) limited space at the scene, short neck, obesity, face and neck injuries, mouth opening less than 3 cm and ankylosing spondylitis,334 and (3) Glasgow scale > 3, limited cervical spine movement, trismus/jaw tension, inability to palpate landmarks in the neck, presence of blood or vomit in the airway.335
For anticipated DAW, it is also recommended that teams have experience in awake TI, although the indications are narrower in emergency TI.336,337
Peri-procedural oxygenationApnoeic oxygenation significantly reduces hypoxaemia during emergency TI,338,339 making it, together with pre-oxygenation, essential for TI in the pre-hospital setting.340 Standard nasal cannulae at 15 L/min should be included from the pre-induction period until TI in daily clinical practice except in patients with epistaxis, severe head trauma with possible skull base fracture, or complex facial fractures because it could worsen TI conditions and cause pneumocephalus.331
Any factors that may influence the success of TI should be optimised prior to the first attempt to achieve the best outcome.
Rapid sequence inductionRSI is the most commonly used method in the pre-hospital setting. However, alternative techniques are of interest.95 It is advisable to follow a standardised RSI procedure using a checklist including drugs, calculation of dose and all available elements.341
Cardiopulmonary resuscitationAny abnormal situation increases the delay in ventilation and alveolar oxygenation, interrupts chest compressions, and delays recovery of spontaneous circulation (ROSC).342
The available evidence does not show strong differences between different non-invasive AW management plans.343–345 Outcomes are conditioned by TI success rates. Therefore, if the desired level of TI efficacy is not achieved, ventilation and alveolar oxygenation should be given preference over the specific treatment plan, taking care not to interfere with other techniques (chest compressions, defibrillation, and treatment of potentially reversible causes of cardiac arrest).328
Severe traumaSevere head trauma carries a high risk of AW obstruction, pulmonary aspiration, hypoxia, brain injury and death.346 Severe head trauma carries a high risk of AW obstruction, pulmonary aspiration, hypoxia, brain injury, and death. Pre-hospital TI is beneficial when performed by experienced physicians following standardised protocols.346,347 Pre-hospital TI together with air transport could reduce overall mortality by 47%.326
Several factors may hinder AW management such as, (1) the possible presence of an unstable cervical spine injury necessitating bimanual alignment, (2) contaminated AW, flooded or pooled by tissue, vomitus, secretions, blood ("bloody airway"), etc., these conditions require aggressive management with manual release of fragments and radical aspiration of secretions using the suction assisted laryngoscopy airway decontamination (SALAD) manoeuvre,349 (3) uncooperative or agitated patient, (4) fractures of the facial mass, and (5) direct trauma to the AW, both penetrating and blunt (AW burn and/or inhalation syndrome). The presence of penetrating cervical trauma is the most frequent indication for awake TI while those with maxillofacial trauma have the highest incidence of FONA.348,350
In these conditions, TI with RSI and VL with hyperangulated blade and preconfigured stylet is recommended.348,351 The impact of sunlight on the screen or the presence of blood or vomitus in the AW may condition the procedure.352 If VL is not available, an SAD or DL with traction reduction can be used.329 The use of DL may increase the risk of cervical spine injury.348,350
Trapped, buried, crushed, or inaccessible patientThis is the paradigm of the difficult-to-access AW. This new field forces teams to expand their knowledge so as to take part in life support manoeuvres for rescue (8 methods) and in hostile environments.353
Cuff pressure monitoringMuch laryngotracheal morbidity is related to inadequate cuff pressure.354 Underinflation may cause hypoventilation or an increased risk of aspiration, while excessive pressure, even for short periods, may cause hoarseness, sore throat, impaired ciliary motility, and injuries such as mucosal swelling and ischaemia, laryngeal oedema, ulceration, stenosis, tracheoesophageal fistula, tracheomalacia, tracheal rupture, vocal cord paralysis, or nerve injury.241,355–357 The incidence of these complications has reduced since the introduction of low-pressure, high-volume cuffs 358; however, the devices used still cause avoidable harm.94,359
Intermittent cuff pressure monitoring by manometry is desirable after cuff pressure is established and periodically during maintenance360–364 (not applicable in crisis situations). The use of continuous monitoring devices to constantly maintain the cuff pressure in range in the critically ill patient may decrease the risk of ventilator-associated pneumonia.365–367 Continuous monitoring with cuff pressure manometry is suggested (1 C).
