



Intestinal malrotation is a congenital anomaly of the intestinal rotation and fixation, and usually occurs in the neonatal age.
ObjectiveDescription of a clinical case associated with acute occlusive symptoms.
Clinical caseA case of intestinal malrotation is presented in a previously asymptomatic woman of 46 years old with an intestinal obstruction, with radiology and surgical findings showing an absence of intestinal rotation.
ConclusionsIntestinal malrotation in adults is often asymptomatic, and is diagnosed as a casual finding during a radiological examination performed for other reasons. Infrequently, it can be diagnosed in adults, associated with an acute abdomen.
La malrotación intestinal es una anomalía congénita de la rotación y fijación intestinal, que se presenta generalmente en la edad neonatal.
ObjetivoDescripción de un caso clínico asociado a un cuadro oclusivo agudo.
Caso clínicoPresentamos el caso de una mujer de 46 años, previamente asintomática, atendida por un cuadro de obstrucción intestinal, con el hallazgo radiológico y quirúrgico de una ausencia de rotación intestinal.
ConclusionesLa malrotación intestinal en el adulto, frecuentemente es asintomática, y se diagnostica de una forma casual, en el curso de una exploración radiológica realizada por otra causa. De forma infrecuente puede diagnosticarse en adultos, asociado a un cuadro de abdomen agudo.
The term Intestinal malrotation may be defined as: a congenital anomaly of the intestinal rotation and fixation during the development of the foetus. A great variety of anomalies exist and these may remain asymptomatic throughout life or be accompanied by acute abdomen, generally in the form of associated intestinal volvulus.1
Changes in embryological intestinal development may occur in any of its phases and may be grouped in accordance with the corresponding development stage1:
- 1.
Non-rotation: here the small intestine is located on the right of the abdomen. The distal ileum crosses the midline to the caecum, located on the midline.
