
The aim was to analyse the stoma reversal rate after surgery for complicated acute diverticulitis (CAD), and more specifically the end-stoma-reversal, as well as the delay, feasibility, complications and risk factors for stoma maintenance.
MethodsA multicentre retrospective study of patients who had undergone urgent surgery for CAD with stoma formation in 10 hospitals during a period of 6 years. The frequency of reversal over time and the factors affecting the decision for reversal were analysed.
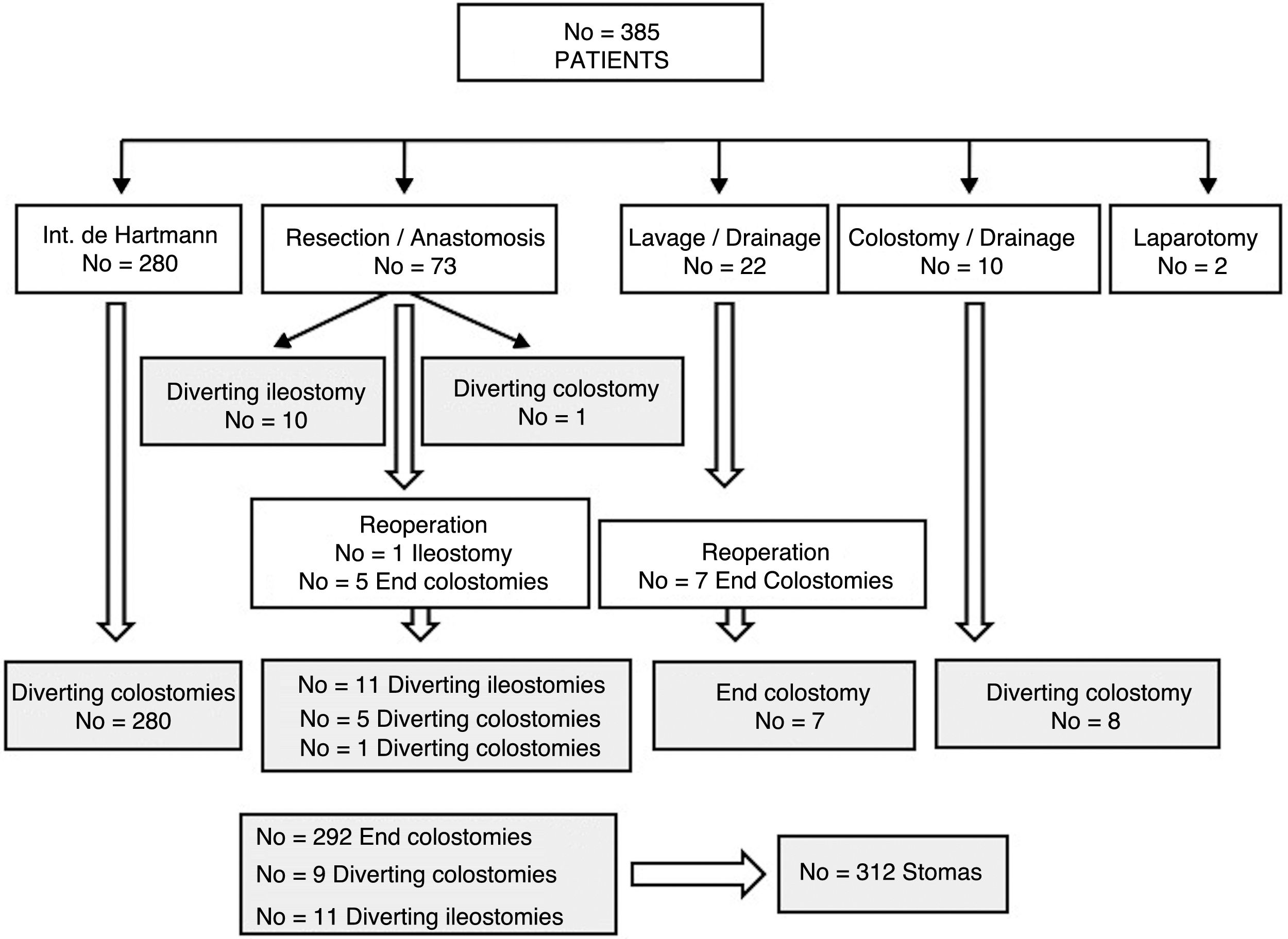
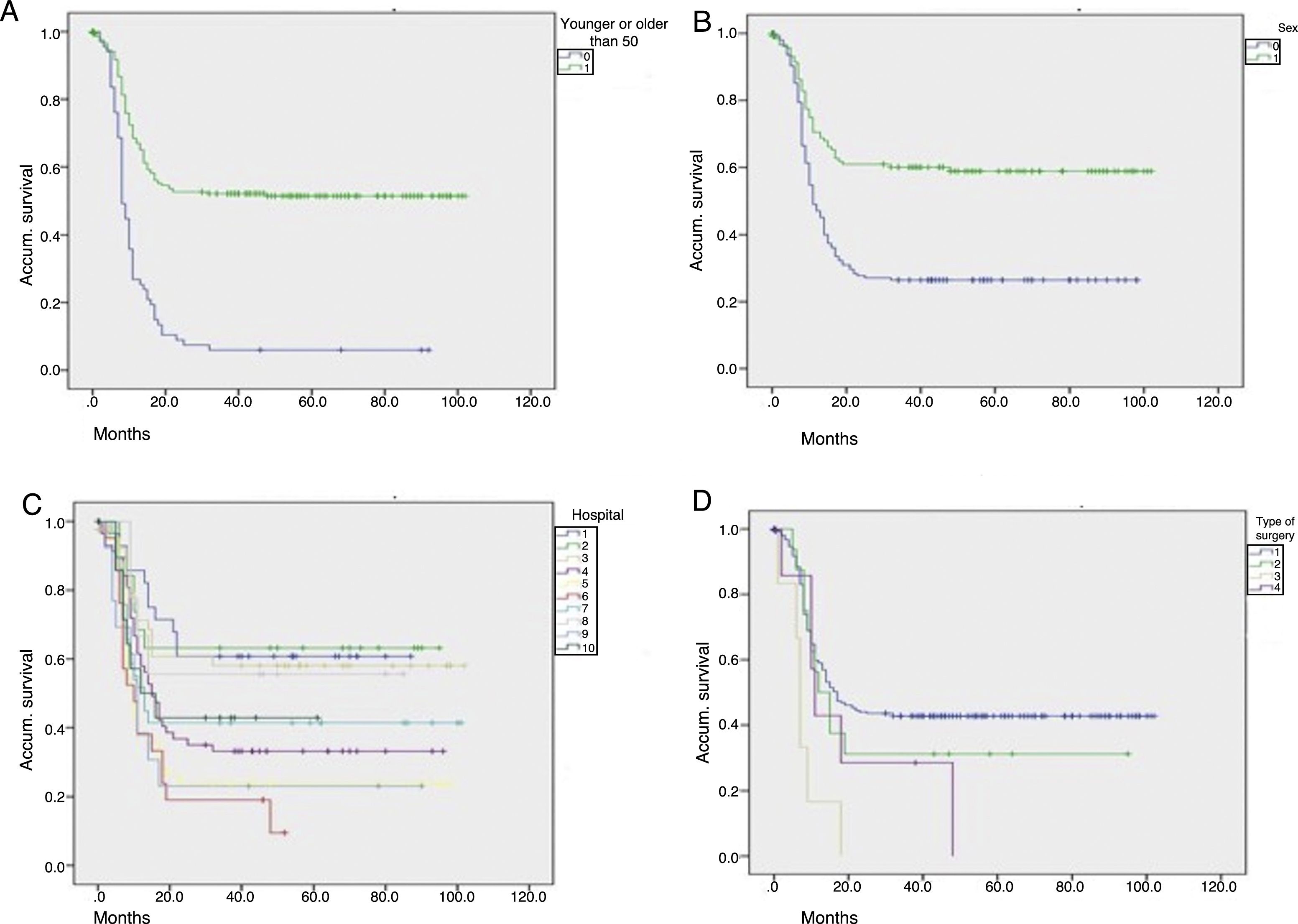
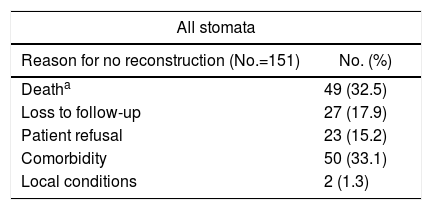
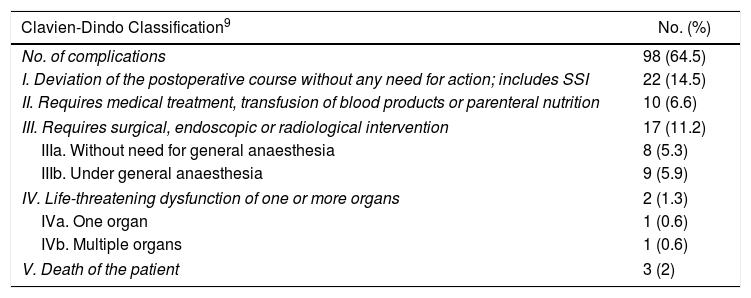
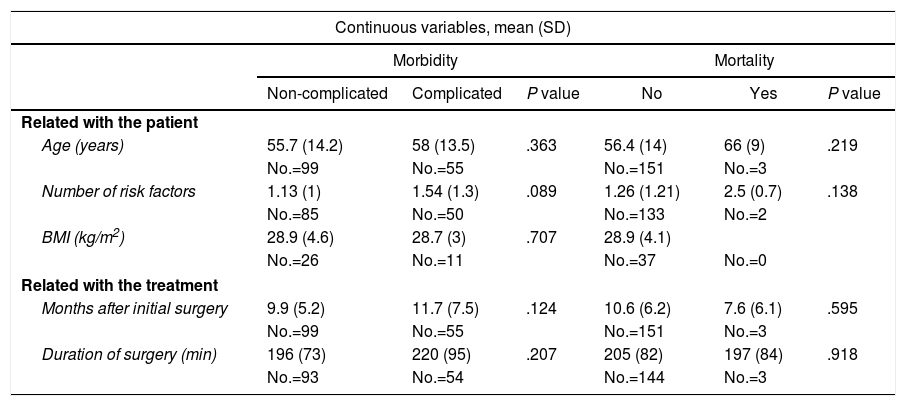
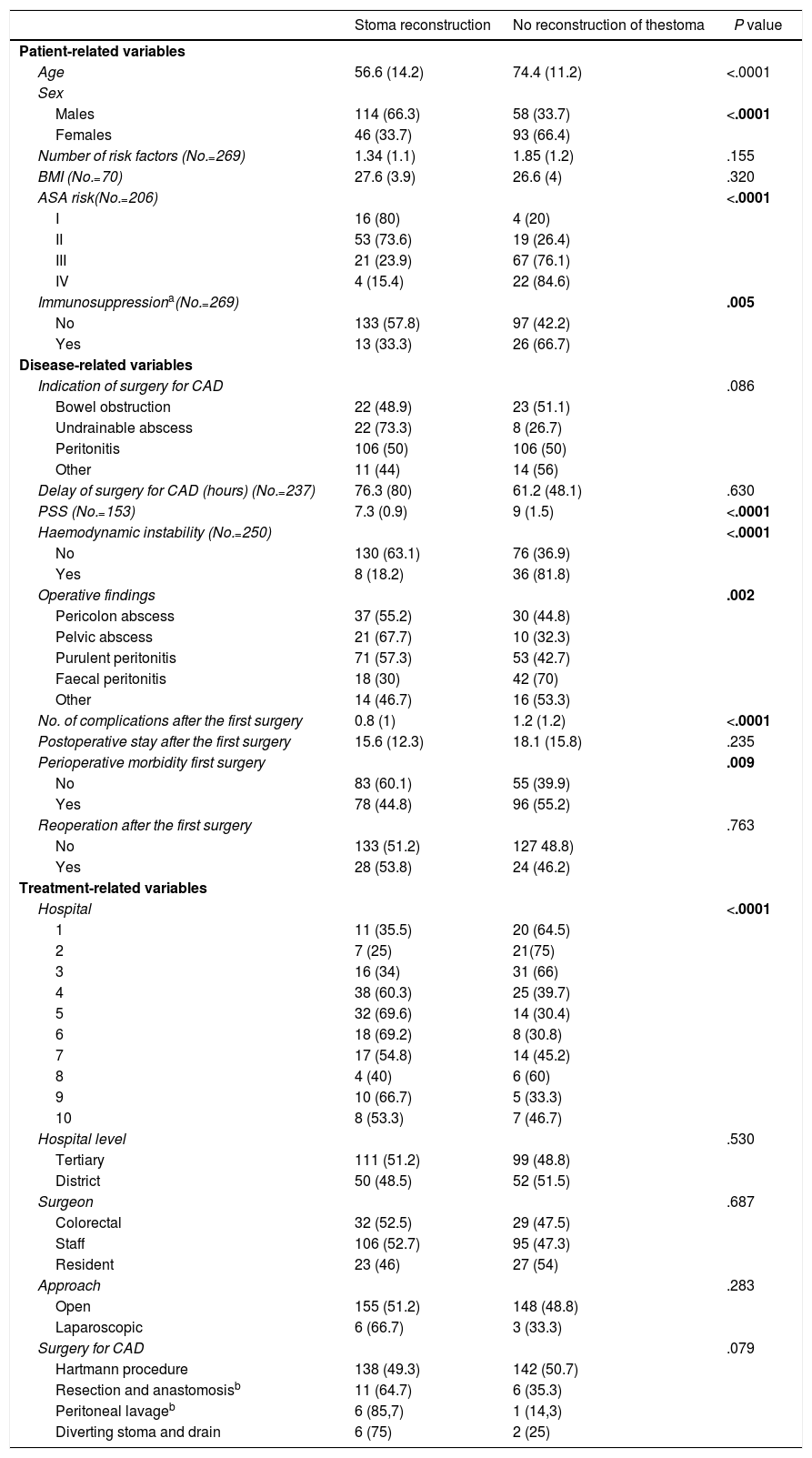