Cuff pressure should be set at the minimum pressure necessary to ensure an effective and safe seal. The pressure should remain between 20 and 30 cmH2O (ideally less than 25 cmH2O) for ETT and tracheostomy and cricothyrotomy tubes, and < 60 cmH2O for SADs (E.S. 94,3%),241,354,358,368–371 from insertion to removal. If within these limits the seal is inadequate, it may be necessary to reposition the device or resize it.372
Nitrous oxide diffuses into the cuff,359 requiring further measurements after 20 min, when the pressure stabilises, and again if its concentration increases.373
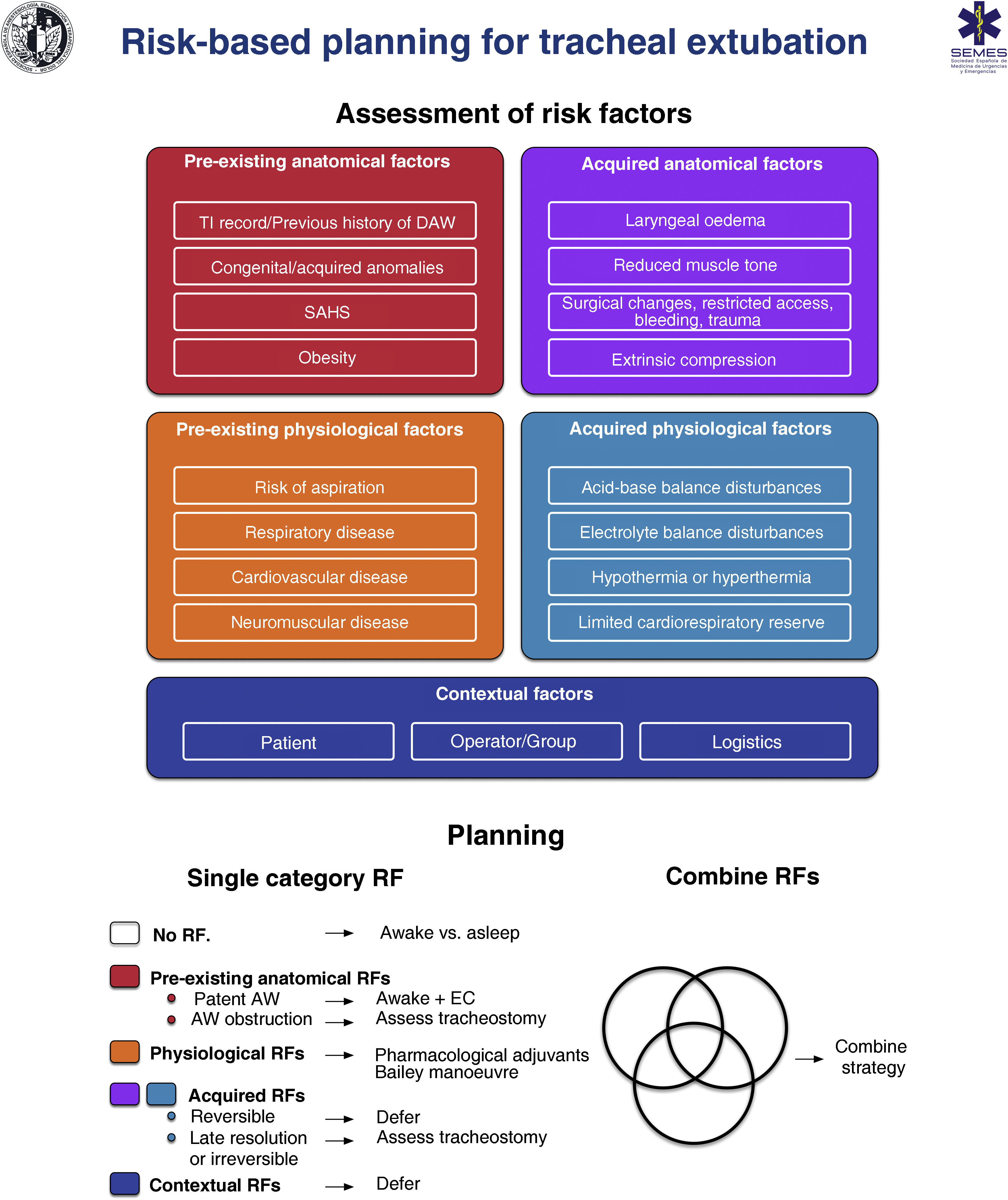
RecommendationExtubationTracheal extubation is a high-risk procedure with major physiological implications.374 It may evoke a haemodynamic response to stress, cough, laryngospasm, or agitation and, secondarily, an increase in intracranial or intraocular pressure.375–378 Protective laryngotracheal reflexes remain impaired for several hours after extubation, facilitating aspiration. Failure of extubation occurs when a patient is unable to maintain oxygenation, adequate ventilation, clearance of secretions, or AW patency and can have catastrophic consequences, particularly in those with DAW.376 AW obstruction is its main cause and is often associated with post-obstructive pulmonary oedema with severe hypoxia.378 Failed extubation, generally defined as the need for reintubation within 24−72 h, occurs in approximately .1%–.45% of general anaesthesia379 and is 10 times more prevalent in patients with sleep apnoea-hypopnoea syndrome (SAHS), or those undergoing AW procedures, and its prevalence is 10-fold higher in critical care areas.380 This is an event with potentially severe outcomes.381–383 Thus, secondary cases of death or permanent brain damage constitute one third of all anaesthesia-related cases.288,384 Poor anticipation and planning for "at-risk" extubation are key issues.288,384 Extubation is an elective procedure that must be prepared for, followed by a stepwise strategy and meticulous follow-up.375,376,378,385Fig. 6 shows a cognitive aid for planning extubation based on risk.

