



Various COVID-19 vaccines are available across the world. However, short phases of clinical trials for emergency use and myriad rumors about and misinformation on vaccines spread through different media sources, induce confusion and trigger vaccine hesitancy behavior. Although clinical trials demonstrated promising results in the ability of vaccines to protect, social endeavor is required for vaccines to succeed. Mitigation of the pandemic is only possible through widespread acceptance of the vaccine. Thus, identifying the factors that impact vaccine intake is crucial. This study determined factors that affect intentions toward vaccination using a mixed-method approach, in which qualitative and quantitative analyses were conducted together. Analysis of variance (ANOVA) is used in the quantitative study, and content analysis is employed in the qualitative study. The final sample of this mixed-method study consists of 568 participants for the quantitative study and 237 for the qualitative study. They were selected using an online questionnaire. Findings suggest that social, psychological, attitudinal, perceptual, and informational factors play a crucial role in shaping people's intentions toward vaccines, ultimately influencing their decision to accept or reject vaccination. Results of both the qualitative and quantitative studies, in parallel with each other, indicated similar barriers against and drivers toward vaccine intake behavior, providing strong insights into the reasons behind vaccine acceptance and hesitancy. Based on the insights gained in this study, a set of recommendations were compiled for policymakers.
Social distance and lockdown regulations stipulate remaining at home, closing businesses or working from home, and abstaining from physical contact with people. These strategies have proved successful in mitigating the COVID-19 pandemic. However, such non-pharmaceutical interventions reduced output and economic growth worldwide (Wang et al., 2022), imposing financial, physical, and psychological costs on individuals (Sarfraz et al., 2022). Vaccination is seen as the most effective way to protect people, reduce the mortality count, and generally cope with the exigencies of the pandemic (Coccia, 2022).
Vaccines are innovative products (Bachmann & Frutos-Bencze, 2022; Mo et al., 2021). The notion of innovation is multifaceted and multidimensional, comprising various attributes (Hajighasemi et al., 2022). Although vaccines are now widespread, people can be hesitant about vaccine intake for various attitudinal reasons (Küçükali et al., 2022). However, the success of vaccines is shown not only in the efficacy rates that are clinically proven but also in individual acceptance rates (Bell et al., 2020; Shakeel et al., 2022). However, its accomplishment has been a social challenge centered on building human confidence (Schoch-Spana et al., 2021). Studies conducted on COVID-19 vaccination have mostly focused on beliefs in conspiracy theories and social media (Haakonsen & Furnham, 2022; Bacon & Taylor, 2022), country of origin Bayır et al. (2022), demographic factors (Hwang et al., 2022), overall perceptions of vaccines and vaccination (Bruno et al., 2022; Caserotti et al., 2021; Sönmezer et al., 2022), political affiliation and historical mistrust (Khubchandani et al., 2021), psychological concerns (Sarfraz et al., 2022), risk and severity perceptions (Yıldırım & Güler, 2022), racial differences and trust issues (Willis et al., 2021), and side effects (İkiışık et al., 2022). Furthermore, the extent to which COVID-19 vaccines have gained social acceptance in different societies remains relatively unclear. A greater proportion of the literature has focused on developed countries (Haakonsen & Furnham, 2022; Hwang et al., 2022; Khubchandani et al., 2021) rather than developing or underdeveloped countries (Salali & Uysal, 2020; Sallam et al., 2021; Sönmezer et al., 2022). Only a few studies have utilized qualitative approaches to gain further insights into understanding the factors affecting vaccination decisions (Bell et al., 2020; Khankeh et al., 2021).
Past studies have tended to evaluate psychological, attitudinal, perceptual, informational, and demographic factors affecting either vaccine-intake issues (Bell et al., 2020; Reiter et al., 2020; Shakeel et al., 2022) or vaccine-hesitancy issues (Caserotti et al., 2021; Hwang et al., 2022; Küçükali et al., 2022; Willis et al., 2021). The studies conducted on vaccination have mainly focused on developed countries and lack (1) integration of social factors, (2) qualitative approaches to gain further insights, and (3) a holistic approach that consists of a set of drivers and barriers that affect vaccination decision making. This study seeks to identify the effects of barriers to and drivers of COVID-19 vaccination using a mixed-method approach in Turkey, a developing country. On the one hand, quantitative results will determine the factors significantly affecting the overall tendencies toward vaccination. On the other hand, qualitative results will provide a detailed picture of how people perceive vaccines and their approach toward vaccination. Studies with mixed-method approaches are expected to strengthen the validity of the results and provide a deeper understanding of a phenomenon (Creswell, 2012; Creswell & Clark, 2018).
Previous studies have shown that vaccine hesitancy in Turkey is deep-seated. İkiışık et al. (2021) suggested that 45.3% of participants were hesitant to get a COVID-19 vaccine. Kucukkarapinar et al. (2021) revealed that vaccine hesitancy increased from 43.9% to 58.9% in the third period of their study. According to İkiışık et al. (2022), 29% of healthcare workers were undecided on vaccines, while 20.7% rejected vaccine intake. On March 11th, 2023, the share of people vaccinated against COVID-19 globally in a complete initial protocol and in partial vaccination only was 64.06% and 5.61%, respectively (COVID-19 data explorer, 2023).
On the other hand, as of March 11th, 2023, the percentage of the Turkish population vaccinated with the first dose was 69.31%, while the second, third, and fourth/fifth doses have reached 63.61%, 33.77%, and 15.93%, respectively (TURCOVID19, 2023). Vaccine hesitancy in Turkey is a significant threat to effective vaccination strategies. Vaccine acceptance is important in gaining herd immunity (Coccia, 2022). If vaccine hesitancy is prevalent among the public for identifiable reasons (İkiışık et al., 2022), other precautions to mitigate the pandemic would merely help public health practitioners buy some time (WHO, 2005) but would fail in the long run. Preparedness plans help governments keep pandemics under control to a certain extent, but the ultimate solution to end the pandemic permanently is to achieve herd immunity through vaccination (Coccia, 2022). Determining the degree of vaccine acceptance and the barriers and drivers that impact vaccine intake behavior will contribute to the vaccination literature and help public health practitioners develop strategies to mitigate the COVID-19 pandemic and promote vaccine intake behavior.
The next section includes a literature review of recent publications on this topic. The methodology section has elaborated the study's methodological design and conceptual model. Then, the results are presented, and the qualitative and quantitative designs are discussed. After summarizing the study's main findings in the conclusion, we advance a set of recommendations for policymakers.
Literature reviewAccording to CDC (2022), people who do not take a booster are considered “fully vaccinated,” but staying up to date with COVID-19 vaccines by taking boosters as they become available ensures the best protection. However, some studies argue that broad public support for vaccine intake is in question (Lazarus et al., 2023). Increasing vaccine hesitancy in society is the principal barrier to herd immunity (Kwok et al., 2020). Some studies estimated the proportion of the population vaccinated for herd immunity. The threshold level strictly depends on the basic reproduction number, R0- the number of other cases caused by one infected individual (Coccia, 2022). According to a study by Kwok et al. (2020), the proportion of the total population required for herd immunity was 85% for Bahrain, 84.3% for Slovenia, and 81.4% for Qatar. Coccia (2022) estimated that the proportion of the vaccinated population required to gain herd immunity ranges between 46.5% and 90% depending on circumstances.