- 2.
Incomplete rotation: the intestine occupies an intermediate position between non rotation and standard layout.
- 3.
Inverse rotation: the duodenum crosses in front of the superior mesenteric artery, and the colon goes behind it. The duodenum is therefore in front, the superior mesenteric artery is behind it and behind this is the transverse colon.
In general malposition of the intestine in itself does not lead to problems, but it is often associated with bad intestinal adherence which may predispose to intestinal volvulus.
Clinical caseA patient aged 46 with no clinical history of note, presented at the emergency department with a three-day history of repeated vomiting and absence of bowel movements. The patient had previously presented at a hospital on 2 occasions, but without any organic causes. On this occasion symptoms included abdominal pain of epigastric origin, which was later diffuse. On examination the abdomen was found to be swollen and slightly painful, without peritoneal irritation.
Blood count was normal, biochemical studies revealed a slight increase in urea and creatine and a PCR of 2.4. A simple X-ray of the abdomen showed swelling of the small intestine loops, compatible with a partial bowel obstruction.
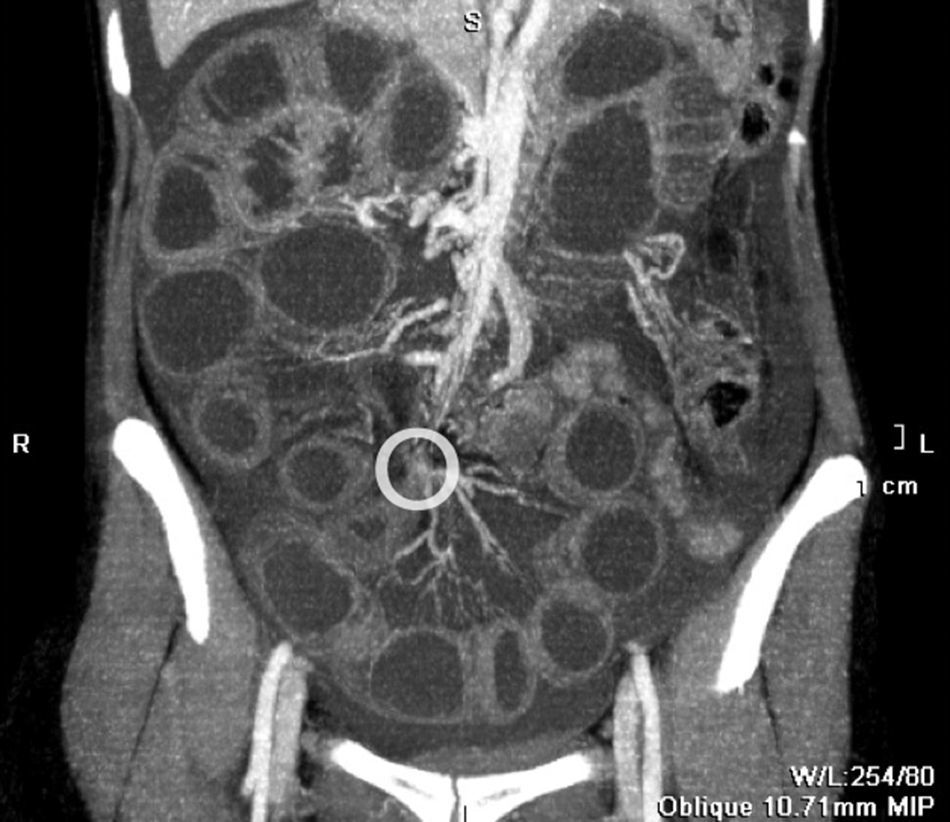
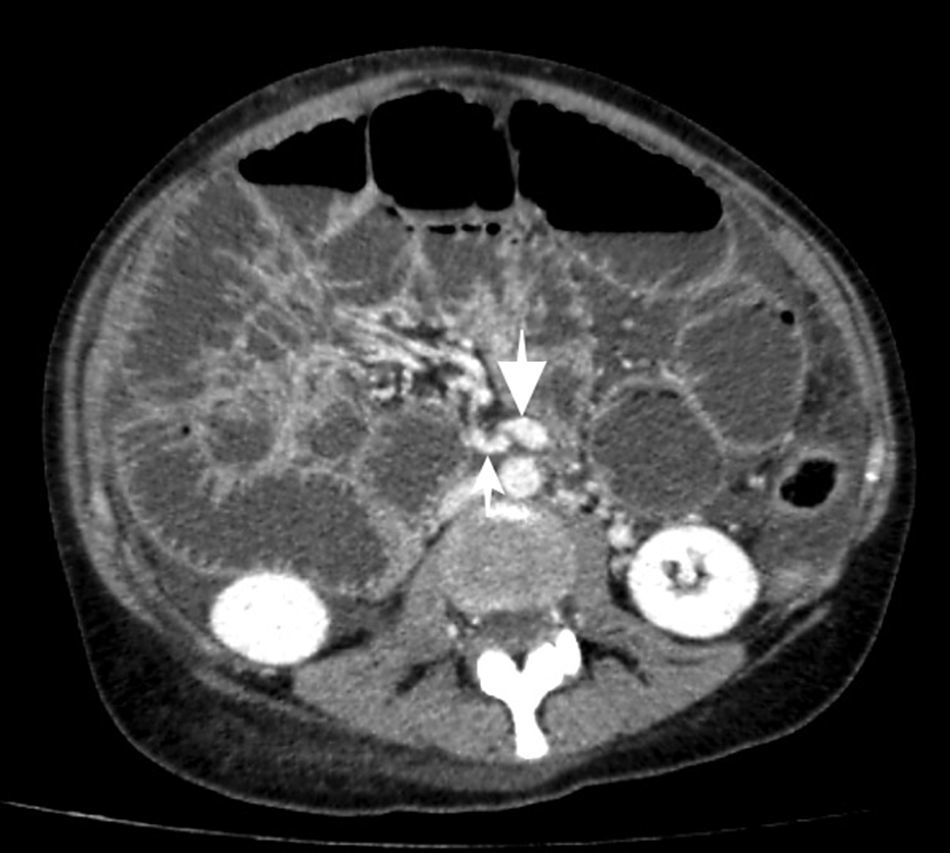
The patient was admitted to the service of digestive medicine and following exacerbation of pain during the next few hours, computed axial tomography (CAT) of the abdomen was requested. This showed swelling of the small intestine loops in the right abdomen, displacing the caecum to a posterior and central position (Fig. 1). There was also abundant free fluid indicative of loop impairment and focused grouping of mesenteric vessels, suggestive of internal hernia or torsion (Fig. 2). The radiologist suggested a primary diagnosis of pericaecal internal hernia. Retrospectively an inversion of mesenteric vessels was observed (Fig. 3).