The primary goal in tracheal extubation is to preserve alveolar oxygenation in addition to avoiding reintubation. Any reintubation can be considered potentially difficult as it involves additional complexity (E.S. 97.1%, distorted anatomy with restricted access, secretions, blood or oedema, limited time, and in a high-stress environment).375,376,385 Risk stratification based at anatomical, physiological, and contextual level376,383,386,387 can determine the chances of success conditioned by extubation tolerance and reintubation feasibility, establishing an individualised strategy and optimising AW-related factors and physiological status such as hypoxaemia, hypercapnia, residual NMB, hypothermia, or oedema in the AW.355,383,387 Leak testing,388 preferably quantitative (leak volumes <110 mL or <12%–24% of tidal volume determine reduced AW patency and risk of post-extubation stridor due to laryngeal oedema387,389), ultrasound assessment,390,391 and visualisation of the larynx with VL or FOB can help in decision making (E.S. 97.1%) because they enable assessment of AW patency and determining the presence of periglottic oedema or bleeding prior to extubation,355 although they are not a specific predictive test for successful extubation.392
Once the decision has been made to proceed with extubation, the first step is to review the original TI and update the AW assessment, and general risk factors.383 Careful preparation beforehand, conveying potential problems and early warnings, and establishing appropriate rescue plans for oxygenation and reintubation in case of failure of the primary plan are conducive to safe and successful extubation.378,383 Important prior to intervention378 are (1) pre-oxygenation until extubation, (2) oropharyngeal suctioning of secretions or blood under direct visualisation, ideally with laryngoscopy, to avoid soft tissue trauma, (3) placement of a bite block,386 (4) correct positioning of the patient, (5) reversal of NMB, neuromuscular monitoring in combination with reversal agents aiming for a train-of-four ratio ≥.90 is essential to avoid residual NMB,393–396 (6) minimisation of head and neck movements and reduction of noxious stimuli to avoid laryngospasm, (7) emergence to state of wakefulness,377,378,385–387 "deep extubation" is an inappropriate technique for DAW or when there is risk of aspiration,377,386 (8) apply positive pressure, deflate the cuff and remove the ETT, (9) administer 100% oxygen, confirm AW patency and adequate spontaneous ventilation, and (10) continuous oxygen therapy until full recovery, surveillance, monitoring, and skilled assistance to cope with potential emergency tracheal reintubation.385 The DAW team must be prepared and remain immediately accessible.
Prophylactic administration of corticosteroids prior to elective extubation is associated with a significant decrease in the incidence of post-extubation adverse events in the AW and reintubation, therefore patients at high risk of obstruction may benefit.397–399 In those with absent or reduced leak, administration of a corticosteroid at least four hours prior to extubation is recommended.376,387,389 Prophylactic administration of corticosteroids prior to extubation is suggested in patients at high risk of obstruction (1 B).
There are several advanced methods for at-risk extubation that should only be performed by experienced personnel.378 The administration of pharmacological adjuvants400–405 such as a remifentanil infusion406 or the Bailey manoeuvre, which involves placing a SAD over the ETT and then removing it,407 may be considered when gentle emergence and attenuation of undesirable cardiovascular or respiratory responses is required.408–410 The use of VLMs for TI may have a role to play in safer and simplified TI because they allow the switch to be performed by simply pulling back the ETT through its ventilation channel, vision-guided, and reversing it instantaneously.66 Both techniques require a deep level to perform, and may therefore be inappropriate in patients in whom reintubation may be difficult or there is a risk of aspiration.1,378
Awake extubation using advanced techniques is the most appropriate method for DAW (E.S. 94.3%), because it maintains upper AW patency with re-established muscle tone, protective reflexes, and spontaneous ventilation.410 Airway exchange catheters are the most commonly used adjuvant to salvage extubation in potential or known DAW.1 These devices allow tracheal reintubation by acting as a guide over which the ETT can be reinserted under direct view185 and insufflation of oxygen at low flows or jet ventilation through them in potentially life-threatening hypoxaemia, although this should be avoided as even low flows have caused barotrauma.411 They should be maintained until reintubation is unlikely.376 Their use has been associated with high overall (92%) and first-attempt (87 vs. 14%) success rates, fewer oesophageal intubations, and fewer episodes of desaturation, bradycardia, or hypotension.412 The main risks of the technique are AW stimulation, trauma with subcarinal insertions, and accidental catheter dislodgement. In adults, they should never be inserted deeper than 25 cm from the lips.378 Staged extubation kits consisting of guidewire and reintubation catheter413,414 are associated with an overall success rate of 93%,415 and appear to improve tolerance at the cost of increased accidental dislodgement.416 If reintubation over an intubation catheter is necessary, limiting the difference between the internal diameter of the ETT and the external diameter of the catheter, establishing an appropriate NMB, viewing advancement of the ETT by VL facilitate the procedure by avoiding impingement of the epiglottis and arytenoids.383,417 The remaining recommendations for facilitating FOB-guided TI are equally applicable to exchange catheter-guided TI. Failure of the technique means referring to the unanticipated DAW algorithm.
Capnography should be available in recovery units and used in high-risk cases (E.D. 97.1%). Oxygen therapy with nasal goggles and masks with capnography line after extubation facilitates early detection of respiratory depression, hypoventilation, hypercapnia, or post-extubation AW obstruction.379,387
Strategies to prevent extubation failure include head tilt and supplemental oxygen administration. A good oxygenation strategy with NIV or HFNO may prevent reintubation in at-risk populations.374,418–421
RecommendationDocumentationDocumentation of AW management is necessary to guide future management. In addition to the collection of consent and pre-procedural assessment it should include methods of peri-procedural oxygenation, topicalisation, awake sedation, induction, device, adjuvants and ETT used, approach (right nasal, left nasal, or oral), number of attempts, extubation, and any difficulties or complications. Appendix A, supplementary material 5 shows a template for recording relevant AW-related information.
