



Advances in clinical applications of computed tomography have been accompanied by improvements in advanced post-processing tools. In addition to multiplanar reconstructions, curved planar reconstructions, maximum intensity projections, and volumetric reconstructions, very recently kinematic reconstruction has also been developed. This new technique, based on mathematical models that simulate the propagation of light beams through a volume of data, makes it possible to obtain very realistic three-dimensional images. This article illustrates examples of kinematic reconstructions and compares them with classical volumetric reconstructions in patients with cardiovascular disease in a way that makes it easy to establish the differences between the two types of reconstruction.
ConclusionKinematic reconstruction is a new method for representing three-dimensional images that facilitates the explanation and comprehension of the findings.
El avance en aplicaciones clínicas en tomografía computarizada se ha acompañado de mejoras en herramientas de posproceso avanzado. Además de las reconstrucciones multiplanares, planares curvas, de proyección de máxima intensidad y de las reconstrucciones volumétricas, muy recientemente se ha desarrollado la reconstrucción cinemática como técnica que, basada en modelos matemáticos que simulan la de propagación de los haces de luz a través de un volumen de datos, permite obtener imágenes tridimensionales de gran realismo. En este trabajo se ilustran y comparan ejemplos de reconstrucciones cinemáticas respecto a reconstrucciones volumétricas clásicas en pacientes con patología cardiovascular, de manera que se pueden establecer fácilmente las diferencias entre ambos tipos de reconstrucción.
Conclusiónla reconstrucción cinemática es un nuevo modo de representar la imagen tridimensional, que facilita la explicación y la comprensión de los hallazgos.
Computed tomography (CT) scanning has become one of the most advanced imaging modalities during the last few decades. Cardiovascular imaging is one of its many clinical applications.1 These days, we can use it to study the heart and major blood vessels with great imaging sharpness and high definition. The great anatomical detail provided by modern machines has also facilitated the visualization and assessment of small-caliber blood vessels such as coronary arteries, and very distal pulmonary branches, in such a way that, for example, we can find small emboli that may go unnoticed in other machines.2 Today cardiac studies can be conducted in less than a heartbeat, and thoracic studies in less than a second.3 These examinations can also be conducted with the lowest possible radiation doses.4
The advances made in new clinical applications also require the development of advanced post-processing tools. To this end, techniques need to be not only intuitive, but also easy to use, provide clinical information, and impact the diagnosis and clinical management of the patients.
In this paper, we will go over the technique known as cinematic rendering (CR) as a new and advanced post-processing technique; also, a few examples will be shown here comparing this type of reconstruction to the one obtained after implementing the method of conventional volume rendering (VR) in order to be able to see the photo-realistic effect achieved with the CR technique.
We should remember that the advances made in new clinical applications also require the development of advanced post-processing tools.
Post-processing techniques in CT scansTraditionally, CT scans have been based on reading and interpreting axial images. It was not until the arrival of multi-slice isotropic imaging CT machines that we started talking about post-processing techniques and tools as such.5 Among these post-processing techniques, we find the multiplanar reconstruction, the curved planar reformation, the maximum intensity projection, and VR.6 The latter type of reconstruction is based on complex algorithms which are in turn based on the attenuation of the voxels that make up the image. In the images, each voxel contains different types of tissue, and each tissue is represented by a given percentage based on a predefined threshold of attenuation to which color and opacity are assigned. The different ranges of density usually look like a trapezium or trapezoid, with a gradual scale of colors that allows overlapping and mixing of the different ranges of attenuation. The ultimate color and opacity of each voxel depends on the weighted sum of these different values. The simulation of how this volume behaves under the illumination of a certain number (one to three) of foci provides that extra “realistic” effect that the images have.7 Since all the study data are used to generate volume rendering, the final result is the spitting image of the organ studied. Volume rendering is usually used, for example, to show the origin and trajectory of thoracic blood vessels on suspicion of an anomaly,8 to confirm the outcome of an intervention9 and to plan surgical treatment, above all, in patients who are going to be operated.6,10
We should remember that VR is based on complex algorithms which are in turn based on the attenuation of the voxels that make up the image.
Cinematic renderingThe CR technique is a new method of 3D reconstruction based on technical models of light propagation through one volume of data to eventually create one 3D image. This technique is more realistic than conventional VR reconstructions.11–14 The CR was originated in the cartoon industry.14 The scheme for the production of 3D images is similar to the one used by the VR technique since it also assigns colors and opacities to the attenuation values of each voxel. The main difference between both types of reconstructions is that each pixel is not created by the passing of one single beam of light through the volume of data; instead, the CR algorithm uses a model of global illumination to simulate the passing of billions of photons from all possible directions through such volume—something similar to what happens with natural lighting. This interaction between the photons and the volume generates pixels that make up the image with great 3D photo-realism.12 The mathematical equation underneath this process of image generation is very complex and has been explained in the Monte Carlo integration formula.15 The ultimate realism of the image is due to the representation of a high dynamic range of the light maps used to create a setting of maps of natural lighting. Therefore, not just one beam of light per pixel is used to generate the final volume as it occurs during VR, but rather it is the effects of natural lighting provided by the other adjacent voxels that are used to generate certain effects in the resulting image such as shadows or reflections that will give an appearance of depth that is so characteristic of this type of reconstruction.11
In order to be able to process cinematic reconstructions, the properties of the photographic image such as exposure time, aperture, and focal plane are used, and they can be manipulated in order to give more depth and volume, or to enhance certain aspects of the image. These possibilities add up to the properties of any post-processing technique, such as the capacity to cut the image through define planes or free edges or contours drawn mannually.14
We should remember that the CR technique is a new method of 3D reconstruction based on technical models of light propagation through one volume of data for the creation of hyper-realistic 3D images.