Twum et al. (2021) revealed that attitude, social norms, perceived behavioral control, perceived susceptibility, and cues to action are essential factors motivating vaccine intake. Burke et al. (2021) revealed that confidence in vaccine approval, perceived effectiveness of the vaccine in protecting others, and conspiracy beliefs are the most critical drivers of vaccination intention. Ackah et al. (2022) determined that distrust of the pharmaceutical industry, the side effects that the vaccine may cause, and the misinformation in the media are barriers to vaccine intake. Jacoby et al. (2022) found that personal protection, protecting others, preserving public health, and general vaccine confidence are the main drivers of vaccine intake. On the other hand, other studies revealed concerns about the side effects of vaccines (İkiışık et al., 2022), concerns about COVID-19 vaccine trials (Jacoby et al., 2022), misinformation on vaccination (Bacon & Taylor, 2022), personal aversion to vaccination (Bruno et al., 2022; Caserotti et al., 2021), general distrust of vaccination (Willis et al., 2021), and mistrust of government (Khubchandani et al., 2021) are the main barriers to vaccine intake. Bolatov et al. (2021) identified concerns about the possible side effects of vaccines, the lack of sufficient evidence on their efficacy and quality, and the lack of belief and confidence that the immune system can cope with COVID-19 as the most critical barriers to vaccine acceptance. Gao et al. (2023) suggested that worry about the side effects of vaccines, uncertainty about vaccine safety, and underestimating the risk of exposure to COVID-19 are barriers to vaccine intake among medical students. Husted et al. (2023) revealed that the benefits of vaccines in facilitating a return to everyday life and protecting others are drivers of vaccine intake.
On the other hand, the authors found that concerns about the vaccine's potentially negative effects on fertility are a barrier to vaccine acceptance. Fisher et al. (2023) argue that recommendation by physicians is one of the most important drivers of vaccine intake. Ojewale and Mukumbang (2023) categorize the barriers to vaccine intake into biological concerns and sociopolitical factors.
To summarize, there is evidence that COVID-19 vaccine acceptance and hesitancy are nuanced and multifaceted, highlighting the need for ongoing research and targeted interventions to address the complex factors influencing vaccination behavior and attitudes.
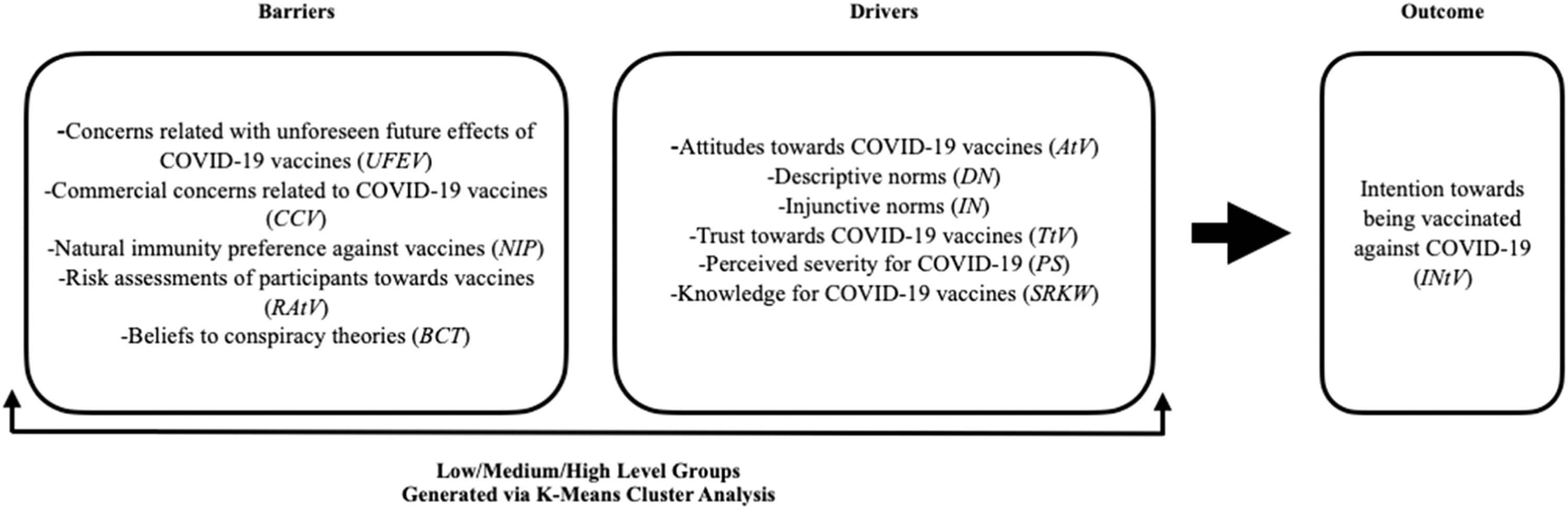
MethodThis study's conceptual model investigates the effects of a set of perceptions and attitudes toward vaccination on intentions to be vaccinated. It is based on the theory of reasoned action (TRA) (Fishbein & Ajzen, 1975) and the theory of planned behavior (TPB) (Ajzen, 1988, 1991). TPB is one of the most popular theories to explain human behaviors. According to TPB, intention is the antecedent of behavior, and intention toward behavior is determined by beliefs, attitudes, subjective norms, and perceived behavioral control (Ajzen, 1991). A holistic approach is required to fully understand people's behaviors toward vaccination, which include a set of barriers and drivers (Flanagan et al., 2020). Human behaviors are inherently complex phenomena to grasp. Given the uncertainties and complexities in vaccination behavior, it would seem to be a complicated matter to understand the factors that cause vaccine acceptance or hesitancy by testing structured models that have a purely quantitative focus. Well-established behavior theories, such as the theory of reasoned action (Fishbein & Ajzen, 1975) and the theory of planned behavior (Ajzen, 1988, 1991), explain up to 39% of behavioral intentions and actual behavior (Armitage & Conner, 2001). The reasons behind the unexplained variance remain largely unanswered in the quantitative studies that use structured models and behavior theories in their research designs. However, the factors that shape human behaviors develop mutually and simultaneously, and these factors are not always direct (Bagozzi, 1974, 2011). Therefore, a qualitative design is required to detect other factors not included in the research model and to compensate for the shortcomings of behavior theories and quantitative designs (Flanagan et al., 2020; Mosimann et al., 2017). These shortcomings reinforce the need for mixed-method and holistic approaches in vaccination studies to obtain a comprehensive overview and to identify factors that may have been overlooked. This study adopted a convergent (or parallel) mixed-method design to understand better how intentions toward vaccination are shaped. The purpose of this design is to attain different but complementary data on the same topic as the best means to explore the research problem. For this purpose, the researcher simultaneously collects and separately analyses quantitative and qualitative data types and compares or combines the results of two data sets to better understand the research problem (Creswell & Clark, 2018). The strength of this design is that quantitative results provide generalizability while qualitative findings give detailed information on the context (Creswell, 2012). The research question of the quantitative design is:
- i.
