






Anterior resection with total mesorectal excision is the standard method of rectal cancer resection. However, this procedure remains technically difficult in mid and low rectal cancer. A robotic transanal proctectomy with total mesorectal excision and laparoscopic assistance is reported in a 57 year old male with BMI 32kg/m2 and rectal adenocarcinoma T2N1M0 at 5cm from the dentate line.
Operating time was 420min. Postoperative hospital stay was 6 days and no complications were observed. Pathological report showed a 33cm specimen with ypT2N0 adenocarcinoma at 2cm from the distal margin, complete TME and non affected circumferential resection margin.
Robotic technology might reduce some technical difficulties associated with TEM/TEO or SILS platforms in transanal total mesorectal excision. Further clinical trials will be necessary to assess this technique.
La resección anterior con escisión total mesorrectal es el tratamiento estándar para el cáncer de recto. Este tratamiento sigue siendo técnicamente dificultoso en los tumores localizados en el recto medio e inferior.
Presentamos un caso de escisión total mesorrectal robótica transanal con asistencia robó tica en un varón de 57 años e IMC 32kg/m2 con un adenocarcinoma T2N1M0 a 5cm de línea pectínea tras tratamiento neoadyuvante. El tiempo quirúrgico fue de 420min. La estancia postoperatoria fue de 6 días, sin objetivarse complicaciones. El estudio anatomopatológico demostró una pieza de 33cm, una tumoración ypT2N0 con margen distal de 2cm, margen circunferencial libre y buena calidad del mesorrecto.
La tecnología robótica puede disminuir la dificultad inherente a las plataformas TEO/TEM o SILS para la realización de este tipo de procedimientos. La realización de ensayos clínicos es necesaria para la completa evaluación de esta técnica.
In recent years, colorectal surgery has undergone different technical changes that have improved the postoperative wellbeing of patients. Some of these changes have been brought about by the application of new technologies that have enabled us to perform classic colorectal procedures using minimally invasive approaches. In the case of rectal cancer, the curative treatment is still currently based on total mesorectal excision, with or without associated chemoradiotherapy.1,2 This procedure has classically been performed by an open anterior abdominal approach. In the last few years, multi-center studies have compared proctectomy in open surgery vs laparoscopic surgery. The preliminary results are similar in oncologic results, with a slight postoperative advantage in the laparoscopic groups.3–5 At the same time, some centers with experience in laparoscopic rectal surgery with robotic assistance have published comparative studies in rectal cancer between open, classic laparoscopic and robotic-assisted laparoscopic approaches that show slight advantages in this latter group.6
In the same context of performing proctectomy in the least aggressive manner possible for the patient, while at the same time maintaining the oncologic safety of the procedure, short series have been published recently using natural orifice transluminal endoscopic surgery (NOTES) with laparoscopic assistance, which have shown promising results.7–11 The feasibility of this technique done with transanal robotic assistance has been demonstrated by Atallah et al. in the treatment of a patient with inflammatory bowel disease, with good postoperative results.12
Now there are several hospital centers throughout the world that are developing the technique published by the Atallah group, and our center is one of them. In this context, we have developed a research program some years ago that is currently in the pilot-study phase, which was approved by the Ethics Committee of the Community of Cantabria. We present a case in which we show the feasibility of robotic transanal total mesorectal excision with laparoscopic assistance in the treatment of rectal cancer.