Applications in cardiovascular imagingThe clinical applications of CR are similar to those of VR since they both are volumetric representations of 3D reconstructions. However, the CR has an added value compared to the VR since the resulting images seem to have greater depth and are more truth to reality.16
The CR allows us to show, with high definition, the anatomical relations that exist among different vascular structures such as cases of congenital heart conditions (Fig. 1), or an anomalous pulmonary vein drainage (Fig. 2). On top of showing the condition of major blood vessels, the CR is an excellent method to show the anomalies of coronary vascularization (Fig. 3). From the surgical point of view, in operated patients, it allows us to see the postoperative outcome (Fig. 4), and in patients requiring re-interventions, it gives us a global vision of the thorax and the anatomical relations of the structures of interest, thus facilitating surgical approach (Fig. 5).
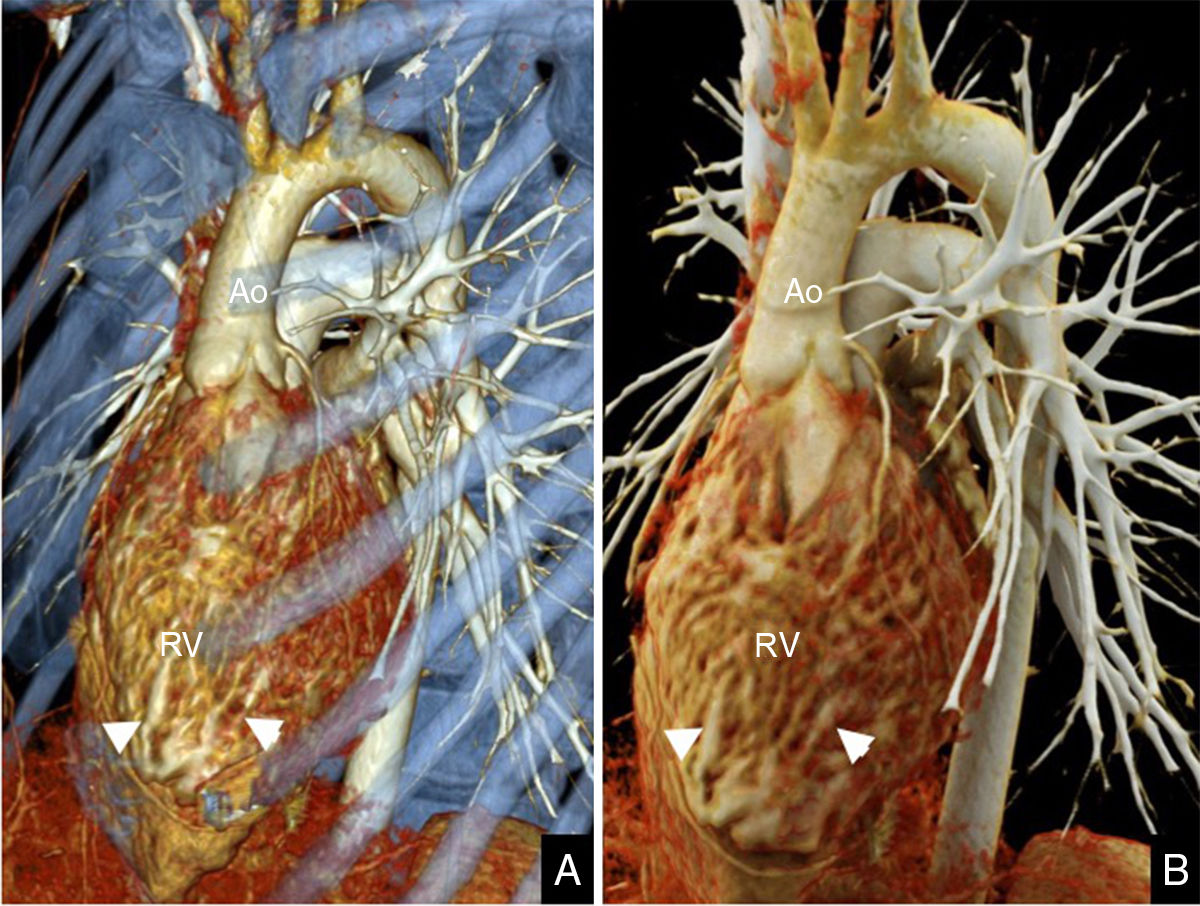
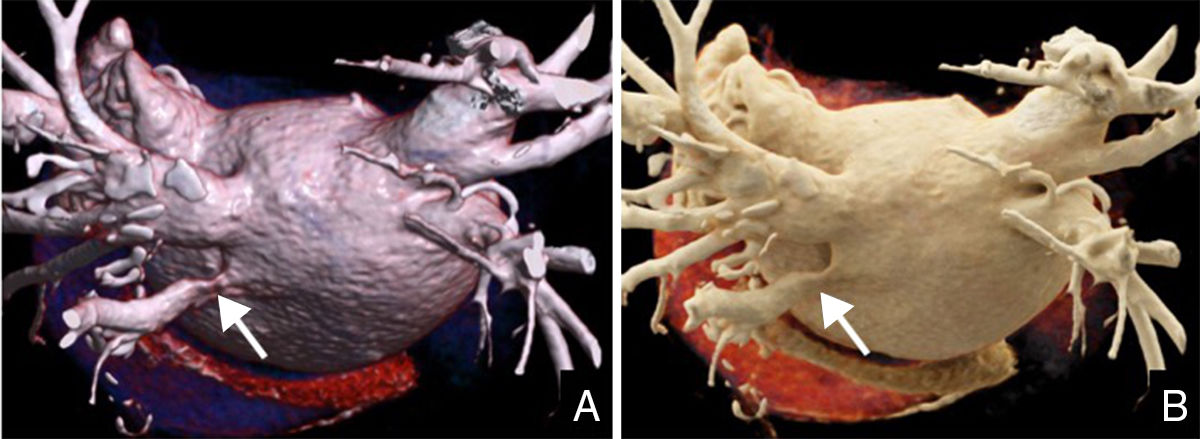
 Volume rendering. (B) Cinematic rendering. Note the patient's mismatch between the arterial and ventricular systems: the aorta originates (Ao) from the morphologically right ventricle (RV) that shows hypertrophy of the moderator band (arrowheads).")