Do the clusters of respondents (low-medium-high), formed from a set of drivers of and barriers to vaccination, differ in their intentions to be vaccinated against COVID-19?
The research question of the qualitative design is:
- i.
How do respondents perceive COVID-19 vaccination?
This question on the qualitative design of the study is the only survey question directed to the participants following the quantitative part of the study. In the quantitative part, accurate scales based on the literature were used to measure the variables in the study. ANOVA tests were used to determine factors that impact intentions toward vaccine intake. On the other hand, in the qualitative part, the overall perceptions of the participants on COVID-19 vaccines were explored using an open-ended question, and data were analyzed using the content analysis method. This qualitative open-ended question further contextualized findings from the qualitative designs. A conceptual model is provided in Fig. 1.
Sampling and data collection
The population of this study consists of people living in Turkey. We used the convenient sampling method. Data were collected using an online survey from Google Forms between January 11 and January 25, 2021. Participants were assured that their answers would remain confidential and be used only for scientific purposes. A total of 645 completed surveys were collected in two weeks. Qualitative and quantitative data were collected simultaneously from the same sample.
Participants in the qualitative study consist of participants in the quantitative design who are willing to participate in the qualitative design. In the qualitative part of the study, the participants were asked one open-ended question on their overall perceptions of COVID-19 vaccines. Two hundred thirty-seven participants shared their overall view of COVID-19 vaccines. Later, their written statements in the questionnaire were content analyzed.
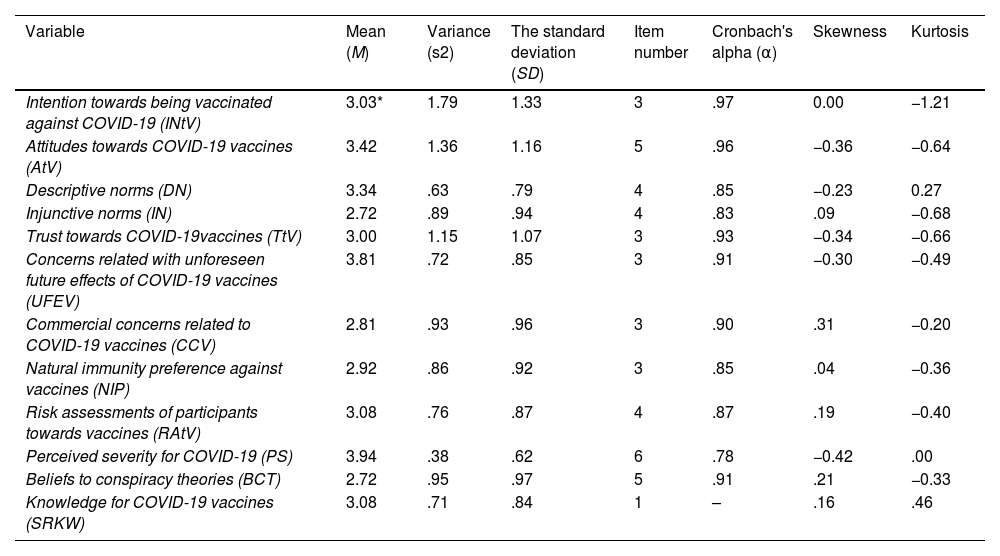
MeasuresThe questionnaire is divided into three sections. The first section of the questionnaire deals with the variables in the research. The items used to measure these variables were adapted from previous studies. A five-item scale was adapted from the study by Catalano et al. (2017) to measure attitudes to vaccines (AtV). This variable was designed to seek the participants’ overall attitude (favorable and unfavorable) to vaccines. A three-item scale was adapted from the study by Martin and Petrie (2017) to measure trust in vaccines (TtV). This variable sought to understand participants' hopes and beliefs about the efficacy of vaccines. To measure concerns related to the unforeseen future effects of the vaccines (UFEV), three items from the study by Martin and Petrie (2017) were employed. This variable aims to reveal participants' beliefs that vaccines may cause serious health problems in the future. Three items measuring the commercial concerns of vaccine companies (CCV) were adapted from the study by Martin and Petrie (2017). This variable aims to demonstrate participants' beliefs that the vaccines were developed for commercial rather than health purposes. Natural immunity preference against the coronavirus (NIP) was measured by three items adapted from Martin and Petrie (2017). This variable aims to reveal participants' desire for immunization by natural exposure to the coronavirus rather than by vaccines. Four items were adapted from Quinn et al. (2017) to gage participants’ perceptions of risk from vaccines (RAtV). This variable was designed to extract perceptions of the side effects that vaccines may cause. To measure the perceived severity of COVID-19 (PS), six items were adapted from Quinn et al. (2017). This variable aims to reveal how seriously participants perceive the COVID-19 outbreak. Five items measuring conspiracy theory (BCT) beliefs were adapted from Quinn et al. (2017). This variable provides insights into the extent to which participants believe in vaccine conspiracy theories. One item adapted from Quinn et al. (2017) measured knowledge of vaccines (SRKW). This variable aims to determine the general level of participants’ understanding of vaccines. Four items to measure descriptive norms (DN) were adapted from Robinson et al. (2008). This variable was designed to determine how participants’ significant others evaluate vaccination. The injunctive norm (IN) was measured by four items adapted from Shi et al. (2017). This variable refers to the social pressure that participants felt concerning vaccination. A three-item scale was adapted from the study by Caso et al. (2019) to measure intention toward being vaccinated. Descriptive statistics for the measures are given in Table 1.
Descriptive Statistics (n = 568).
| Variable | Mean (M) | Variance (s2) | The standard deviation (SD) | Item number | Cronbach's alpha (α) | Skewness | Kurtosis |
|---|---|---|---|---|---|---|---|
| Intention towards being vaccinated against COVID-19 (INtV) | 3.03* | 1.79 | 1.33 | 3 | .97 | 0.00 | −1.21 |
| Attitudes towards COVID-19 vaccines (AtV) | 3.42 | 1.36 | 1.16 | 5 | .96 | −0.36 | −0.64 |
| Descriptive norms (DN) | 3.34 | .63 | .79 | 4 | .85 | −0.23 | 0.27 |
| Injunctive norms (IN) | 2.72 | .89 | .94 | 4 | .83 | .09 | −0.68 |
| Trust towards COVID-19vaccines (TtV) | 3.00 | 1.15 | 1.07 | 3 | .93 | −0.34 | −0.66 |
| Concerns related with unforeseen future effects of COVID-19 vaccines (UFEV) | 3.81 | .72 | .85 | 3 | .91 | −0.30 | −0.49 |
| Commercial concerns related to COVID-19 vaccines (CCV) | 2.81 | .93 | .96 | 3 | .90 | .31 | −0.20 |
| Natural immunity preference against vaccines (NIP) | 2.92 | .86 | .92 | 3 | .85 | .04 | −0.36 |
| Risk assessments of participants towards vaccines (RAtV) | 3.08 | .76 | .87 | 4 | .87 | .19 | −0.40 |
| Perceived severity for COVID-19 (PS) | 3.94 | .38 | .62 | 6 | .78 | −0.42 | .00 |
| Beliefs to conspiracy theories (BCT) | 2.72 | .95 | .97 | 5 | .91 | .21 | −0.33 |
| Knowledge for COVID-19 vaccines (SRKW) | 3.08 | .71 | .84 | 1 | – | .16 | .46 |
The second section was related to demographic factors. Here, participants were asked if they had any chronic disease, whether they had been diagnosed with COVID-19 during the pandemic, and their brand preference for vaccines. In the last section of the questionnaire, participants were asked one open-ended question on their general perceptions of COVID-19 vaccines, allowing them to expound further on the subject.