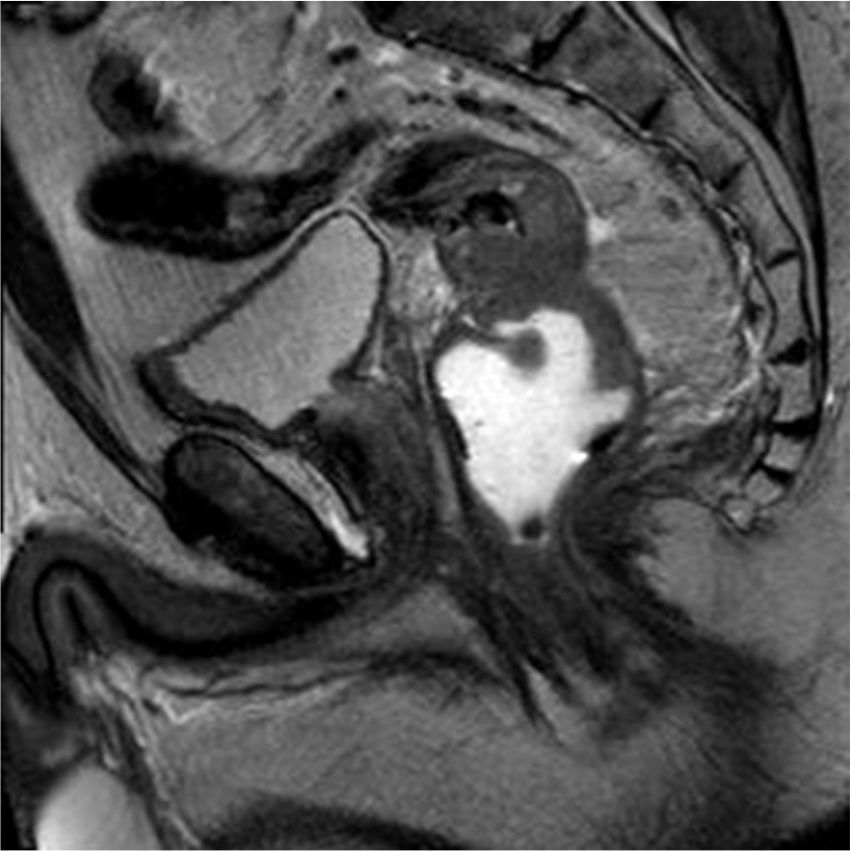
Materials and MethodsPreoperative StudyThe patient is a 57-year-old male who was obese with a BMI of 32kg/m2, with no other prior history of interest, with an adenocarcinoma on the posterior side of the mid-rectum, 5cm from the dentate line. Preoperative studies included colonoscopy with biopsy, endoanal ultrasound, thoracoabdominal-pelvic computed tomography (CT) and pelvic MRI. The lesion was staged as locally advanced rectal cancer (T2N1) with no signs of distant extension. The pelvis measured by CT was 103mm in retropubic promontory diameter and 86mm subsacrum-retropubic, with a maximum lateral diameter of 107mm. The tumor mass was predominantly posterior and had a maximum diameter of 43mm and a maximum longitude of 67mm (Figs. 1 and 2).


These measurements indicated a patient with a complex pelvis for surgical treatment.13 CEA was normal. With these studies, neoadjuvant treatment was indicated with long-course radiotherapy of 50.4Gy associated with capecitabine. After neoadjuvant treatment, a new CT showed absence of distant disease and diffusion MRI reported T2N0, with good response to treatment. Preoperative ultrasound demonstrated an important reduction in the volume of the lesion. After these studies, the patient agreed to be included in the pilot study to validate the transanal robotic excision technique with laparoscopic assistance.
Surgical TechniqueThe technique was performed in accordance with the protocol established for the pilot study.