Thoracic angio-CT scan in an 18-year-old male diagnosed of congenital heart disease of the kind of congenitally corrected transposition of the great arteries due to ventricular inversion. (A) Volume rendering. (B) Cinematic rendering. Note the patient's mismatch between the arterial and ventricular systems: the aorta originates (Ao) from the morphologically right ventricle (RV) that shows hypertrophy of the moderator band (arrowheads).
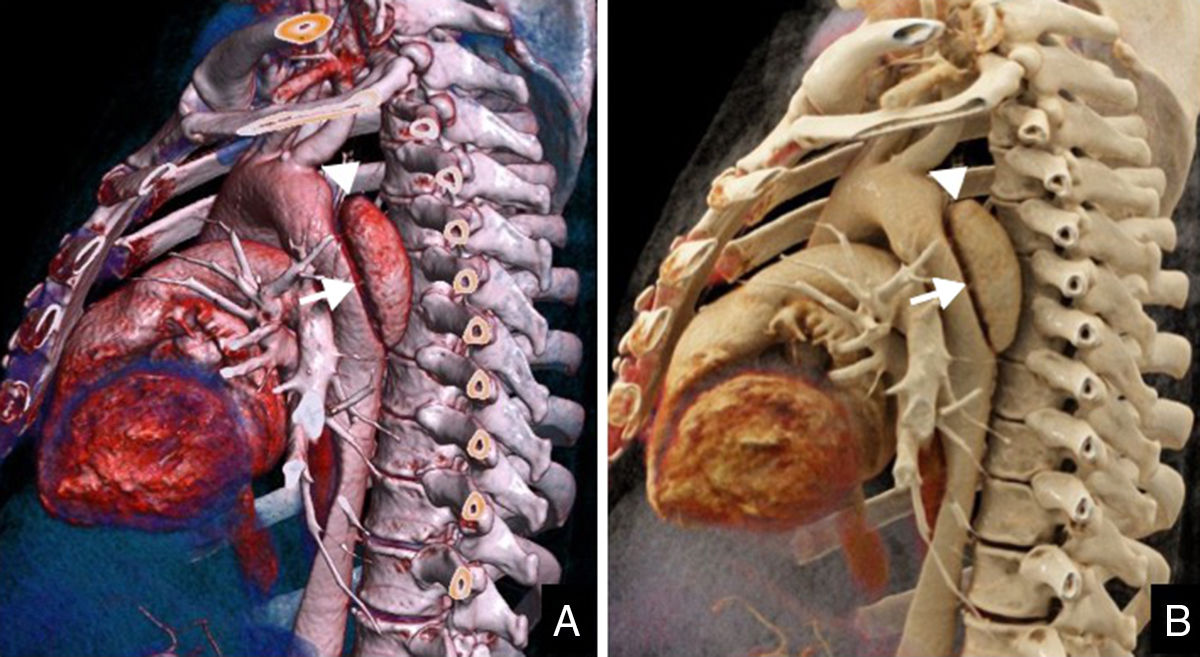
 Volume rendering. (B) Cinematic rendering. The study showed a scimitar-like large right vertical vein picking up venous blood from the right lung (arrows) toward the suprahepatic inferior vena cava (arrowheads). One cardiac MRI conducted to establish the hemodynamic compromise showed the presence of left–right shunt (Qp/Qs=1.5). After evaluation by a multidisciplinary team, medical therapy was prescribed.")
Thoracic angio-CT scan in a 70-year-old acyanotic female with a history of systemic arterial hypertension, hypercholesterolemia, and paroxysmal atrial fibrillation. The thoracic X-ray conducted at a different center confirms the presence of cardiomegaly, dextroposition of the cardiac silhouette, right lung hypoplasia, and signs of pulmonary hypertension. One angio-CT scan was conducted to confirm the diagnosis. (A) Volume rendering. (B) Cinematic rendering. The study showed a scimitar-like large right vertical vein picking up venous blood from the right lung (arrows) toward the suprahepatic inferior vena cava (arrowheads). One cardiac MRI conducted to establish the hemodynamic compromise showed the presence of left–right shunt (Qp/Qs=1.5). After evaluation by a multidisciplinary team, medical therapy was prescribed.