ResultsOut of 385 patients operated for CAD, 312 underwent stoma creation: 292 end colostomies and 20 diverting stomas. During follow-up, stoma reversal surgery was performed in 161 patients (51.6%) after a median of 9 months. The main causes for not performing stoma reversal were comorbidities and the death of the patient. Advanced age was an adverse factor in the multivariate analysis, and the actuarial rate of reversal was higher in men and in patients with no previous Hartmann's operation. Stoma reversal surgery was completed in all but 1 patient, and a loop ileostomy was associated in 4. Morbidity and mortality rates were 35.7% and 1.9%, respectively. A total of 8.4% of patients underwent re-operation, and 6% experienced an anastomotic leak. Twelve patients remained with a stoma after the attempted reconstruction surgery.
ConclusionsSurgery for CAD is frequently associated with an end stoma, which will ultimately not be reversed in almost 50% of patients. Moreover, reversal surgery is frequently delayed and is associated with significant morbidity and mortality.
El objetivo del estudio es analizar la tasa de reconstrucción del estoma tras cirugía por diverticulitis aguda complicada (DAC), su demora, factibilidad, complicaciones y factores de riesgo de mantenerlo.
MétodosEstudio retrospectivo multicéntrico de pacientes intervenidos mediante cirugía urgente por DAC con realización de un estoma en 10 hospitales durante 6 años. Se analiza la frecuencia de reconstrucción del estoma, fundamentalmente de los terminales, y el tiempo en que se produce, así como los factores relacionados con ella.
ResultadosDe 385 pacientes intervenidos por DAC, a 312 (81%) se les realizó un estoma: 292 fueron colostomías terminales y 20 estomas derivativos. Durante el seguimiento, en 161 (51,6%), se intentó el cierre a una mediana de 9 meses. Las causas más frecuentes de no efectuarlo fueron la comorbilidad y el fallecimiento del paciente. La edad más avanzada se mostró factor adverso en el análisis multivariante y la tasa actuarial de reconstrucción fue mayor en hombres y en quienes no se realizó un Hartmann. La cirugía pudo completarse en todos menos en un paciente y en 4 se asoció un estoma derivativo. La morbimortalidad fue del 35,7 y 1,9%, respectivamente. Hubo un 8,4% de reintervenciones y un 6% de fallos de sutura, quedando 12 pacientes (7,9%) con un estoma tras el intento de reconstrucción.
ConclusionesLa cirugía de la DAC se asocia muy frecuentemente a la construcción de un estoma terminal, que en casi un 50% no se reconstruirá. Además, la intervención de reconstrucción tiene una demora notable y está asociada a una morbimortalidad nada despreciable.