Development of the codes and themesCoding is analyzing and interpreting the qualitative dataset (Miles et al., 2018). Based on the participants' statements, the first and second levels of coding were handled. First-level coding is the summary of data, whilst second-level coding categorizes the summaries into smaller groups. It resembles factor analysis or cluster analysis in qualitative research (Miles et al., 2018).
Coding of the qualitative data is done inductively rather than evaluating the qualitative data from the perspective of a predetermined theoretical framework. As a result of the second-level coding process, six themes and seventeen codes were identified. Of the six themes, half showed certain qualities related to vaccine hesitancy, whereas the rest were classified as vaccine acceptants.
Preliminary data screeningInitial screening demonstrated that all the data were in the dataset. Firstly, unengaged respondents (n = 17) were deleted from the dataset by calculating standard deviation values (lower than 0.5) for each participant's answers to five-point Likert items. Secondly, the dataset was checked to detect univariate (n = 14) and multivariate outliers (n = 46). Skewness and kurtosis values of the variables were checked for normal distribution. The dataset's skewness and kurtosis values are within the acceptable threshold values of −2 and +2 (George & Mallery, 2010). For multivariate outliers, the Mahalanobis distance of each case was calculated using regression analysis, and critical values of chi-square distribution (73.402 for df:40) were used (Tabachnick & Fidell, 2013). In this analysis, Mahalanobis distances of 46 cases were found to be higher than the expected critical value of chi-square distribution (df:40; p< .001), and these cases were removed from the dataset. In total, 77 cases were removed from the dataset. Further statistical analyses were conducted with 568 cases.
The scales' reliability was checked with Cronbach's alpha coefficient, which should be 0.70 or above (Nunnally, 1978). We determined that all scales used in this study were reliable.
ResultsParticipant characteristicsOf 568 participants, 48.6% (276) are female, and 51.4% (292) are male. Descriptive statistics on education level indicated that participants who graduated from high school and below amount to 12.9% (73), bachelor's degree holders are 49.9% (283), and postgraduates are 37.3% (212). The average age of participants is between 39 and 40. The biggest income group is earners between 5001 and 7000 TL (28.9%). Of the participants, 85.6% have no chronic diseases, and 88% have not been infected with the coronavirus. Furthermore, the most preferred vaccine brand is Biontech (47.6%).
Result and discussion on quantitative designWe performed a cluster analysis in this study. The variables of attitudes to COVID-19 vaccines, belief in conspiracy theories, commercial concerns related to COVID-19 vaccines, concerns pertaining to unforeseen future effects of COVID-19 vaccines, descriptive norms, injunctive norms, knowledge about COVID-19 vaccines, preferences for natural immunity as opposed to COVID-19 vaccines, perceived severity of COVID-19, participants’ risk assessment of COVID-19 vaccines, and trust in COVID-19 vaccines were divided into three groups of low, medium, and high. Later, the differences between the groups of the COVID-19 vaccine were tested using the ANOVA test.
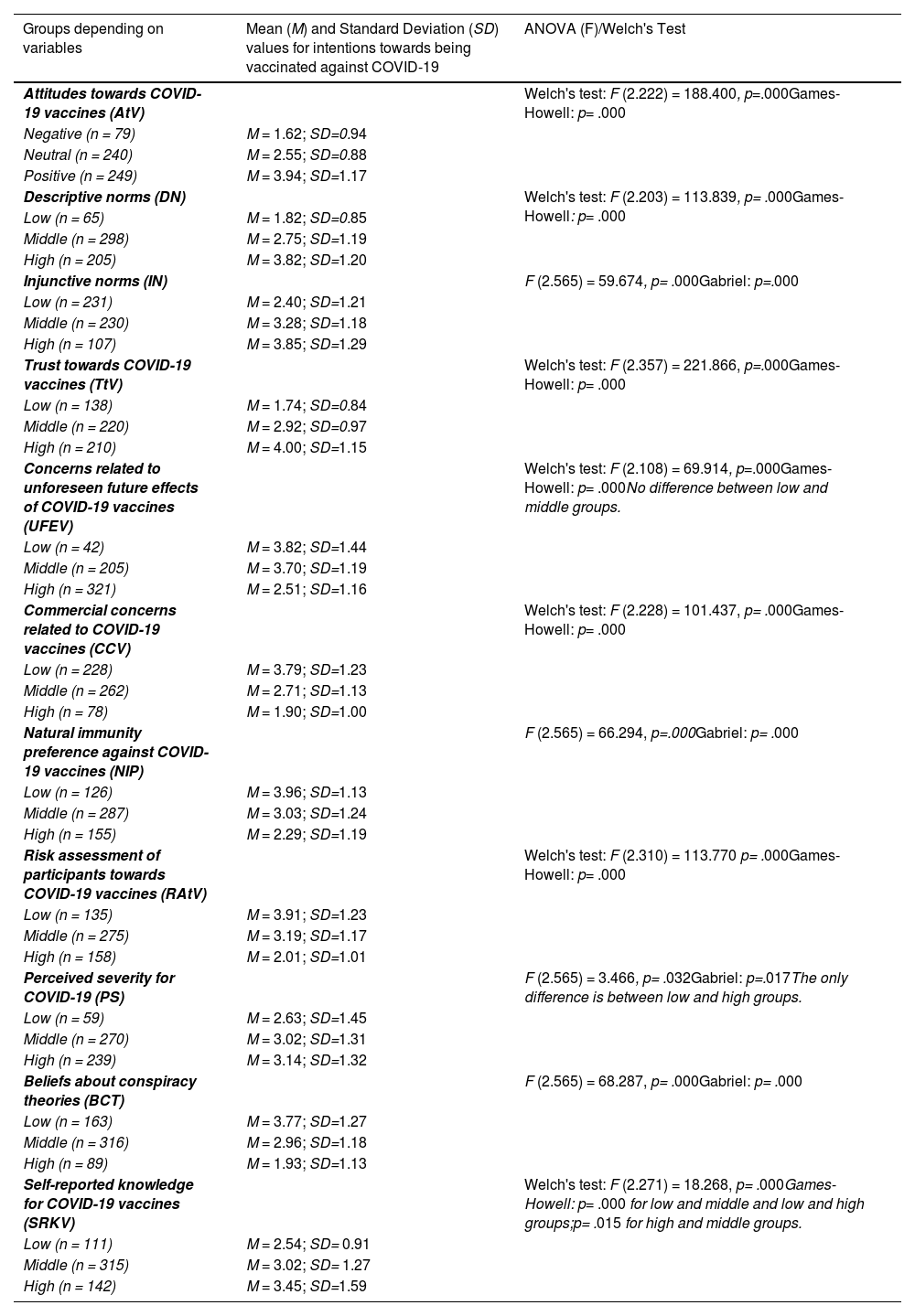
First, the independent variables, initially continuous by nature, were transformed into categorical data of low, medium, and high or negative, neutral, and positive by K-means cluster analysis. Second, the analysis of variance (ANOVA) test was conducted to determine whether these groups have statistically significant differences regarding their intentions for vaccine intake. ANOVA and post-hoc tests demonstrated statistically significant differences between groups, as shown in Table 2.