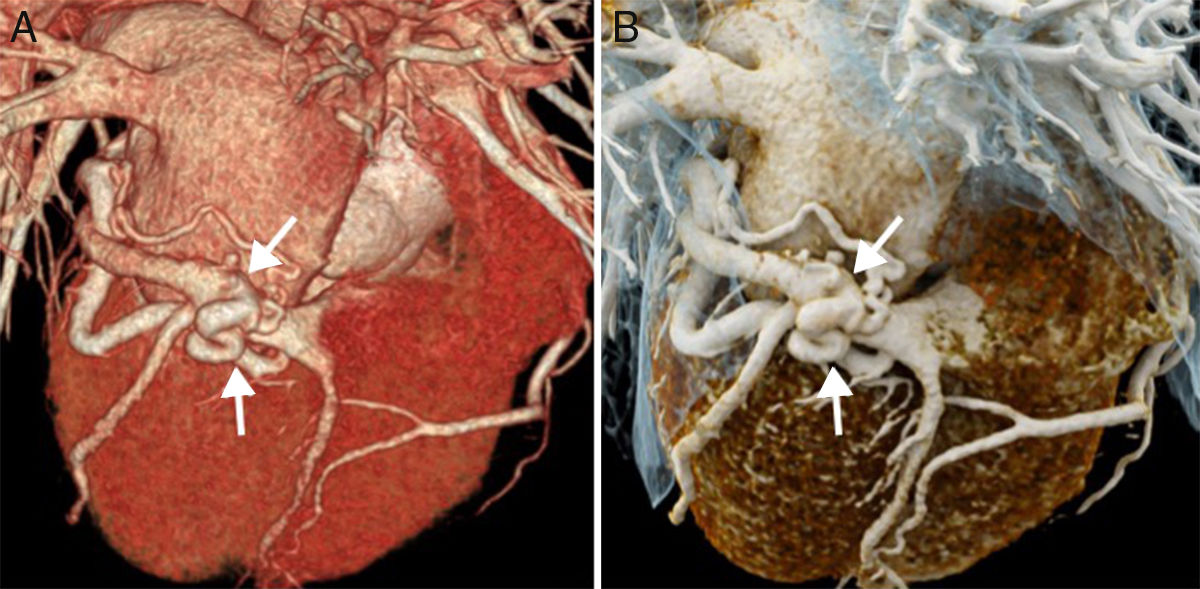
 in a 72-year-old female with hypercholesterolemia and possible obstructive sleep apnea syndrome. She has remained asymptomatic from the cardiovascular point of view; however, 7 years ago she started experiencing dyspnea that she now experiences while trying medium-level efforts and consequently limits her daily activities. Occasionally, she would have suprasternal rhythmic and fast palpitations. One CCTA was requested in order to rule out coronary disease. (A) Volume rendering. (B) Cinematic rendering. The study showed one circumflex artery of a larger caliber and a winding trajectory that was more obvious in its distal third. There was direct communication between such artery and the great cardiac vein before entering the coronary sinus (arrows). Since this finding was not considered responsible for the patient's symptoms, it was agreed to keep monitoring the patient.")
Coronary computed tomography angiography (CCTA) in a 72-year-old female with hypercholesterolemia and possible obstructive sleep apnea syndrome. She has remained asymptomatic from the cardiovascular point of view; however, 7 years ago she started experiencing dyspnea that she now experiences while trying medium-level efforts and consequently limits her daily activities. Occasionally, she would have suprasternal rhythmic and fast palpitations. One CCTA was requested in order to rule out coronary disease. (A) Volume rendering. (B) Cinematic rendering. The study showed one circumflex artery of a larger caliber and a winding trajectory that was more obvious in its distal third. There was direct communication between such artery and the great cardiac vein before entering the coronary sinus (arrows). Since this finding was not considered responsible for the patient's symptoms, it was agreed to keep monitoring the patient.
 Volume rendering. (B) Cinematic rendering. The angio-CT scan confirmed aortic re-coarctation (arrows). Given the lack of symptoms and the lack of a significant gradient in the echocardiography, conservative management was prescribed with further exploration.")
Thoracic angio-CT scan in a 32-year-old female diagnosed of aortic coarctation in her infancy and operated through aortoplasty. She comes to her regular check-up remaining asymptomatic from the cardiovascular point of view. (A) Volume rendering. (B) Cinematic rendering. The angio-CT scan confirmed aortic re-coarctation (arrows). Given the lack of symptoms and the lack of a significant gradient in the echocardiography, conservative management was prescribed with further exploration.
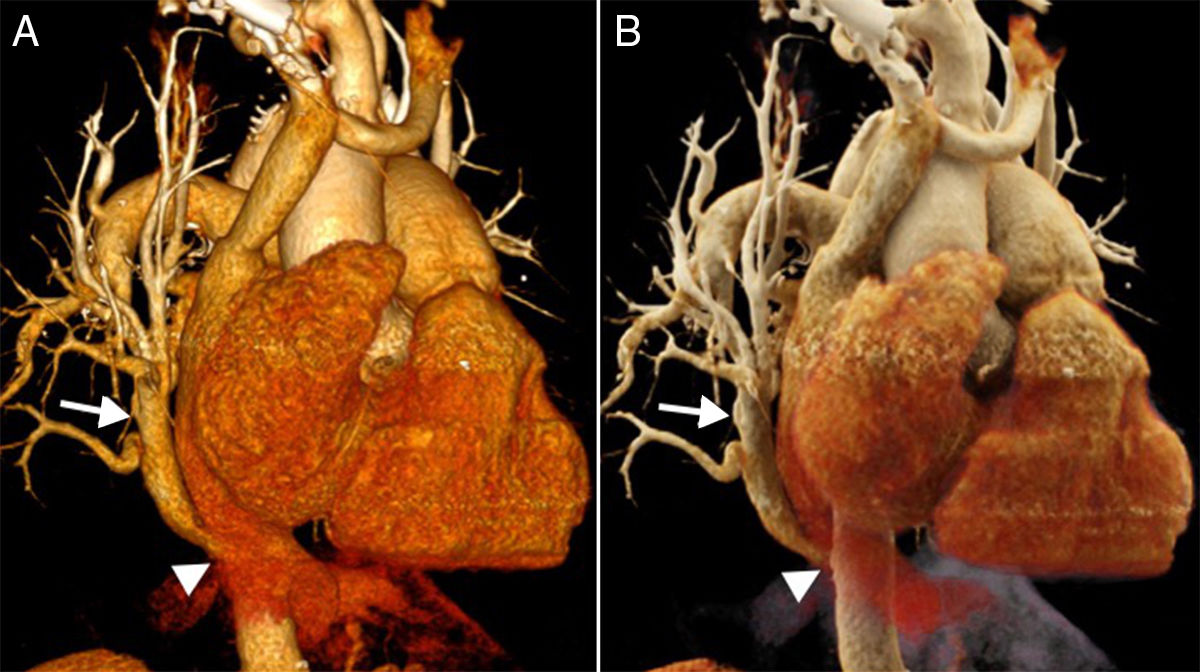
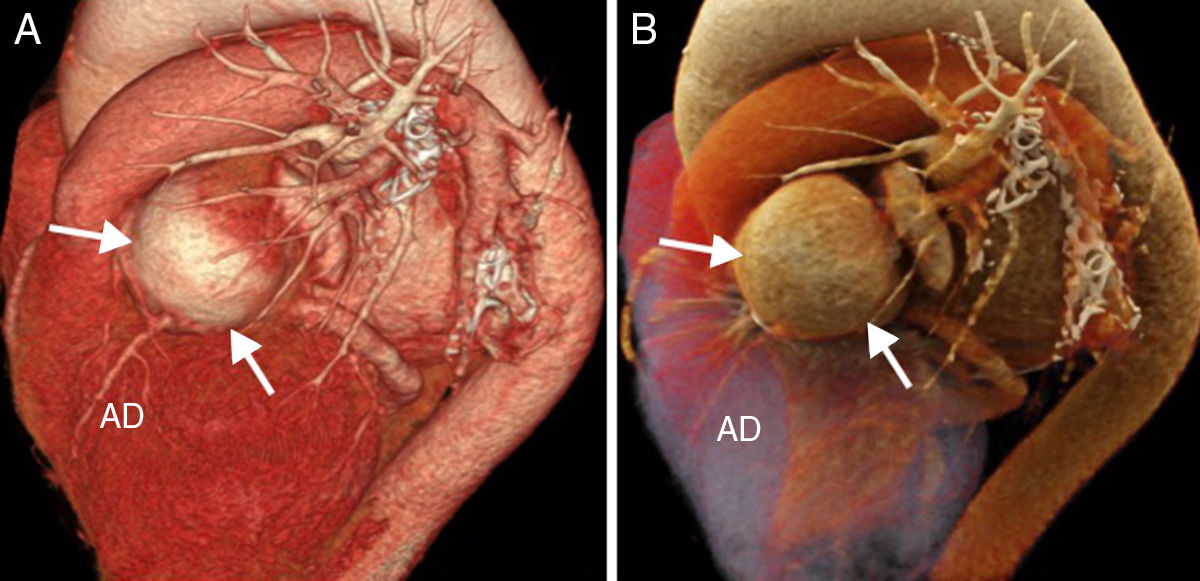
 in a 67-year-old female in permanent atrial fibrillation and with a history of mitral aortic valve replacement. The echocardiographic examination showed an image suggestive of subvalvular pannus in the aortic valve with high velocity that was indicative of severe aortic stenosis. One CCTA was requested in order to assess the state of the patient's coronary arteries before proceeding with the intervention. (A) Volume rendering. (B) Cinematic rendering. The CCTA showed one aneurysm in the ostium and trunk of the left coronary artery of 45×47mm in diameter (arrows), and one anterior descending (AD) coronary artery of normal characteristics and without stenosis. The patient was operated through aortic valve replacement with valved graft, saphenous vein graft to the anterior descending coronary artery, and anastomosis of the right coronary to the valved graft. The circumflex artery could not be found during the intervention. The left coronary trunk was ligated at its origin for the closure of the aneurysmal sac. The patient's progression after the surgery was satisfactory.")