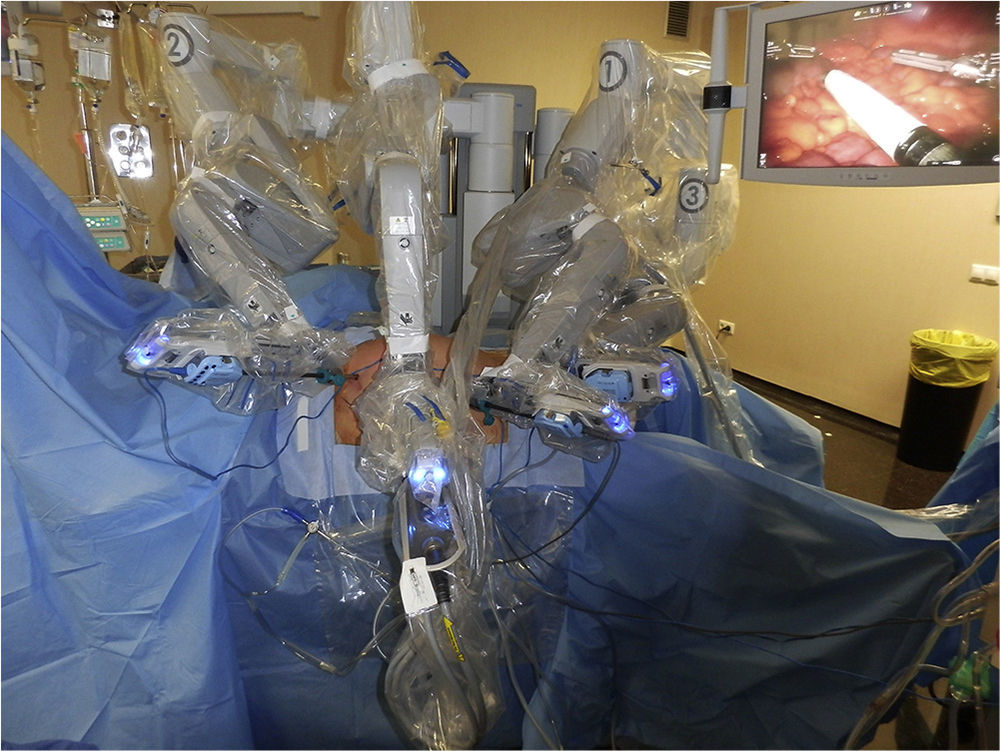
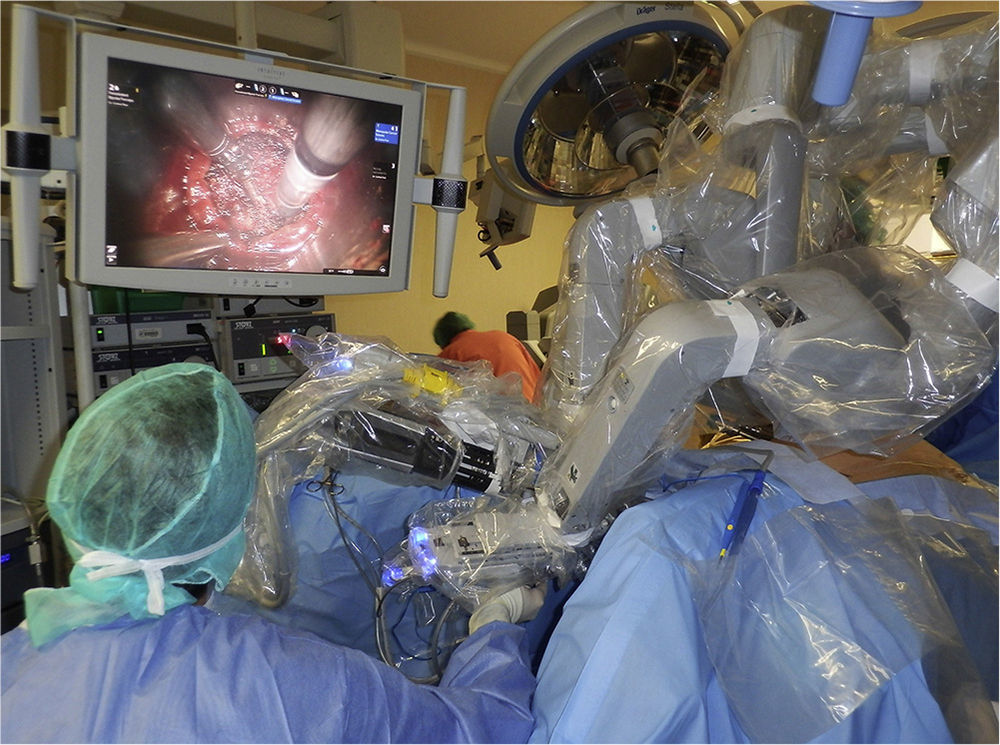
Initially, the left colon was completely mobilized by means of laparoscopy with the Da Vinci robot with the positioning of trocars shown in Fig. 3. The fenestrated bipolar forceps were used in arm 2, the monopolar scissors in arm 1 and the double-fenestrated grasper in 3. The optics used were 30°. The robot was anchored to the patient from the left as shown in Fig. 4. An approach was used between the transverse colon and greater omentum, separating the two. Once this phase of the operation was completed, the inferior mesenteric vein was ligated under the pancreas along with ligature of the inferior mesenteric artery to complete the mobilization of the left colon from medial to lateral. This abdominal phase was finalized by identifying the left ureter above the left iliac and passing the promontory, entering in the mesorectal plane. At this time, the mesocolon was transected at the sigmoid arteries.