Differences in the Intentions Toward Vaccine Intake.
In the ANOVA test, homogeneity of variances of groups is expected, and it is checked using Levene's test. If Levene's test is significant (the p-value is less than 0.05), the homogeneity of variance assumption is violated. In that case, Welch's F statistic, a corrected form of the F ratio, can be used to check the differences between groups (Field, 2013). After finding the differences between groups, post-hoc multiple comparison tests can be used to see which specific group differs significantly from the others. In this stage, if the sample sizes of the groups are different, Gabriel's test, considered a robust test under this condition, can be used when the homogeneity of variances of the groups is not violated. However, when the homogeneity of variance assumption is violated, Games-Howell's test, considered a robust test under this condition, can be used (Field, 2013).
Participants’ intentions concerning vaccination were tested regarding AtV, DN, IN, TtV, UFEV, CCV, NIP, RAtV, PS, BCT, and SRKV variables. ANOVA results on AtV showed statistically significant differences between groups regarding their intentions concerning vaccination. Attitudes to vaccines determine intentions concerning vaccination. Results showed that the intention to be vaccinated increases as the attitude level changes from negative to positive. According to the theory of planned behavior (Ajzen, 1991), a person with a favorable attitude toward a behavior is likelier to perform that behavior. Thus, this finding is consistent with the assumptions of the theory of planned behavior. In addition, the results of many previous studies support this finding. For instance, Juraskova et al. (2012) and Graffigna et al. (2020) show that attitudes toward vaccines are positively associated with intentions concerning vaccine intake.
Results on DN showed statistically significant differences between groups in their intentions to be vaccinated. They showed that vaccination intention increases when participants believe others (e.g., family members, friends) consider vaccine intake the correct behavior. Similarly, results on IN showed statistically significant differences between groups in terms of their intentions to take the vaccine. Results indicated that intentions toward vaccination increase as perceived social pressure for vaccine intake increases. Findings on social norms demonstrate the importance of the social environment on vaccine intake decisions. According to the focus theory of normative conduct, two norms influence behaviors (Cialdini et al., 1990). These are the is (descriptive) and the ought (injunctive). Descriptive norms are what most people follow. These norms make people think, "If everyone is doing it, it must be sensible." Injunctive norms express what ought to be done.
According to this norm, people expect their behavior to be approved by the social environment (Cialdini et al., 1990). These results are in line with previous studies. Robinson et al. (2008) revealed that descriptive and injunctive norms positively affect the intention to donate blood. Thaker (2020) found that injunctive norms positively affect the choice to take the COVID-19 vaccine, but descriptive norms negatively affect the intention to take the COVID-19 vaccine. On the other hand, Mo et al. (2021) revealed that descriptive norms positively affected the intention to receive both the free and the self-paid COVID-19 vaccine.
Results on TtV showed statistically significant differences between groups in terms of their intentions to be vaccinated. Results showed that intentions toward vaccination increase as trust in vaccines increases. The study by Quinn et al. (2017), which reported a significant relationship between trust in the flu vaccine and intention toward vaccine intake, supported this finding. Verger et al. (2021) found that lower trust in COVID-19 vaccines and the Ministry of health negatively affects COVID-19 vaccine acceptance.
Results on UFEV demonstrate a statistically significant difference between low, high, and medium-high groups in their intentions toward vaccination. Results revealed that the intention to be vaccinated decreases as concerns related to unforeseen future effects of vaccines increase. Previous studies show that unexpected future effects of COVID-19 vaccines are one of the most critical barriers to the willingness to be vaccinated. For instance, İkiışık et al. (2022) explain that fear of the side effects of the COVID-19 vaccines is the most critical factor affecting indecision concerning and rejection of COVID-19 vaccination.
Results on CCV similarly demonstrated statistically significant differences between groups in terms of intentions toward vaccination. This indicates that vaccination intention decreases when participants view vaccine companies as profit oriented. Huynh (2020) suggested that commercial concerns about vaccines were higher during the COVID-19 pandemic.
Results on NIP showed statistically significant differences between groups in terms of intentions toward vaccination. Results indicated that the intention to be vaccinated decreases as participants prefer to gain immunity from exposure to the coronavirus. Paul et al. (2021) suggested that participants who prefer natural immunity have a highly negative attitude toward COVID-19 vaccines.
Results on RAtV showed statistically significant differences between groups regarding intentions toward vaccination. They indicated that the vaccination intention decreases if participants perceive vaccines as risky. This is consistent with previous research showing that risk perception impacts vaccination intention. Caserotti et al. (2021) suggested that as risk perception toward COVID-19 increases, choosing to receive COVID-19 vaccines increases. On the other hand, as PS increases, intentions toward vaccination also increase. Post-hoc results show a statistically significant difference between low-level and high-level groups regarding their preferences concerning vaccination. Reiter (2020) found that people reporting a high perceived severity of COVID-19 infection are more willing to take the vaccine due to the associated risks of the disease. Moreover, Ma and Ma (2021) suggested that the perceived severity of COVID-19 positively affected intentions toward COVID-19 and seasonal flu vaccinations.
BCT results showed statistically significant differences between groups regarding their intentions to be vaccinated. Results indicated that the intention to be vaccinated decreases when participants believe in conspiracy theories. This result is confirmed by existing studies on vaccine conspiracy theories (Bertin et al., 2020). Haakonsen and Furnham (2022) found that beliefs in conspiracy theories concerning the HPV vaccine negatively affected the intention to get the HPV vaccine. Similarly, Sallam et al. (2021) revealed that conspiracy beliefs concerning COVID-19 vaccination significantly affect vaccine rejection.
Contrary to this finding, vaccination intentions increase when people are knowledgeable about vaccines (SRKW). Results show statistically significant differences between groups with differing levels of knowledge on vaccines concerning their vaccination intentions. Many studies have revealed that insufficient vaccine knowledge results in vaccine hesitancy (Faasse & Newby, 2020). Moreover, Sönmezer et al. (2022) suggested that the level of knowledge about vaccines is associated with the willingness to be vaccinated.
Result and discussion on qualitative designSix themes were identified as a result of the qualitative data analysis. These themes were further elaborated by exploring some of the opinions and statements of the participants.
The Mistrustfuls: Participants clustered under the mistrustful theme, which accounts for 35% of participants, communicated that they did not regard COVID-19 vaccines as necessary. Furthermore, they did not trust them because of their concerns about the degree of protection; efficacy issues; hastiness in the phases of the development; information pollution; the origin of the vaccines; and unknown long-term effects and possible side effects.