A history of failure of previous procedures is the most accurate predictor of failure of subsequent treatments (E.S. 97.1%).422 Documenting the difficulty is one of the most important actions to prevent complications as it facilitates decision-making and allows for a targeted structured approach and efficient transition with less instrumentation by avoiding persevering with plans that have failed in previous procedures.422,423 Therefore, it is appropriate to diversify the means of documenting a DAW as this increases the chances of successful transmission of this critical information.423,424 Thus, the following are recommended11,294,424: (1) recording in the electronic history with detailed description and visual record, images and/or video, of the anatomy and the successful technique employed,425 (2) verbal communication to the conscious patient and the family member, guardian, or caregiver, (3) written report to the patient, Appendix A, supplementary material 6 includes the DAW notification template proposed by SEDAR SEMES SEORL-CCC, (4) notification bracelet or necklace or ID card with QR code for access to clinical information, Appendix A, supplementary material 7 shows the means of identifying a DAW suggested by SEDAR SEMES SEORL-CCC, (5) alert each time the electronic patient record is accessed, and (6) entry in national or international databases.426 It is recommended to standardise records with mandatory fields and free text sections to include the characteristics of the AW, the nature of the difficulty, failed and successful techniques.294,424 Structured notes in the electronic record have shown an improvement with reduction of adverse events.427,428
Management in the field of the airwayIn addition to individual commitment, a proactive state, and institutional and departmental involvement are required to implement strategies.429,430 The action plan to improve safety, cost-effectiveness, and quality of care in AW management includes (1) standardisation of practice and equipment in all locations, effective adherence to guidelines, a standardised DAW trolley,431 removal of barriers and application of facilitators,432–434 (2) coordination of departments that manage the AW (anaesthetics, intensive care, ED, ENT, and pre-hospital care), (3) procurement and availability of appropriate equipment, (4) continuous staff training and education, (5) regular audits and error limitation programme: (a) incident analysis, (b) identifying and addressing departmental and institutional factors that may have contributed to the event for learning and implementation of improvements, (c) case review and discussion of alternative plans, (6) incident documentation and notification plans,435 (7) DAW coding, recording, identification and alerting systems, and (8) organisational resource guidelines and continuous process improvement.436,437
Appointing an AW lead in each institution is recommended (E.S. 100%);11,429,430,438 a professional with experience in the field, who liaises with management to assume the actions and organisational aspects indicated. Their primary objective is to provide each professional with the necessary tools.429,439 Some hospitals have set up multidisciplinary teams of specialised staff with defined roles to increase safety.440–442 The creation of a national network of AW leads and teams can enable the field to develop.438,439
Decisions on the procurement of AW devices should be supported by formal evaluation based on scientific evidence.24,443,444
Teaching and trainingAW management is an essential competence in anaesthesiology, critical care, pre-hospital, and emergency medicine.445,446 Poor training is a common causal or contributing factor to complications234,384 and impacts on the confidence operators have in the use of devices and performing essential techniques such as FOB and cricothyrotomy.447–449 Optimising teaching and training is key to increasing safety.322
There is limited evidence and lack of standardisation in AW management teaching,324,450 and therefore strategies are extrapolated from other fields. Good training should include cognitive skills based on theoretical principles and technical and non-technical skills.322,451 Competency acquisition should be gradual, through a cognitive phase, simulation, and clinical training with problem solving until the learning curve is complete, with assessment and feedback from the instructor at each phase (E.S. 100%).437,452,453 Competency-based education requires individualised instruction.454 Training should follow a learning approach consisting of reaching a predefined standard goal of mastery of a skill to escalating levels of difficulty and stress.455 It is a learner-centred, evidence-based method,456 potentially associated with better outcomes.457,458
Education and training should cover all sections of the guidelines in a structured way,37,322,445,455 with special priority given to core, versatile, and time-critical skills.445 Standardisation of a teaching and training programme is highly recommended. Simulation plays a relevant role, mainly in the acquisition of non-technical skills such as teamwork, the incorporation of guidelines and cognitive aids in clinical practice, and the rehearsal of tasks and resolution of rare life-threatening events.437,448,455,459–464 Guidelines and algorithms are training tools for gaining knowledge and learning strategies and act as a resource during debriefing,322,465,466 while cognitive aids are a good implementation tool for rehearsal during simulation.127,322 Structured debriefing improves clinical knowledge, skill acquisition, and implementation of skills in practice.455,467
Operators with greater professional experience may be at risk of providing lower quality care,446,468 and therefore require ongoing education and regular training to develop the new skills needed with the addition of new devices or techniques, and to maintain competencies,322,445,455,469,470 preferably on an annual basis (E.S. 97.1%).471 A proactive organisational and individual attitude is necessary. It is highly recommended that each service designate a local AW lead to promote quality interprofessional and multidisciplinary training programmes, with defined objectives, evaluation and supervision, and to ensure dissemination and adherence to the guidelines and cognitive aids.322,324,439,445,448,472 Training should be diversified to provide the operator with alternatives.43 Appendix A, supplementary material 8 shows the skills recommended by SEDAR SEMES SEORL-CCC that should be included in any AW training programme and the training methods needed to achieve objectives.