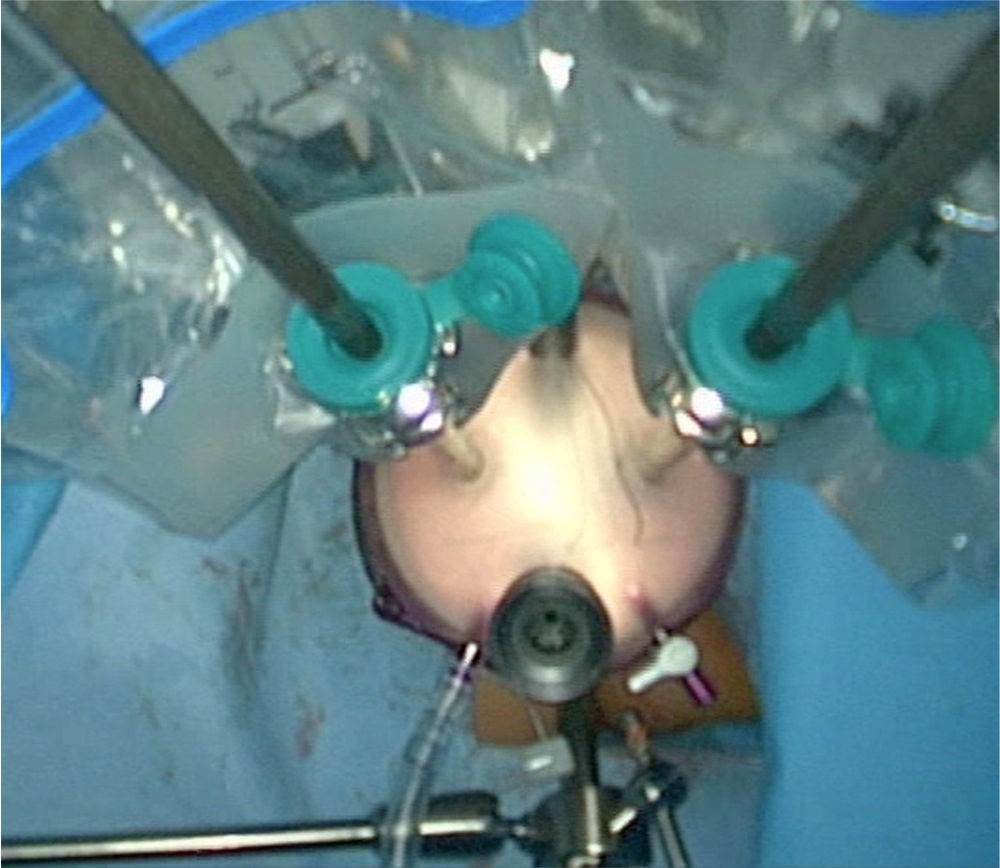
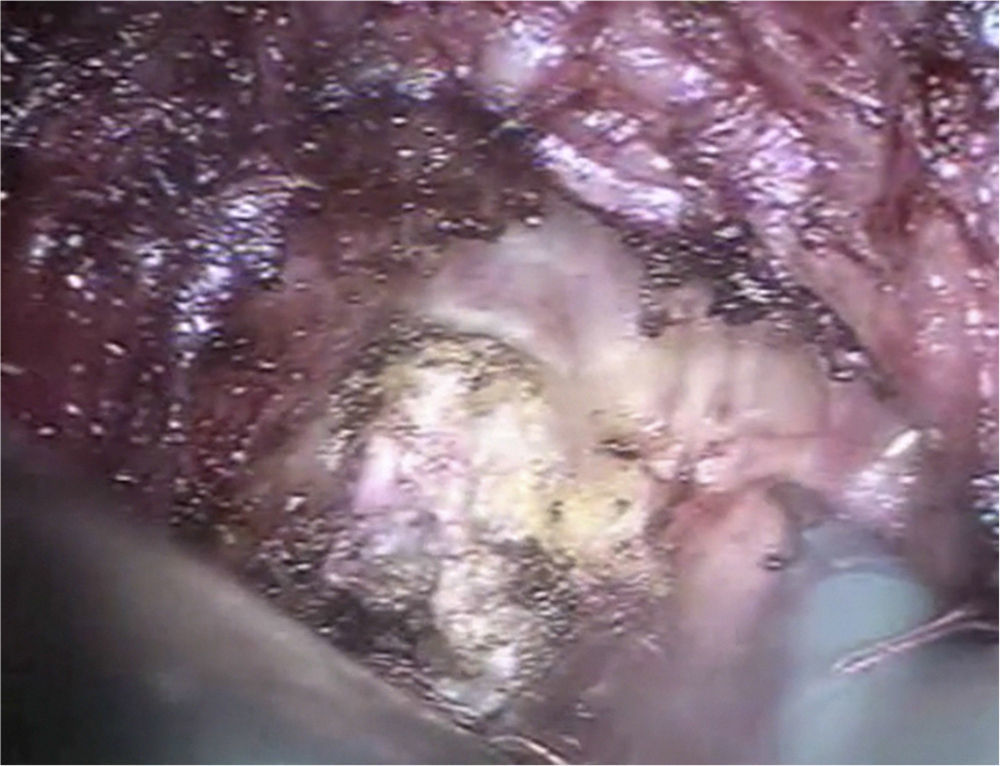
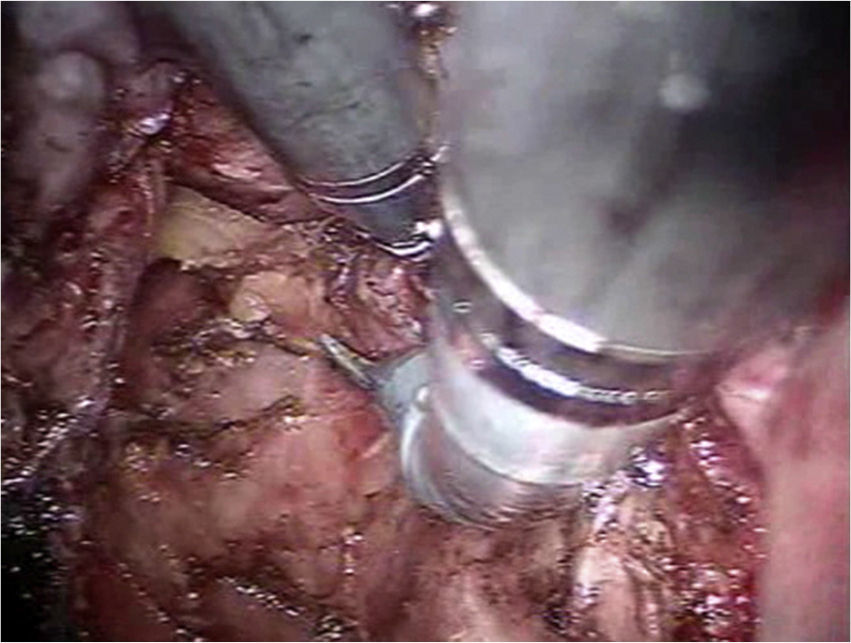
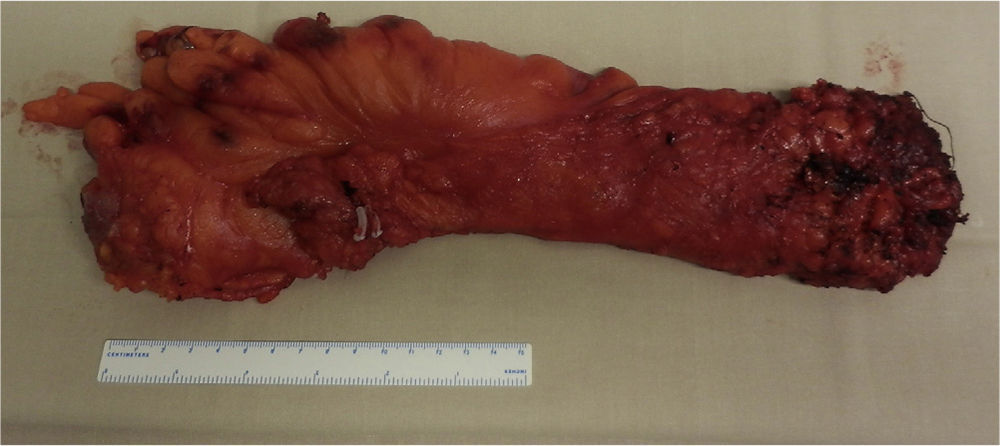
Afterwards, the transanal phase was begun with the closure of the rectal lumen 3cm above the dentate line through the proctoscope of the PHS stapler (Ethicon Endosurgery, Cincinnati, OH, USA), with a purse-string pouch. The proctoscope was then withdrawn and the transanal access port we have developed (PAT, Developia Inc., Spain) was used and secured to the surgical table with the static retraction arch (Karl Storz GmbH, Tuttlingen, Germany). The transanal access port was closed at the back with Gel-POINT (Applied Medical Inc., Rancho Santa Margarita, CA, USA). The optics trocar and 2 robotic work trocars were positioned together through the Gel-POINT with a trocar for the assistant (Fig. 5). The robot was anchored to the patient above the left leg as shown in Fig. 6. We used 30° optics, fenestrated bipolar forceps and monopolar scissors in the robot. The assistant