Regarding the necessity of the coronavirus vaccination, participant 610 pointed out, “Because China, where coronavirus originates, overcame it without vaccination, I believe vaccines are unnecessary.” Similarly, participant 477 stated, “I regard the vaccination as unnecessary for a disease that can be overcome with a treatment at home.” Some participants are not totally against vaccines, yet they discriminate against them based on their origins. Participant 6 stresses that “China's is the least credible vaccine among all others.” Participant 206 states that she does not trust vaccines, except for European-based ones.
Concerning hastiness in the development phases of the vaccines, participant 312 says, “I do not trust vaccines because production is made, restricting immensely the time required for the phases of the clinical trials.” With reference to the unknown long-term effects and possible side effects, participant 252 states, “Because side effects are uncertain now, and even the side effects might be reported years later, I do not want to be vaccinated.” Drawing attention to information pollution and transparency issues, participant 14 contends, “We cannot accredit any information. Different news spreads every day. The vaccination process is not being managed transparently by the governments and vaccine companies.” Pointing to protection and efficacy issues, participant 555 claims, “It is not reliable now. Doctors say masks and hygiene (rules) continue even after the vaccination. Even if it is protective, its protection only lasts for 5–6 months, and (the coronavirus) has an eternal cycle of mutation. So, what benefit does it offer?” Participant 10 asserts, “I do not believe vaccines will work. Its harm will be much greater than its benefits.”
The Conspiracy Theorists: Participants identified as conspiracy theorists, who account for 6% of the total number of participants, think: the vaccines have malicious purposes; aim to change DNA; trigger various hereditary diseases; and let pharmaceutical companies get rich from people who are scared of the pandemic.
Concerning the possible effect of the vaccines on DNA, participant 556 believes that the sole purpose of the vaccines is to “change the genes,” and the purpose of the Chinese vaccine is to “cause the extinction of the Turks.” Participant 636 speculates, “I think vaccines include content effective on DNA by which mutant individuals are to be created. Issues such as pregnancy prevention, sexual preference, and so on might have been studied.” Emphasizing the hereditary diseases and financial interests, participant 395 surmises, “The vaccines were produced to cause vulnerability to the immune system, induce certain diseases (infertility, asthma, etc.), and also raise the morale of the people.” Participant 154 argues, “Vaccines are the continuation of the project (?), maybe there is no chip, but they trigger hereditary diseases and infertility.” Participant 302 regards vaccination as “a system designed to let pharmaceutical companies earn money.”
The Undecideds: Participants called the undecideds, who account for 17% of participants, have not decided whether or not to be vaccinated. They are undecided whether vaccines or COVID-19 disease carry the greater risk. The undecided participants are neutral on both vaccines and vaccination because they do not command full knowledge on the benefits of the vaccines.
Participant 44 mentions that he is unsure which vaccine type he should choose, but he is more prone to opt for inactive vaccines than mRNA vaccines. In addition, he claims, “I stand distant from vaccines of countries, such as China and Russia, who publish reports that are beyond transparency and being scientific.” Participant 508 states, “When the proper explanation about vaccination is given, people would trust and get injected. However, now, there are a few brands, and we do not know which one to trust (and choose).” Participant 624 points to the importance of information on vaccines and states, “According to my observations, because the extent of the side effects and the extent to which the vaccines are effective is unknown, people are hesitant about whether to be vaccinated or not.” Participant 614 summarizes the overall thoughts of the undecideds in remarking, “I am undecided about my thoughts on vaccines. While one part of me accepts vaccines, the other rejects them.”
The Hopefuls: Participants whose thoughts are classified under hopefuls, who account for 18% of participants, expect vaccines to work and end the pandemic very soon. Many participants emphasized the benefits of vaccines and expressed their trust in science and technology. Therefore, these participants believe in the protection that COVID-19 vaccines provide. Participant 592 is convinced that “It is possible to expedite the vaccine development process through developing science and technology.” In general, participants are more prone to believe in the efficacy of the vaccines. Participant 60 contends, “I believe in the phases of the vaccine development and that it will impede the pandemic.” Participant 538 claims, “I think the vaccines are protective.”
Furthermore, participant 148 argues, “I hope to get back to normal life even if (vaccines) would provide a small amount of protection.” Participant 384 asserts, “I believe the COVID-19 pandemic will have been controlled through vaccines by spring.” Others are more cautious about the timescale. Participant 543 stresses, “I am hopeful for the vaccines. Thanks to vaccines, I hope we will begin to normalize in a few years.” Some participants imply that normalization is only possible when a sufficient number of people are vaccinated. Participant 608 believes, “We will be safely back to our old days only if a sufficient number of people are vaccinated with sufficient doses.”
The Ones Seeing Vaccines As A Necessity: Participants seeing vaccines as a necessity, who account for 18% of participants, emphasize, ceteris paribus, that the public should be vaccinated to overcome the pandemic and get back to everyday life. Even though some participants infer that vaccines might cause unknown side effects because of the hastened phases of clinical trials, they perceive the coronavirus as a greater danger to health, economy, and social life. Participant 13 argues that, leaving all kinds of conspiracy theories aside, “it is a must that the public, especially certain people at risk, should be vaccinated for health and even survival.” Participant 518 offers a loss/gain analysis of vaccination, “I am sure there are going to be side effects. However, compared to what happens if I infect my mom at the age of 70 after coming back home from work by using public transportation (every day), it sounds much more reasonable to choose vaccines.” Participant 481 affirms, “It is necessary for the sustainability of the economic and social life that pandemic must end. For that, vaccination matters a lot.” Participant 596 regards COVID-19 vaccines as “the only one force to stop the pandemic.” Regarding the unknown side effects of the vaccines and severity of the coronavirus, participant 601 avers, “While facing the deadly coronavirus each day, I regard the injection of the inactive coronavirus as less dangerous.” Participant 196 offers a concluding thought that reflects the overall views of the participants who regard vaccines as a necessity, “Because full results of the 3rd phase of the clinical trials will take years, vaccines should be launched without making each control. However, this is a cost that people should bear, and the risks are to be taken to lower the harm of the COVID-19 pandemic and put things back in order.”
Domestic Vaccine Supporters: Participants whose opinions were evaluated under the theme of domestic vaccine supporters, who account for only 6% of participants, represent an apparent inclination toward domestic attempts at COVID-19 vaccines. Domestic vaccine supporters tend to discriminate against vaccines because of their foreign origin, showing certain ethnocentric tendencies, medical products notwithstanding. The main reason for this inclination toward domestic vaccines revolves around trust issues. Participants who do not trust foreign alternatives are prepared to take the risk of not being vaccinated and, instead, wait for the launch of the domestic vaccines. Participant 311 explains, “I will wait until my country's vaccine is produced.” Participant 54 asserts, “I trust only in Turkey-made vaccines.” Participant 540 argues, “I do not trust foreign-based vaccines. Although I trust domestic vaccines, I am worried about what kind of side effects and problems in the long term would emerge.”