. Abnormal position of caecum, located mid line (arrow).")
, responsible for occlusion.")
 located to the right of the superior mesenteric vein (thick arrow).")
A surgical assessment was requested and on examination the patient presented with a very swollen, diffusely painful abdomen, low peristalsis and considerable compromise of the patient's general health status.
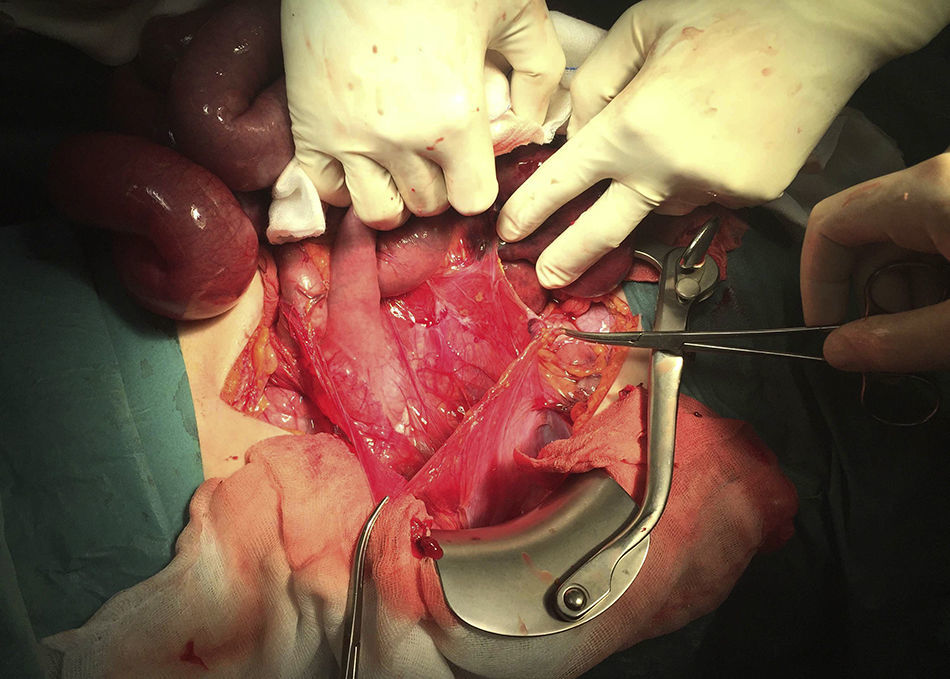
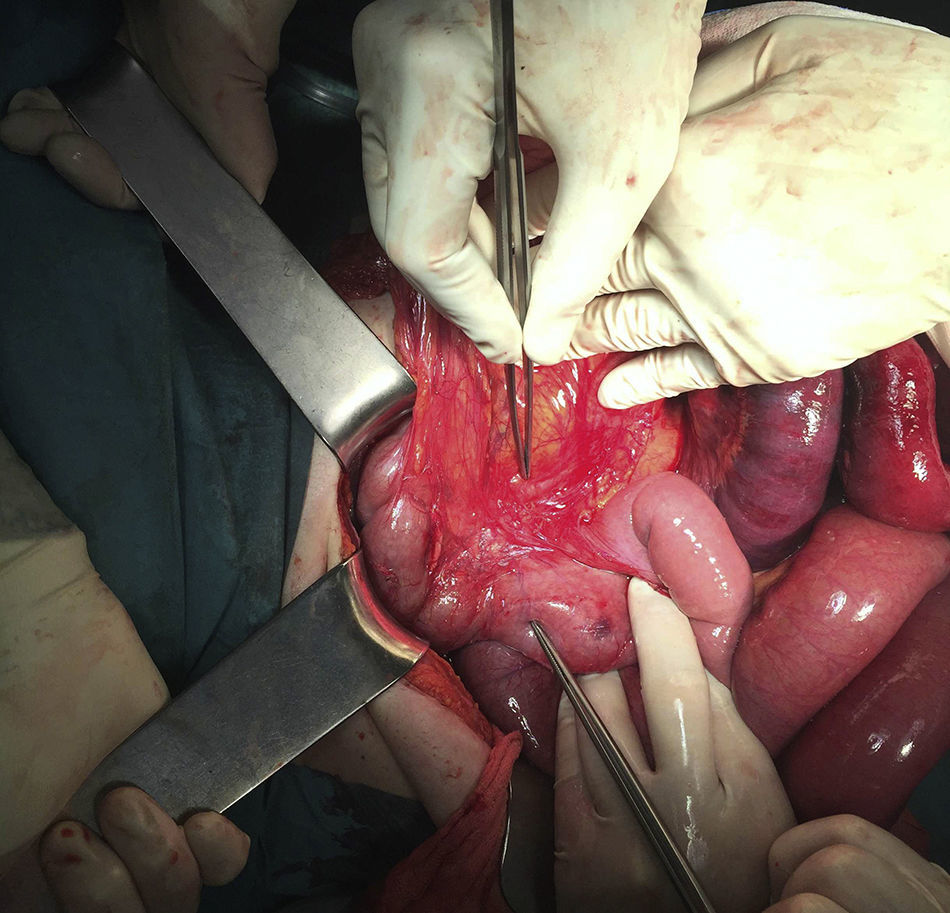
Emergency surgery was performed, with an exploratory laparotomy, which revealed the beginning of an irreversible intestinal ischaemia of 150cm of ileum and a large herniated sac in the right abdomen, with the caecum in medial position and almost 1l of intra-abdominal fluid.
The herniated sac which contained dilated jejunum was opened and resected and we confirmed the existence of an intestinal malrotation existing from the angle of Treitz to the left of the mesenteric vessels, in addition to an intestinal volvulus (Figs. 4 and 5).


Removal of the largest part of the mesenteric sac and resection of 150cm of the compromised intestine was performed, remaining 300cm above and 16cm from the end of the ileum, with side-to-side manual isoperistaltic anastomosis.
The postoperative period passed without event and the patient was discharged 7 days after surgery.
DiscussionIntestinal malrotation is determined by an interruption or alteration of the embryological development of the midgut, in any of its phases, whereby it divides into 2 parts through the superior mesenteric artery axis. The proximal part, which later becomes the duodenal-jejunal loop, is located above and anterior to the superior mesenteric artery. The distal part is posterior and inferior to the artery and becomes the ileum, ascending colon and proximal transverse colon.