Coronary computed tomography angiography (CCTA) in a 67-year-old female in permanent atrial fibrillation and with a history of mitral aortic valve replacement. The echocardiographic examination showed an image suggestive of subvalvular pannus in the aortic valve with high velocity that was indicative of severe aortic stenosis. One CCTA was requested in order to assess the state of the patient's coronary arteries before proceeding with the intervention. (A) Volume rendering. (B) Cinematic rendering. The CCTA showed one aneurysm in the ostium and trunk of the left coronary artery of 45×47mm in diameter (arrows), and one anterior descending (AD) coronary artery of normal characteristics and without stenosis. The patient was operated through aortic valve replacement with valved graft, saphenous vein graft to the anterior descending coronary artery, and anastomosis of the right coronary to the valved graft. The circumflex artery could not be found during the intervention. The left coronary trunk was ligated at its origin for the closure of the aneurysmal sac. The patient's progression after the surgery was satisfactory.
Thus, cinematic rendering is one imaging modality that gives us more realism than conventional VR without detriment to its diagnostic performance (Fig. 6). The CR is a new way to show the anatomy more intuitively than in all other imaging post-processing techniques that we can use in cardiovascular imaging as a tool to facilitate the explanation and understanding of the imaging findings and, eventually, communication among clinicians, surgeons, and patients (Figs. 7–9). This type of reconstructions can be particularly useful for teaching purposes to students and residents.
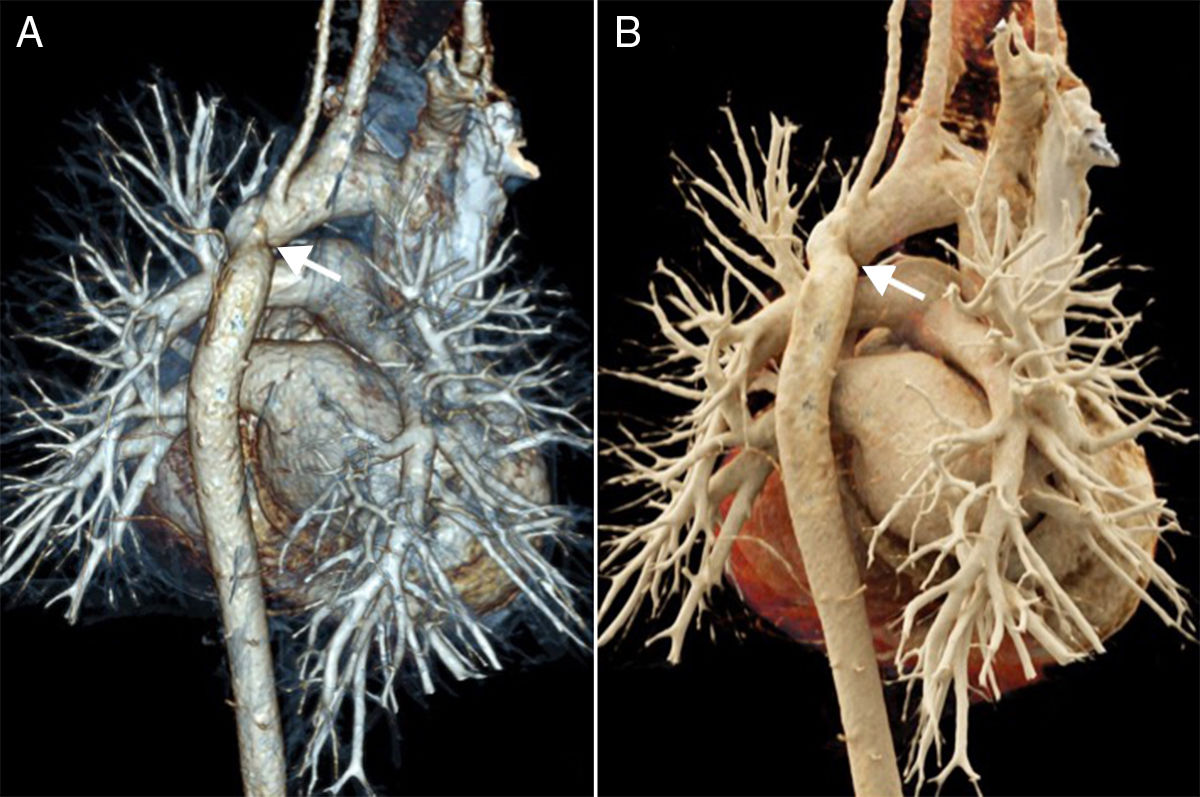
 Volume rendering. (B) Cinematic rendering. The study showed pulmonary thromboembolism affecting the left main pulmonary artery and spreading toward the left inferior lobar artery (arrows). No pulmonary infarction was confirmed.")
Pulmonary angio-CT scan in a 52-year-old male with orthotopic heart transplant due to dilated cardiomyopathy. After spending 1month with pain in his left leg and knee, the patient came to his GP's office showing dyspnea. One angio-CT scan was conducted in order to rule out thromboembolism. (A) Volume rendering. (B) Cinematic rendering. The study showed pulmonary thromboembolism affecting the left main pulmonary artery and spreading toward the left inferior lobar artery (arrows). No pulmonary infarction was confirmed.
. One angio-CT scan was conducted in order to rule out aortic dissection. (A) Volume rendering. (B) Cinematic rendering. The study confirmed one DeBakey type III aortic dissection (arrows) originated distal to the left subclavian artery (arrowheads) and spreading across the thoracoabdominal aorta until the right iliac artery.")
Aortic angio-CT scan in a 42-year-old male who presented to the ER complaining of interscapular pain after physical exercise with resistance to analgesia; the patient was hypertensive upon arrival to the hospital (PA 200/100mmHg). One angio-CT scan was conducted in order to rule out aortic dissection. (A) Volume rendering. (B) Cinematic rendering. The study confirmed one DeBakey type III aortic dissection (arrows) originated distal to the left subclavian artery (arrowheads) and spreading across the thoracoabdominal aorta until the right iliac artery.
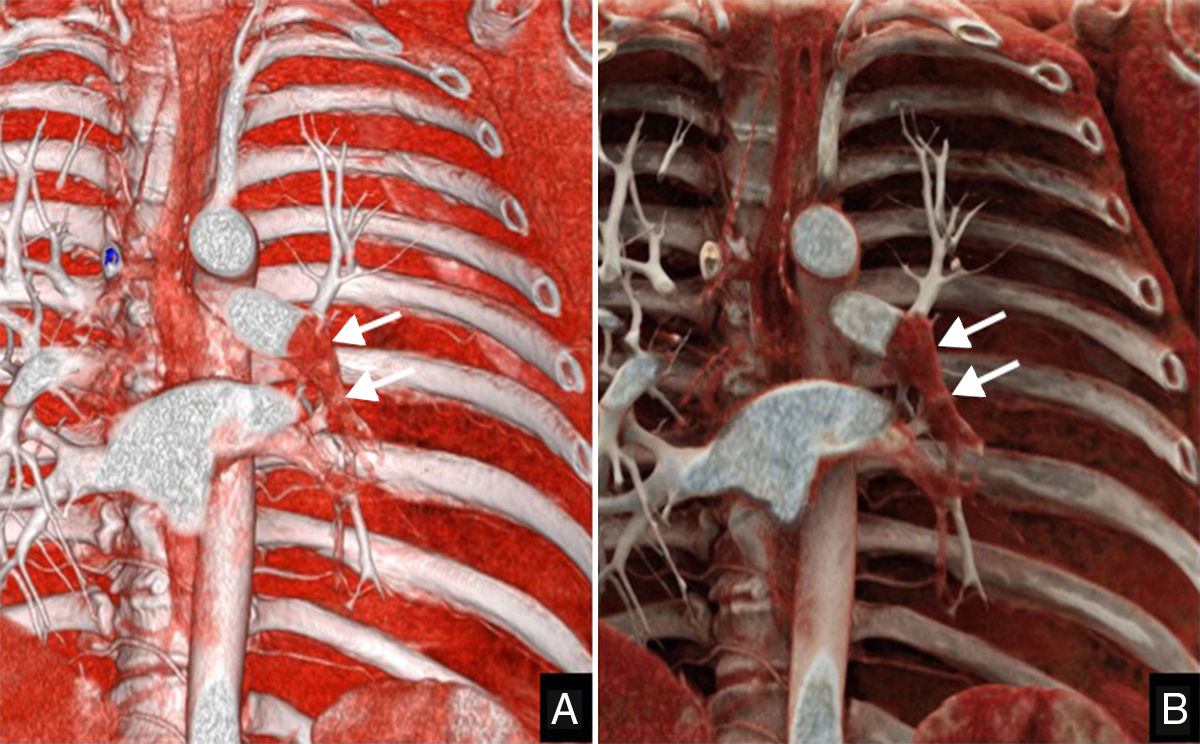
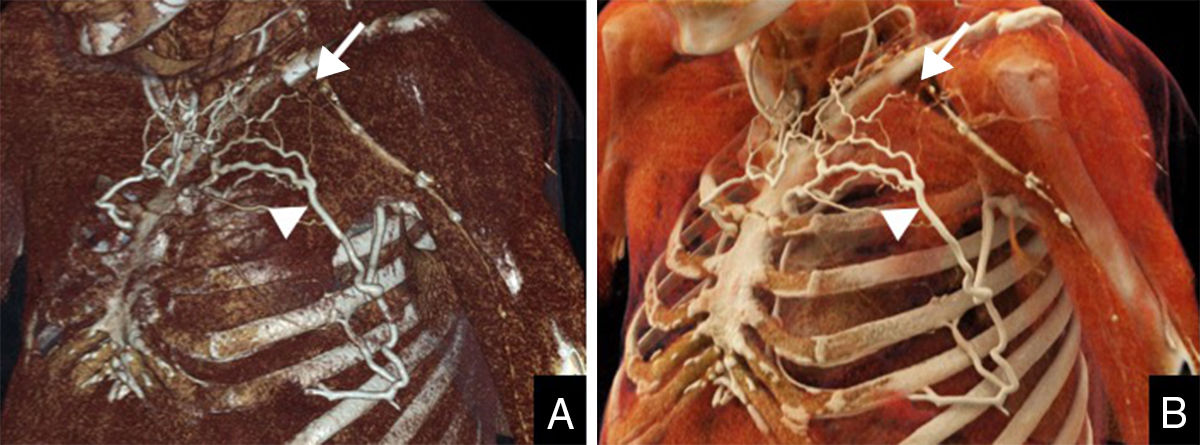
 in a 41-year-old male with diabetes, dyslipidemia, and a personal history of ischemic cardiomyopathy treated with stents. The patient was evaluated following bilateral thoracic outlet syndrome, asymptomatic in the left side, that was operated through resection of the first rib. There was a torpid postoperative period. One CTV was requested in order to assess the patency of the left subclavian vein because, while in the postoperative care, the mobility of the patient's fingers got worse and was associated to paresis and pain in the patient's left hand and forearm. (A) Volume rendering. (B) Cinematic rendering. The patient showed postoperative changes in the left subclavian region after resection of the left transverse apophysis and partial resection of the patient's left first rib and lack of opacification (thrombosis) of the proximal third of the left subclavian vein along 3.5cm (arrows). The distal venous system of such limb was patent. An abundant collateral circulation was evident (arrowheads), above all in the anterior thoracic wall and, to a lesser extent, in the resection bed, draining into the venous brachiocephalic trunk and the left jugular vein.")