As with the ANOVA results, certain factors that stand as drivers toward and barriers against vaccination have been identified by employing a qualitative study. Trust issues represent the essential element in vaccine hesitancy. Participants abstain from being vaccinated because of concerns over the degree of protection, efficacy issues related to vaccines, hastiness in the development phases, information pollution, and unknown long-term effects. These reasons constitute trust issues that militate against vaccine acceptance. When the concerns that trigger a lack of trust in vaccines predominate, participants are more inclined not to be vaccinated.
Some participants mentioned various conspiracy theories about COVID-19 vaccines. They explicitly stated that some clandestine organizations have malicious intentions with vaccines. Commercial concerns, controlling people, genetic modification, reducing the world population, and triggering genetic diseases were the ulterior motives behind the COVID-19 pandemic and the vaccines. Similarly, over one-quarter of participants stated they were undecided about vaccination. The most crucial factor for undecided people was the lack of information about and perceived risks from vaccines. It was clear that vaccine hesitancy was prevalent among participants clustered under “the mistrustful,” “the conspiracy theorists,” and “the undecideds” categories.
Participants who favor vaccination believe in vaccines' protection and the merits of contemporary science and technology. They are aware of discussions on the level of protection, the safety of vaccines, and the possible future side effects. Despite this, they are inclined to believe in the authorities’ statements and scientific results. On the other hand, some participants are more skeptical and have a higher risk awareness associated with vaccine intake. Nonetheless, after processing information about vaccines' possible risks and benefits, they conclude that vaccination is necessary for everyone, and the potential risks can be borne. Skeptics who nevertheless favor vaccination regard coronavirus as a more significant threat. They are eager to use vaccines despite the risks they perceive.
Interestingly, a particular group of participants showed interest only in Turkey-based vaccines, possibly stemming from ethnocentric tendencies and trust issues concerning things foreign. One-quarter of participants in the quantitative findings chose the Turkey-based vaccine as the second most favored vaccine brand. Hence, the concept of ethnocentrism is an influential factor in the degree of vaccine acceptance in Turkey. In conclusion, it was evident that participants clustered under “the hopefuls,” “the ones seeing vaccines as a necessity,” and “domestic vaccine supporters” categories were in favor of vaccination because they had positive attitudes toward and trust in vaccines.
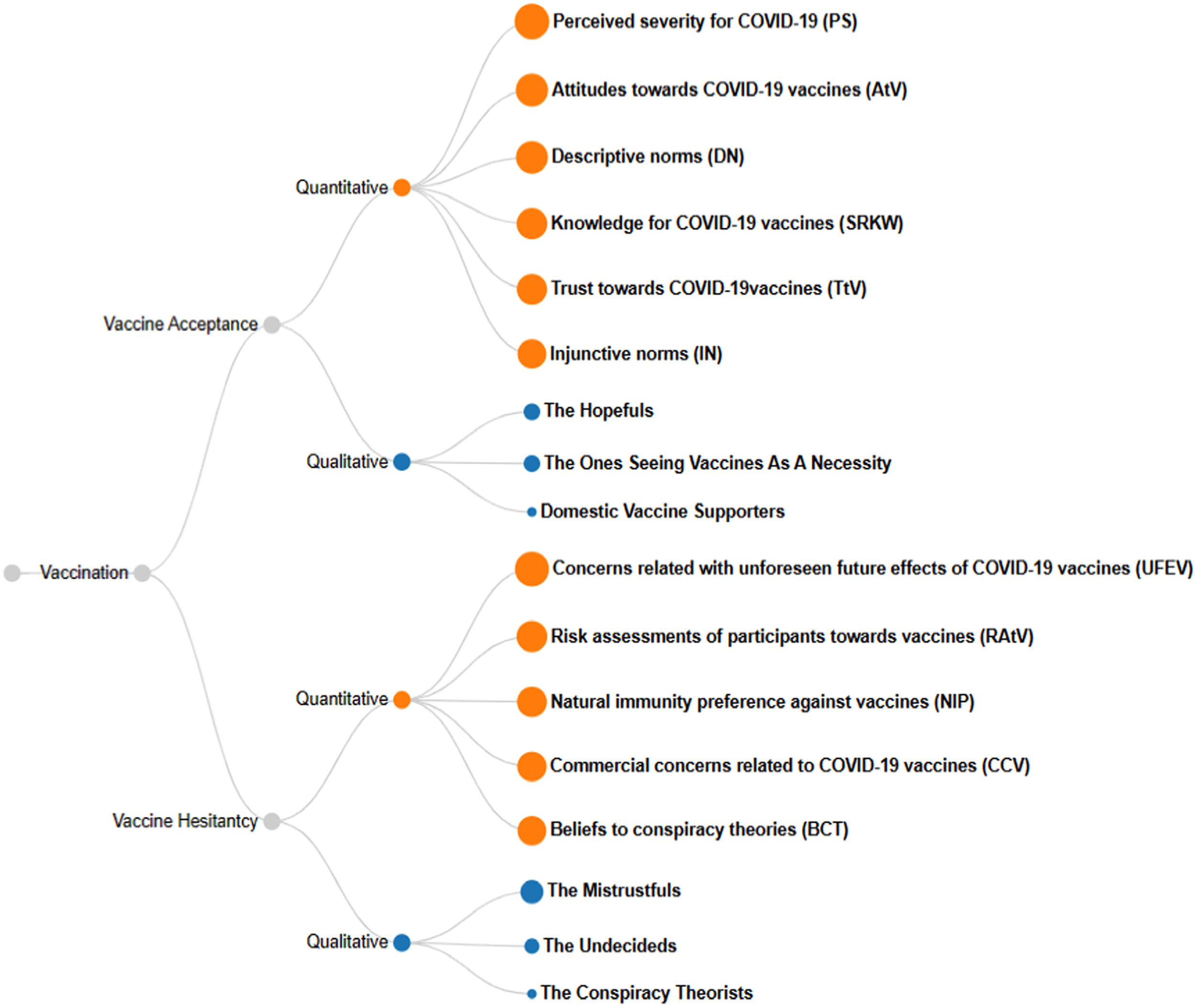
ConclusionsParticipants would be concerned about COVID-19 vaccines even if they expressed trust in vaccines that possessed certain qualities. This conclusion is generalizable to almost every participant in this study. Therefore, vaccine hesitancy appears to be a significant problem in Turkey. In the qualitative study, vaccine hesitancy was widespread among the mistrustful, the conspiracy theorists, and the undecideds, who account for 58% in total. In contrast, the hopefuls, the ones seeing vaccines as a necessity, and domestic vaccine supporters, who account for 42% in total, were inclined to vaccine acceptance. Similarly, the quantitative research results determined that 74% of the participants are vaccine hesitant, while 26% are prone to vaccine acceptance. The percentage of vaccine hesitancy derived from the quantitative study is higher than the data of TURCOVID-19 (2023), while qualitative results seem to be more in line with the statistics of TURCOVID-19 (2023). One reason might be the gap between intentions and behaviors, as suggested in the theory of reasoned action (Fishbein & Ajzen, 1975) and the theory of planned behavior (Ajzen, 1988, 1991). Another reason why intentions were not transformed into actual actions in vaccination behavior may be explained by the statements of Participant 196: “Because full results of the 3rd phase of the clinical trials will take years, vaccines should be launched without making each control. However, this is a cost that people should bear, and the risks should be taken to lower the harm of the COVID-19 pandemic and put things back in order.” Although people are afraid of the unknown future effects of the vaccines, they regard it as a cost to be borne when faced with the risk, severity, and societal outcomes of COVID-19. Individuals who are intrinsically vaccine hesitant seem to get vaccinated to share the cost of “putting things back in order.” This finding strengthens the idea that, since the exploratory studies into vaccination include a high level of uncertainty, information asymmetry, and information pollution, mixed-method studies can help researchers to gain further insights into the factors that shape vaccination behavior and to interpret the results of quantitative research in a more meaningful way. The summary of the drivers of and barriers to vaccine intake behavior identified in the quantitative and qualitative studies is illustrated in Fig. 2. The dots in the figure vary across the averaged means for quantitative variables and percentages for the qualitative variables. These have been transformed into a five-point scale to form a unified measurement and illustration.