Summary of recommendations from the systematic literature searchSearch strategies and GRADE tables are shown in the supplementary material.
| No. | Recommendation | Level of evidence | Grade of recommendation |
|---|---|---|---|
| Pre-procedural assessment and planning | |||
| 1. | A diagnosis of SAHS is a predictor of difficult face mask ventilation | Low | Strong |
| 2. | A diagnosis of SAHS is a predictor of difficult tracheal intubation | Moderate | Strong |
| 3. | Gastric ultrasound examination is recommended to assess the risk of aspiration in at-risk situations | Low | Strong |
| Preparation | |||
| 4. | Capnography waveform is recommended as gold standard to confirm alveolar ventilation | Moderate | Strong |
| 5. | Ramped position or elevated head to 30 ° in the obese population is recommended to improve tracheal intubation conditions | Low | Strong |
| 6. | Ramped position prolongs safe apnoea time in obese populations | Moderate | Strong |
| Peri-procedural oxygenation | |||
| 7. | HFNO is recommended as first-line pre-oxygenation technique for patients with mild hypoxaemia | Low | Strong |
| 8. | NIV is recommended over conventional oxygen therapy for anaesthetic induction in the obese patient | Moderate | Strong |
| 9. | Oxygenation during apnoea with high-flow nasal goggles (NOT DESAT/HFNO) is recommended | Low | Strong |
| Rapid sequence induction | |||
| 10. | Neuromuscular block is recommended to improve TI conditions and the incidence of AW-related adverse events in the general population | Moderate | Strong |
| 11. | The rocuronium + sugammadex combination is not inferior to succinylcholine for RSI | Moderate | Strong |
| Unanticipated difficult airway | |||
| Tracheal intubation | |||
| 12. | The routine use of VL is recommended over DL as the primary device for TI | Moderate | Strong |
| 13. | The use of a dynamic or articulated bougie (flex-tip or FOB type) versus a conventional stylet is recommended for TI in patients with difficult airway | Low | Strong |
| 14. | Parker Flex ETT is recommended over conventional ETT for FOB-guided TI in the general population | Moderate | Strong |
| 15. | Parker Flex ETT over conventional ETT for TI guided by FOB and laryngoscopy in the general population is suggested to reduce complications | Low | Strong |
| Face mask ventilation | |||
| 16. | Face mask ventilation is recommended with modified triple manoeuvre over the C-E technique for the general population | Low | Strong |
| Front-of-neck access | |||
| 17. | Use of ultrasonography over palpation to identify the cricothyroid membrane is recommended | Low | Strong |
| Pressure cuff monitoring | |||
| 18. | Continuous pressure cuff monitoring with manometry is suggested | Low | Strong |
| Extubation | |||
| 19. | Prophylactic administration of corticosteroids prior to extubation in recommended in patients at high risk of AW obstruction | Moderate | Strong |
AW: airway; DL: direct laryngoscopy; ETT: endotracheal tube; FOB: fibrobronchoscopy; HFNO: high-flow nasal oxygen; NIV: non-invasive ventilation; NO DESAT: nasal oxygen therapy during efforts to secure an ETT; RSI: rapid sequence induction; SAHS: sleep apnoea-hypopnoea syndrome; TI: tracheal intubation; VL: videolaryngoscopy.
Expert statement from the results of the Delphi questionnaire| No. | Question | % in favour [in favour; neutral; against] |
|---|---|---|
| Human factors | ||
| 1. | The number of attempts for each non-invasive treatment plan should be limited to three | 88,6 [31; 2; 2] |
| 2. | The first attempt should be made under optimal conditions | 100 [35; 0; 0] |
| 3. | The most appropriate primary technique should be the one that offers the best guarantee of first-attempt success | 94,3 [33; 1; 1] |
| 4. | Visual cognitive aids are recommended for the management of emergency crises | 97,1 [34; 1; 0] |
| 5. | A standardised difficult airway trolley is recommended in areas with AW management | 100 [35; 0; 0] |
| 6. | Use of checklists is recommended to reduce the incidence of human error, improve task completion time, and reinforce a culture of safety in the AW management | 100 [35; 0; 0] |
| 7. | The use of ergonomic and communication models is recommended | 91,4 [32; 3; 0] |
| Pre-procedural assessment and planning | ||
| 8. | Pre-procedural assessment is recommended for all patients requiring AW management | 100 [35; 0; 0] |
| 9. | Pre-procedural assessment of AW should be multifactorial, structured and aimed at detecting anatomical, physiological, and contextual DAW | 97,1 [34; 1; 0] |
| 10. | AW exploration can start by detecting predictors of difficulty or failure for the primary plan and subsequently for the 3 alternative plans | 97,1 [34; 1; 0] |
| 11. | Multivariate models may have a higher predictive power | 97,1 [34; 1; 0] |
| 12. | Decision-making should be individualised according to patient, operator, context, and time | 97,1 [34; 1; 0] |
| 13. | Restriction of food and fluid intake following preoperative fasting guidelines is necessary | 97,1 [34; 1; 0] |
| 14. | The presence of a full stomach indicates that the AW should be protected with TI | 88,6 [31; 2; 2] |
| Preparation | ||
| 15. | Capnography waveform should be available in all AW management sites to assess the success of any of the 4 plans used | 97,1 [34; 1; 0] |
| Basic options for difficult airway management | ||
| 16. | Before each procedure, the appropriateness of the treatment should be assessed, and a risk-benefit analysis performed | 97,1 [34; 1; 0] |