Prevalence in adults is estimated to be 0.2%,2 and it is mainly asymptomatic, and diagnosed as a casual finding during a radiological examination performed for other reasons. Diagnosis in adults is difficult due to low incidence and the CAT scan is the technique of choice.3,4
What is characteristic about the CAT scan is the medial position of the caecum and the lateral position of the small intestine loops, and inversion of mesenteric vessels. In our case, which was complicated by a volvulus, there was dilation of the small intestine loops, free fluid and grouping of mesenteric vessels, similar to agitated vessels.
On other occasions we may refer to chronic symptoms with episodes of abdominal pain and vomiting, even evidence of malnutrition associated with malabsorption, due to intermittent chronic volvulus. The incidence of intestinal volvulus is high (33% of cases) regardless of age, and acute abdomen should therefore be treated as an emergency.5
Defining the exact type of malrotation is of little clinical interest since they all predispose to volvulus, and the important point is to diagnose the existence of volvulus. Treatment is surgical, with devolvulation of the small intestine loops, releasing the membranes attached to them, separating the common meso colon and an appendectomy, given that the abnormal situation of the caecum inhibits a posterior diagnosis of appendicitis.
ConclusionsThe clinical presentation of intestinal malrotation in an adult is asymptomatic in the majority of cases. Diagnosis is usually coincidental to radiological examination, usually from computed tomography performed for a different reason. It is infrequently associated with acute abdomen, where diagnosis occurs during laparotomy.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Hernando-Almudí E, Cerdán-Pascual R, Vallejo-Bernad C, Martín-Cuartero J, Sánchez-Rubio M, Casamayor-Franco M. Malrotación intestinal en adulto asociada a vólvulo intestinal. Cirugía y Cirujanos. 2017;85:424–427.