It is generally understood that herd immunity is the only way to eliminate the COVID-19 pandemic permanently. COVID-19 vaccines play an essential role in the formation of herd immunity. The main purpose of this study is to investigate the factors affecting intentions toward COVID-19 vaccine intake in Turkey. According to the results of our study, knowledge, social norms, perceived severity, attitudes, and trust positively affect the intention to take vaccines. At the same time, possible unknown future effects, the commercial interests of pharmaceutical companies, the perceived risk from vaccines, and beliefs about conspiracy theories are the negative factors that impede vaccine intake behavior.
Moreover, our qualitative study supports these findings and highlights the importance of transferring accurate vaccine information to the public. It was ascertained that vaccine hesitancy is primarily rooted in information pollution, trust issues, and misbeliefs about vaccines. These results can contribute significantly to planning and developing decisions to increase acceptance of COVID-19 vaccines.
Evans and French (2021) identify a pressing need to create vaccine demand. Vaccines are the product of an intellectual and technological endeavor, while their widespread acceptance is a social endeavor influenced by human factors (Schoch-Spana et al., 2021). Creating a solid marketing plan requires having reliable and valid consumer insights. Appraising the findings from past studies related to vaccine hesitancy might be helpful to obtain these insights. After determining the factors related to vaccine hesitancy, the antithesis of these factors can be created and used to form effective marketing strategies. Vaccines are products developed for community health and social benefit. If they are promoted through practical marketing efforts, undecided, hesitant, and resistant people can be encouraged to adopt them much more quickly.
Limitations and directions for future studiesThe data were collected between January 11 and January 25, 2021, which limits the possibility of providing insights into the barriers to and drivers of vaccination in the early and late pandemic stages. Although the participants in the study were selected using an online questionnaire distributed via various social media platforms, systematic approaches to probability sampling have yet to be employed in the sample selection. Therefore, this study's findings are limited to the sample and cannot be generalized beyond the context of Turkey. Future studies can utilize the benefits of longitudinal data to determine the direction of the changes in vaccination behavior. The purpose of this study was to explore and describe a set of barriers to and drivers of vaccination behavior. Therefore, basic ANOVA tests for quantitative data and content analysis for the qualitative data were deemed sufficient to serve this study's purposes. However, future studies can focus on experimental and predictive designs to identify the interrelationships between these variables that significantly influence vaccination behavior in a cause-and-effect framework and to contribute to the body of knowledge on how vaccination behavior is formed.
Recommendations to policy makersIn addition to the supply problems of vaccines, governments face many societal problems in their endeavors to overcome the worsening effects of the pandemic. If these problems are defined clearly, possible solutions can be created.
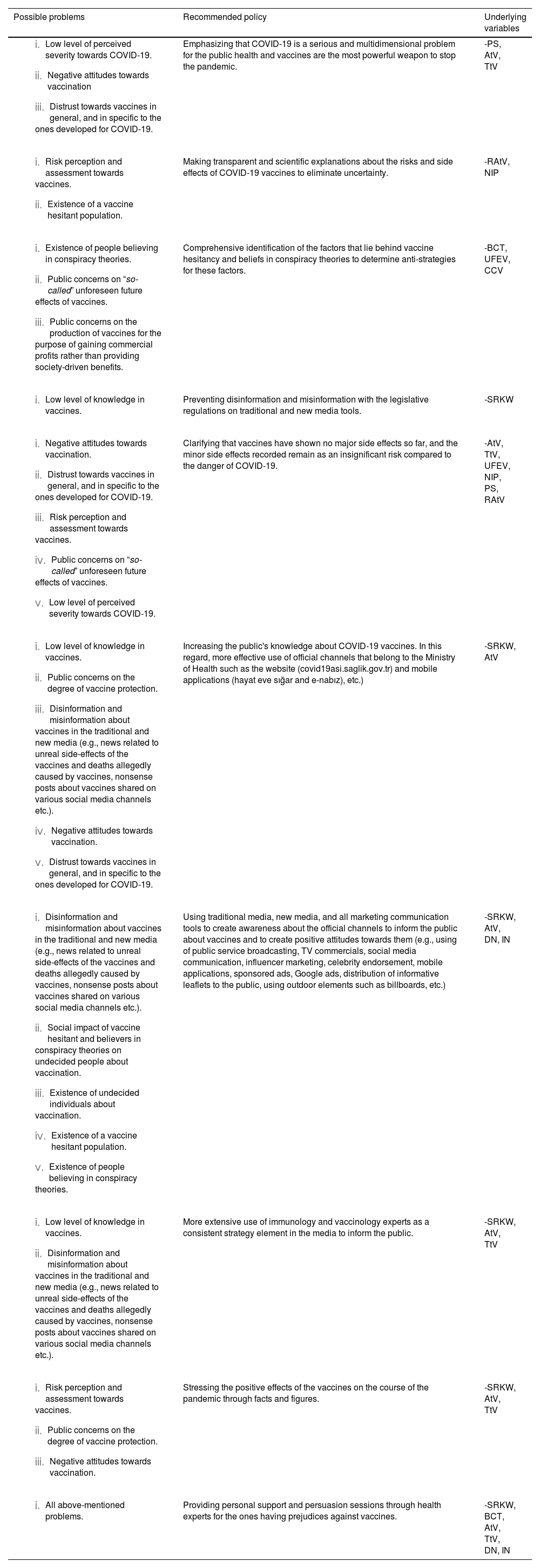
While the potential problems outlined in Table 3 are apparent and have culturally solid bases in the context of Turkey, some of these problems can be seen as issues that many other countries face. These problems can be closely associated with people's beliefs, attitudes, risk perceptions, and evaluations toward COVID-19 and the vaccines developed to eradicate its effects. A consistent, determined, and effective communication strategy can overcome these problems. Therefore, the first recommendation of the present study is to establish a strong communication strategy to promote the policies formulated from the problems identified and the findings of the current study, as shown in Table 3.
Recommendations to Policymakers.