| 17. | Awake management is recommended when there is a high degree of difficulty or impossibility of TI, combined predictors of difficulty, or physiological disturbances, and negative contextual conditions | 82,9 [29; 5; 1] |
| 18. | Induction of general anaesthesia with preservation of spontaneous ventilation is suggested in situations where awake management is recommended but general anaesthesia is unavoidable due to uncooperativeness or urgency, and there are no physiological or contextual predictors of difficulty or obstructive pathology | 91,4 [32; 2; 1] |
| 19. | When physiological or contextual predictors of difficult AW exist, the benefit of deferral may be assessed if it outweighs the risk of proceeding to airway management, or alternative anaesthetic strategies may be considered | 85,7 [30; 5; 0] |
| Known or anticipated difficult airway | ||
| 20. | Awake management is the option of choice to ensure a known or anticipated DAW | 85,7 [30; 4; 1] |
| 21. | High-flow nasal oxygen therapy is recommended over conventional low-flow cannulae | 91,4 [32; 3; 0] |
| 22. | NIV with endoscopic mask may have a role in TI in the critically ill patient with hypoxaemia | 82,9 [29; 6; 0] |
| 23. | Premedication with an antisialogogue is recommended to optimise the efficacy of local anaesthetic efficacy and field of view, glycopyrrolate being the preferred option | 80 [28; 5; 2] |
| 24. | Sedation is an optional adjunct to adequate topical anaesthesia in awake airway management | 88,6 [31; 2; 2] |
| 25. | The goals of conscious sedation for awake AW management are effective amnesia, patient satisfaction, and analgesia to reduce cough, gag, and haemodynamic reflexes, while preserving AW patency, spontaneous ventilation, and protective laryngeal reflexes | 94,3 [33; 2; 0] |
| 26. | If the selected primary technique (FOB or VL) fails, the alternative technique should be used | 80 [28; 6; 1] |
| 27. | A third attempt may benefit from a multimodal approach (VL + FOB) | 100 [35; 0; 0] |
| 28. | The combination of a TI SAD and FOB may be useful as a rescue technique to maintain oxygenation, maintain AW patency and to perform a TI through it | 100 [35; 0; 0] |
| 29. | A smaller than usual ETT is recommended with VL and FOB | 85,7 [30; 4; 1] |
| 30. | Decreasing the difference between the outer diameter of the FOB and the inner diameter of the ETT is recommended to facilitate FOB-guided TI | 85,7 [30; 3; 2] |
| 31. | Standard PVC ETTs are not recommended for FOB-guided TI as they are more likely to impact glottic structures | 71,9 [23; 4; 5] |
| 32. | After visual confirmation of TI, it is recommended to induce general anaesthesia after establishing cuff pressure and capnographic confirmation of TI | 94,3 [33; 2; 0] |
| 33. | Alternative techniques and approaches should be planned in advance and implemented without delay after failure of the primary approaches | 100 [35; 0; 0] |
| 34. | With a high probability of awake TI failure, it is recommended to prepare a FONA in parallel to the invasive treatment plan in case of total obstruction | 88,6 [31; 4; 0] |
| 35. | Awake tracheostomy under local anaesthesia is recommended in the presence of pre-existing critical AW compromise | 82,9 [29; 6; 0] |
| 36. | Awake cricothyrotomy would be the most indicated technique in the presence of emergent critical compromise | 91,4 [32; 3; 0] |
| 37. | Awake ECMO under local anaesthesia may be the safest option when all 4 conventional plans are expected to be impossible, unsuccessful, or ineffective, with risk of full AW obstruction | 90,6 [29; 1; 2] |
| Unanticipated difficult airway | ||
| Peri-procedural oxygenation | ||
| 38. | HFNO should be considered as the first-line pre-oxygenation technique for patients with mild hypoxaemia (PaO2/FiO2 > 200 mmHg), while NIV is the technique of choice in those with severe hypoxaemia (PaO2/FiO2 ≤ 200 mmHg) | 87,5 [28; 3; 1] |
| 39. | Pre-oxygenation with NIV + HFNO and apnoeic oxygenation with HFNO should be a priority option for critically ill patients during TI | 85,7 [30; 4; 1] |
| Rapid sequence induction | ||
| 40. | RSI is the recommended technique when there is a significant risk of aspiration in an AW without predictors of difficulty | 97,1 [34; 1; 0] |
| 41. | RSI with or without Sellick manoeuvre is recommended for all emergency TIs | 84,4 [27; 1; 4] |
| 42. | The use of checklists is suggested for safe preparation of RSI | 97,1 [34; 1; 0] |
| 43. | Premedication with non-particulate antacid immediately before induction and an H2 -receptor antagonist 40−60 min before, or a proton pump inhibitor to increase pH and reduce the volume of gastric contents is suggested in patients at high risk of aspiration | 82,9 [29; 5; 1] |
| 44. | Nasogastric tube treatment should be individualised | 88,6 [31; 4; 0] |
| 45. | Highly efficient suction devices with large multi-hole suction tubes should be available in case of potential regurgitation | 100 [35; 0; 0] |
| 46. | An elevated head position to 20°-30 ° is recommended to prevent passive regurgitation and, if regurgitation occurs, the Trendelenburg position, turning the head to one side and suctioning the oropharynx and trachea before initiating positive pressure ventilation | 94,3 [33; 2; 0] |
| 47. | The choice of hypnotic as well as the dose and speed of administration should be individualised | 91,4 [32; 3; 0] |
| 48. | Delayed sequence induction is suggested in agitated and uncooperative patients for adequate pre-oxygenation | 71,9 [23; 3; 6] |