used either atraumatic forceps or the suction instrument. Dissection was begun on the anterior side following the rectoprostatic fascia (Fig. 7) to open the bottom of the sac and connect with the peritoneal cavity. On the posterior and lateral sides, the mesorectal plane was followed (Fig. 8), and its dissection was aided by the traction done from the abdominal cavity by a second assistant. After completing the total mesorectal excision, the specimen was extracted through the anus (Fig. 9) and the colon was dissected at the level previously marked by the transection of the mesocolon. A purse-string was created and the anvil of the circular stapler (ILS 33mm, Ethicon Endosurgery, Cincinnati, OH, USA) was situated. The colon was reintroduced into the pelvic cavity and a purse-string was made at the rectal stump to close the lumen. Once this suture was completed, end-to-end colorectal anastomosis was performed with the ILS 33mm circular stapler. With laparoscopic assistance, an ileostomy was brought out at the site of the abdominal port located in the right iliac fossa.
Postoperative Follow-up




The patient underwent routine analytical controls, including inflammation markers: procalcitonin and C-reactive protein on the first, third and fifth days post-op. A follow-up CT on the sixth day post-op was also part of the protocol for the pilot study.
ResultsTotal anesthesia time was 420min. The abdominal robotic procedure was 110min and the transanal robotic procedure was 100min. The remaining time was for patient preparation, anchoring of the robotics, placement of the transanal access port, extraction of the surgical specimen, completion of the anastomosis and ileostomy. Intraoperative bleeding amounted to 100ml. The patient's postoperative hospital stay was 6 days, with no observed postoperative complications. The follow-up blood tests were normal, with procalcitonin levels of 0.08ng/ml on the first and third days, and 0.05ng/ml on the fifth day. Follow-up CT on the sixth day was normal, with no observed collections or anastomotic dehiscence.