Thoracic computed tomography venography (CTV) in a 41-year-old male with diabetes, dyslipidemia, and a personal history of ischemic cardiomyopathy treated with stents. The patient was evaluated following bilateral thoracic outlet syndrome, asymptomatic in the left side, that was operated through resection of the first rib. There was a torpid postoperative period. One CTV was requested in order to assess the patency of the left subclavian vein because, while in the postoperative care, the mobility of the patient's fingers got worse and was associated to paresis and pain in the patient's left hand and forearm. (A) Volume rendering. (B) Cinematic rendering. The patient showed postoperative changes in the left subclavian region after resection of the left transverse apophysis and partial resection of the patient's left first rib and lack of opacification (thrombosis) of the proximal third of the left subclavian vein along 3.5cm (arrows). The distal venous system of such limb was patent. An abundant collateral circulation was evident (arrowheads), above all in the anterior thoracic wall and, to a lesser extent, in the resection bed, draining into the venous brachiocephalic trunk and the left jugular vein.
. One cardio-CT scan was conducted as a follow-up to the ablation procedure. (A) Volume rendering. (B) Cinematic rendering. Four main pulmonary veins could be identified draining into the left atrium without an anomalous pulmonary vein drainage. There was stenosis of the left inferior pulmonary vein that had a diameter of 6×3mm (arrows). It was agreed to monitor the patient.")
Cardio CT scan in a 72-year-old female with a history of hypercholesterolemia and arterial hypertension. She had undergone left atrial flutter ablation and atrial fibrillation procedures a few months earlier. During the routine examination, the patient remained asymptomatic from the cardiovascular point of view (NYHA functional class I). One cardio-CT scan was conducted as a follow-up to the ablation procedure. (A) Volume rendering. (B) Cinematic rendering. Four main pulmonary veins could be identified draining into the left atrium without an anomalous pulmonary vein drainage. There was stenosis of the left inferior pulmonary vein that had a diameter of 6×3mm (arrows). It was agreed to monitor the patient.
As it occurs with the remaining post-processing techniques, the final outcome of images after cinematic rendering depends on the quality of the images originally obtained in the study. This is why we should pay special attention here adjusting all the necessary parameters in order to obtain images with the best possible diagnostic quality. Another limitation of this post-processing technique is that it requires very powerful computers since the reconstruction algorithms used are extremely complex. Similarly, each modification, displacement, or rotation conducted in the volume of data requires re-calculating the parameters, which is why the images are shown with lower resolution until such an estimate has been completed. Thus, the resulting final image can take up to 20s before being shown at full resolution.17 Another limitation of this technique is that it will not let us do endoscopic reconstructions to navigate through the lumen of an organ, trachea, or blood vessel. Finally, the cinematic rendering technique is built by one manufacturer only (Siemens Healthineers) and is used in a single platform (syngo.via Cinematic VRT). These days, its use is recommended for communication, teaching, and publishing purposes only, but not for diagnostic reading.
ConclusionThe CR is a new reconstruction method that provides hyper-realistic images by combining a more sophisticated morphological drawing and a higher perception of depth. These characteristics translate into high-quality images that simulate reality and probably increase diagnostic utility compared to conventional VR reconstructions, yet its clinical value is still to be determined.
Authors1. Manager of the integrity of the study: G.B., I.J.G., and A.A.B.
2. Study idea: G.B., I.J.G., and A.A.B.
3. Study design: G.B., I.J.G., V.M.V., and A.A.B.
4. Data mining: G.B., I.J.G., and M.C.I.
5. Data analysis and interpretation: G.B., I.J.G., M.C.I., V.M.V., and A.A.B.
6. Statistical analysis: N.A.
7. Reference: G.B. and I.J.G.
8. Writing: G.B. and A.A.B.
9. Critical review of the manuscript with intellectually relevant remarks: G.B., I.J.G., and A.A.B.
10. Approval of final version: G.B., I.J.G., M.C.I., V.M.V., and A.A.B.
Conflicts of interestThe authors declare no conflicts of interests associated with this article whatsoever.
Please cite this article as: Bastarrika G, González de la Huebra Rodríguez IJ, Calvo-Imirizaldu M, Suárez Vega VM, Alonso-Burgos A. Reconstrucción cinemática en imagen cardiovascular. Radiología. 2018;60:387–393.