| 49. | Routine use of cricothyroid pressure cannot be recommended | 81,3 [26; 2; 4] |
| 50. | A "modified RSI" can be applied in patients at high risk of hypoxia who are not candidates for ATI | 85,7 [30; 5; 0] |
| Tracheal intubation | ||
| 51. | Devices with a standard Macintosh-type blade (allows direct and indirect laryngoscopy) are appropriate for AW management without predictors of difficulty, while those with a hyperangulated blade (without or with a guide channel) are indicated for known or anticipated DAW | 94,3 [33; 1; 1] |
| 52. | It is recommended that a bougie be available in all AW management sites | 97,1 [34; 1; 0] |
| 53. | Absence of capnography trace (ventilation grade 3) indicates failed TI until proven otherwise | 80 [28; 6; 1] |
| 54. | Capnography waveform monitoring during maintenance of mechanical ventilation is highly recommended in all sites | 100 [35; 0; 0] |
| Ventilation with supraglottic airway device | ||
| 55. | A SAD should be inserted without delay to preserve alveolar oxygenation in the event of difficult or failed TI | 85,7 [30; 3; 2] |
| 56. | Immediate availability of a second-generation SAD is recommended, as well as competency in its use in all AW management sites | 100 [35; 0; 0] |
| 57. | Cricoid pressure should be released during insertion of an SAD if it is being used | 80 [28; 5; 2] |
| 58. | 90 ° rotation, jaw-thrust, and DL or VL (of choice) with the "insert-detect-correct-as-you-go" technique increase the efficacy and safety of the SAD by facilitating insertion, increase first-attempt success rate, and reduce pharyngeal trauma | 82,9 [29; 4; 2] |
| 59. | FOB-guided TI through the SAD may be chosen if the situation is stable, under adequate NMB and if the operator is competent in the technique | 97,1 [34; 1; 0] |
| Face mask ventilation | ||
| 60. | For FMV it is recommended at the beginning to use the optimal technique (triple manoeuvre of full neck extension, anterior jaw thrust, and mouth opening, placement of oropharyngeal or nasopharyngeal cannula and two-handed V-E technique, in a patient with optimal positioning and strong NMB | 80 [28; 3; 4] |
| 61. | Declaration of failed FMV implies immediate transition to VSAD | 85,7 [30; 2; 3] |
| Front-of-neck access | ||
| 62. | Failure of all 3 non-invasive plans (primary and rescue), regardless of SpO2 value, requires verbalisation of the need for and subsequent FONA | 90,6 [29; 0; 3] |
| 63. | Cricothyrotomy is the technique of choice in a CICO situation | 91,4 [32; 2; 1] |
| 64. | The scalpel-bougie-tube surgical technique is recommended for cricothyrotomy | 91,4 [32; 2; 1] |
| 65. | A FONA should be feasible wherever AW is managed | 100 [35; 0; 0] |
| 66. | Emergency cricothyrotomy should be converted to ETT or tracheostomy because there is insufficient evidence for it as long-term management | 85,7 [30; 3; 2] |
| 67. | Failure of a cricothyrotomy to secure the AW makes it advisable for tracheostomy to be performed by a skilled operator | 94,3 [33; 1; 1] |
| 68. | Any AW management practitioner must acquire and maintain the necessary competency to perform a surgical or percutaneous cricothyrotomy with Seldinger’s technique | 100 [35; 0; 0] |
| Cuff pressure monitoring | ||
| 69. | Cuff pressure should be established at the minimum pressure necessary to ensure an effective and safe seal. Pressure should remain between 20 and 30 cm H2O for ETT and tracheostomy and cricothyrotomy tubes, and < 60 cm H2O for SADs | 94,3 [33; 1; 1] |
| Extubation | ||
| 70. | Any reintubation can be considered potentially difficult as its management involves additional complexity | 97,1 [34; 1; 0] |
| 71. | Leak testing, preferably quantitative, ultrasound assessment, and laryngeal visualisation with VL or FOB may facilitate decision making | 97,1 [34; 1; 0] |
| 72. | Awake extubation with use of advanced techniques is the most appropriate method for DAW | 94,3 [33; 2; 0] |
| 73. | Capnography should be available in recovery units and used in high-risk cases | 97,1 [34; 1; 0] |
| Documentation | ||
| 74. | A history of failure of previous procedures is the most accurate predictor of failure of subsequent management | 97,1 [34; 1; 0] |
| Management in the field of the airway | ||
| 75. | Allocation of an AW lead in each institution is recommended | 100 [35; 0; 0] |
| Teaching and training | ||
| 76. | Competency acquisition should be gradual, through a cognitive phase, simulation, and clinical training with problem-solving until the learning curve is complete, with assessment and feedback from the instructor at each phase | 100 [35; 0; 0] |
| 77. | Ongoing teaching and regular training are required for the development of new skills or techniques and the maintenance of competencies, preferably on an annual basis | 97,1 [34; 1; 0] |
AW: airway; CICO: can’t-intubate-can’t oxygenate situation; DAW: difficult airway; DL: direct laryngoscopy; ECMO: extracorporeal membrane oxygenation; ETT: endotracheal tube; FOB: fibrobronchoscopy; FiO2: fraction of inspired oxygen; FONA: Front-of-neck access; HFNO: high-flow nasal oxygen therapy; FMV: face mask ventilation; NIV: non-invasive ventilation; NMB: neuromuscular block; PaO2: partial arterial pressure of oxygen; PVC: polyvinyl chloride; RSI: rapid sequence induction; SAD: supraglottic airway device; 2 GSAD: second generation supraglottic airway device; SpO2: peripheral oxygen saturation; TI: tracheal intubation; VSAD: Ventilation with supraglottic airway device; VL: videolaryngoscopy.