The pathology study showed a stage I ypT2N0 adenocarcinoma on a surgical specimen measuring 33cm long and 2cm on the distal edge. A total of 29 negative lymph nodes were isolated. The circumferential margins were negative and the quality of the mesorectal excision was good (Fig. 9).
DiscussionTechnological advances made in recent years have led to the advent of minimally invasive surgery in the treatment of rectal cancer, providing better postoperative recovery. In spite of this, few hospital centers currently perform this type of interventions, mainly due to the technical complexity of these procedures, with conversion rates that are close to 20%, even in expert hands.4 These rates are even higher in male patients with voluminous tumors, obese patients and those with narrow pelvis, in whom postoperative complications are also more frequent.14 Transanal total mesorectal excision with laparoscopic assistance could be a good alternative for the treatment of tumors in the mid and lower thirds in this type of patients in whom the final third of the dissection or the rectal transection are occasionally very complicated in the anterior approach. This technique has been employed with TEO/TEM or SILS transanal ports, with which most groups (except Rouanet et al.11) have presented good postoperative and pathologic results.8–10,15
In this paper, we present the first experience with totally robotic transanal proctectomy for rectal cancer. Recently, Atallah et al. have reported a clinical case of robotic transanal proctectomy with a conventional laparoscope in a patient with colorectal polyposis. In our case, although it is possible to carry out the abdominal phase laparoscopically (and most of the time synchronically with robotic transanal proctectomy, thus saving surgical time), we have performed the entire procedure robotically with double anchoring of the robot in order to save on intraoperative material costs. The mobilization of the splenic angle and the transection of the inferior mesenteric vein lengthen the mobilized mesocolon, providing better descent of the colon. At the same time, this allows for tension-free anastomosis, which is undoubtedly an important factor for lowering the rate of deshiscence of this anastomosis, especially in patients who have received neoadjuvant chemoradiotherapy.16
Although the total surgical time presented in this case is excessive and longer than those of other publications, the robotic operative time is not that long; this leads us to believe that the total time can be reduced. Conventional laparoscopic left colon mobilization simultaneous to the robotic transanal phase would be feasible and could shorten surgical time even more.
Both the postoperative recovery of the patient and the pathology results were favorable. We therefore consider that this technique is a good option to keep in mind in complex cases such as an obese male with narrow pelvis and tumor in the mid to lower third of the rectum. Given that the patient is currently being treated with oral capecitabine and had an ileostomy, fecal continence has not been able to be evaluated, although from a theoretical standpoint it is not expected that a transanal mesorectal total excision would affect the patient functionally. The transanal access port used (PAT, Developia Inc., Spain) has endorectal dimensions similar to TEO/TEM, and no permanent disturbances have been shown in fecal continence with their use.17
Thus, the technique presented with robotic assistance is feasible with good initial results. It can facilitate transanal total mesorectal excision by providing a tridimensional view, better maneuverability of the robotic instruments and a more comfortable situation for the surgeon, who does not have to work under the technical difficulties and space inherent to TEO/TEM or SILS.
The rapid advances being made with the Da Vinci robot will probably make single-port access in the abdominal phase possible. This is another step in the direction toward the NOTES concept of this procedure, in which the single abdominal incision will be used for the construction of the ileostomy.
Conflicts of InterestDr. Gómez Ruiz collaborates with Intuitive Surgical, Inc. as proctor of colorectal robotic surgery. In addition, he has participated in studies about human factors and in the new applications of robotic technologies for Intuitive Surgical, Inc.
Dr. Alonso Martín collaborates with Intuitive Surgical, Inc. as proctor of colorectal robotic surgery.
We would like to thank the nursing staff at the Hospital Universitario Marqués de Valdecilla for their dedication to this project. Our special thanks to our families.
Please cite this article as: Gómez Ruiz M, Palazuelos CM, Martín Parra JI, Alonso Martín J, Cagigas Fernández C, del Castillo Diego J, et al. Nueva técnica de proctectomía trasanal con escisión total del mesorrecto totalmente robótica en el tratamiento del cáncer de recto. Cir Esp. 2014;92:356–361.