Authors’ contribution- •
Manuel Á. Gómez-Ríos: drafting of the manuscript, preparation of all cognitive aids and graphic material, tables and annexes, literature review, critical reading, levels of evidence, final revision of the document.
- •
José Alfonso Sastre: Draft of RSI sections, SAD, and checklist, risk factor tables, information document models, literature review, critical reading, levels of evidence, final revision of the document.
- •
Xavier Onrubia-Fuertes: FONA contribution, unanticipated difficult tracheal intubation, literature review, final revision of the document.
- •
Teresa López: Draft of SAD and ECMO sections, literature review, critical reading, levels of evidence, final revision of the document.
- •
Alfredo Abad-Gurumeta: literature review, critical reading, levels of evidence, final revision of the document.
- •
Rubén Casans-Francés: literature review, critical reading, final revision of the document.
- •
David Gómez-Ríos: literature review, critical reading, final revision of the document.
- •
José Carlos Garzón: literature review, critical reading, final revision of the document.
- •
Vicente Martínez-Pons: Algorithm for unanticipated difficult tracheal intubation, literature review, final revision of the document.
- •
Marta Casalderrey-Rivas: literature review, critical reading, final revision of the document.
- •
Miguel Ángel Fernández-Vaquero: Algorithm for unanticipated difficult tracheal intubation, literature review, and critical reading aimed at AW predictors and assessment, final revision of the document.
- •
Eugenio Martínez-Hurtado: Algorithm for unanticipated difficult tracheal intubation, final revision of the document.
- •
Ricardo Martín-Larrauri: Algorithm for unanticipated difficult tracheal intubation, final revision of the document.
- •
Laura Reviriego-Agudo: Algorithm for unanticipated difficult tracheal intubation, literature review, final revision of the document.
- •
Uxía Gutierrez-Couto: literature search strategies.
- •
Javier García-Fernández: critical reading, final revision of the document.
- •
Alfredo Serrano Moraza: prehospital setting section, literature review, critical reading, final revision of the document.
- •
Luis Jesús Rodríguez Martín: prehospital setting section, final revision of the document.
- •
Carmen Camacho Leis: prehospital setting, final revision of the document.
- •
Salvador Espinosa Ramírez: prehospital setting, final revision of the document.
- •
José Manuel Fandiño Orgeira: critical reading, final revision of the document.
- •
Manuel José Vázquez Lima: critical reading, final revision of the document.
- •
Miguel Mayo-Yáñez: FONA contribution, final revision of the document.
- •
Pablo Parente-Arias: FONA contribution, final revision of the document.
- •
Jon Alexander Sistiaga-Suárez: critical reading, final revision of the document.
- •
Manuel Bernal-Sprekelsen: critical reading, final revision of the document.
- •
Pedro Charco-Mora: Coordination, Algorithm for unanticipated difficult tracheal intubation, draft ergonomic options, draft teaching and training, literature review, critical reading, final revision of the document
MAGR received lecture honoraria from Medtronic.
XOF received honoraria for lecture and practical workshop on neuromuscular block from Merck Sharp & Dohme.
RCF received honoraria for lectures from Fresenius Kabi.
AAG received honoraria for lectures from Merck Sharp & Dohme and 3 M Edwards.
Delphi expert panelManuel Á. Gómez-Ríos, José Alfonso Sastre, Xavier Onrubia-Fuertes, Teresa López, Alfredo Abad-Gurumeta, José Carlos Garzón, Vicente Martínez-Pons, Marta Casalderrey-Rivas, Miguel Ángel Fernández-Vaquero, Eugenio Martínez-Hurtado, Ricardo Martín-Larrauri, Laura Reviriego-Agudo, Javier García-Fernández, Pedro Charco-Mora, Raquel García Álvarez, Alfredo Panadero Sánchez, Alejandra Prieto Gundín, María Luisa Santos Marqués, David Domínguez García, Irma, María Barrio, Uxío García-Aldao, Aixa Espinosa, Carmen M. Holgado Pascual, Jesús Carazo Cordobés, Cristobal Añez Simón, Natividad Quesada Gimeno, Marina Gómez-Morán Quintana, Silvia Bermejo, Pilar Cabrerizo Torrente, Francisca Llobell, Roque J. Company Teuler, Teresa del Castillo Fdez de Betoño, Carlos González Perrino, and Paola Hurtado.
External reviewersJaideep Pandit, Luis Gaitini, Tomasz Gaszyński, and Pavel Michalek
ContributorsA list of contributors can be found in the supplementary material.
AcknowledgementsWe would like to thank Sandra Tejero Muñoz for illustrating figure 5 of this consensus document.
The following are Supplementary data to this article:
