





Pragmatics is an area of language that may be impaired in a wide variety of disorders. However, there is a dearth of instruments for the assessment of pragmatic abilities. The Children's Communication Checklist (CCC-2) is the most widespread test, although more adaptations of this instrument to other languages are necessary.
AimsIn this paper we (1) develop a pilot study to adapt the CCC-2 to the Galician language, (2) check the capacity of this version to assess communicative difficulties in Galician speakers from 4 to 16 years of age, and (3) we also check its capacity to discriminate the linguistic profiles of different disorders.
MethodThe reference profile of the Galician CCC-2 was established with a sample of 48 schoolchildren. Comparisons of the scores obtained by children with ASD (n=11), ADHD (n=10), Down Syndrome (DS) (n=9) and Typical Development (n=10) were carried out.
ResultsThe Galician CCC-2 (1) accurately identified children with and without communicative impairments, (2) distinguished between profiles with predominance of pragmatic (ASD and ADHD) and structural disorders (DS), and (3) distinguished between different profiles with predominance of pragmatic impairment.
ConclusionsThe Galician CCC-2 seems to be a useful instrument to assess pragmatic disorders and to differentiate among different clinical groups.
La pragmática es un área del lenguaje que puede verse afectada en una amplia variedad de trastornos. Sin embargo, hay una escasez de instrumentos para la evaluación de las habilidades pragmáticas. El Children's Communication Checklist (CCC-2) es la prueba más utilizada, aunque se necesitan más adaptaciones de este instrumento a otros idiomas.
ObjetivosEn este documento 1)desarrollamos un estudio piloto para adaptar el CCC-2 al gallego; 2)comprobamos la capacidad de esta versión para evaluar las dificultades comunicativas en hablantes de gallego de 4 a 16años, y 3)también comprobamos su capacidad para discriminar perfiles lingüísticos de diferentes trastornos.
MétodoEl perfil de referencia del CCC-2 gallego se estableció con una muestra de 48 escolares. Se realizaron comparaciones de las puntuaciones obtenidas por los niños con TEA (n=11), TDAH (n=10), síndrome de Down (SD; n=9) y desarrollo normal (n=10).
ResultadosEl CCC-2 gallego 1)identificó con precisión a los niños con trastornos comunicativos y sin ellos; 2)distinguió entre los perfiles con predominio de trastornos pragmáticos (TEA y TDAH) y estructurales (SD), y 3)distinguió entre los diferentes perfiles con predominio del deterioro pragmático.
ConclusionesParece que el CCC-2 gallego es un instrumento útil para evaluar trastornos pragmáticos y para diferenciar entre diferentes grupos clínicos.
Pragmatics has received less attention than other dimensions of language, and there is even a lack of agreement on its precise definition (Airenti, 2017; Perkins, 2010). The American Speech Language and Hearing Association (ASHA, 2015) considers that pragmatics includes: (1) to carry out different speech acts, (2) to modify language in relation to the interlocutor's needs or to the situation, and (3) to follow the rules of conversation and narration.
These abilities are altered, to different degrees of severity, in multiple impairments. The impairment of pragmatic abilities can be found in the Social Communication Disorder (SCD) (also called Pragmatic Language Impairment), as well as in the Autism Spectrum Disorder (ASD), the Specific Language Impairment (SLI), the Attention Deficit with Hyperactivity Disorder (ADHD), the Down syndrome (DS), the Williams syndrome, the X-fragile syndrome, cerebral damage, among others.
SCD is the most representative pragmatic deficit. Recently incorporated in the DSM-5, SCD is characterized by persistent difficulties in use of communication for social purposes, its adaptation to the context and the interlocutor's needs, the capacity to follow conversational and narration rules, and non-literal, ambiguous or implicit meaning understanding (Norbury, 2014).
ASD children also show pragmatic impairment. Around 20–25% of these children do not have functional language (Rodríguez-Santos, 2016; Tager-Flusberg, Paul, & Lord, 2005). Among those who have oral language there are different profiles, with pragmatic alterations being a universal and distinctive feature of ASD (Kjelgaard & Tager-Flusberg, 2001; Sotillo, 2002; Volden, 2017). The majority of pragmatic abilities are altered (Eigsti, de Marchena, Schuh, & Kelley, 2011; Martín-Borreguero, 2005), including difficulties to initiate and maintain conversations, respect conversational turns, understanding non- literal meaning, or narratives use and comprehension (Eigsti et al., 2011; Rice, Warren, & Betz, 2005).
Pragmatic difficulties are also frequent in people with ADHD (Kim & Kaiser, 2000; Korrell, Mueller, Silk, Anderson, & Sicberras, 2017; Staikova, Gomes, Tartter, McCabe, & Halperin, 2013), and they are included as diagnostic criteria of this deficit (Westby & Watson, 2010). The communicative difficulties of ADHD and high functioning ASD children are similar, although less severe in ADHD children. In both cases, pragmatic difficulties surpass structural difficulties (Geurts & Embrechts, 2008; Helland, Biringer, Helland, & Heimann, 2012).
Regarding Down syndrome, pragmatic aspects are an area of relative strength, while structural aspects are an area with difficulties, particularly phonology and syntax (Martin, Klusek, Estigarribia, & Roberts, 2009; Rice et al., 2005; Vicari, Caselli, & Tonucci, 2000). In any case, pragmatic competence is lower when compared to children with typical development (TD), since overall linguistic development is lower in Down syndrome children in comparison to TD children with equivalent mental age.
In spite of the existence of pragmatic alterations in a variety of disorders, adequate assessment instruments are scarce (Bishop & Baird, 2001; Hyter, 2017). Among the existing tools, pragmatic abilities checklists are considered to be the most adequate (Carballo, 2012; Norbury, Nash, Baird, & Bishop, 2004; O’Neil, 2014). They consist of a list of abilities that parents or teachers have to score on the basis of their knowledge of the child. Checklists offer representative information of the behaviors observed in different contexts over a long period of time (Bishop, 1998), which an external observer could not identify (Adams, 2002).
The Children's Communication Checklist – 2 (CCC-2) (Bishop, 2003) is a remarkable tool, “which has rapidly become the instrument of choice for the identification of pragmatic language impairment” (Adams, 2002, p. 976). It is widely used in clinical practice as well as in research, where the CCC-2 has been used for the comparison of different linguistic profiles: ASD and ADHD (Geurts et al., 2004; Helland et al., 2012), ASD, ADHD and SLI (Bishop & Baird, 2001; Geurts & Embrechts, 2008), ASD and Down syndrome (Mendoza & Garzón, 2012), ASD and Williams syndrome (Philofsky, Fidler, & Hepburn, 2007).
The CCC-2 has been adapted to different cultural and linguistic environments: Finland (Väisänen, Loukusa, Moilanen, & Yliherva, 2014), Norway (Helland, Biringer, Helland, & Heimann, 2009), the Netherlands (Ketelaars, Cuperus, van Daal, Jansonius, & Verhoeven, 2009), Quebec (Vézina, Samson-Morasse, Gauthier-Desgagné, Fossard, & Sylvestre, 2011), Serbia (Glumbić & Brojčin, 2012), Brazil (Barbosa, Harsányi, de Oliveira, & Kummer, 2013), and Thailand (Chuthapisith, Taycharpipranai, Roongpraiwan, & Ruangdaraganon, 2014). In Spain only a few scales of the first version of the CCC have been adapted (Crespo-Eguílaz, Magallón, Sánchez-Carpintero, & Narbona, 2016), although no validation or standardization has been carried out. No adaptation of the CCC-2 to Galician exists.
Given the influence of culture on pragmatics and the impossibility of generalizing from the results obtained in other languages, we aim to carry out a pilot study to create the Galician version of the CCC-2. Our objectives are (1) to establish a reference profile in a sample of school age Galician children, and (2) to determine the capacity of this version to differentiate between TD and atypical children (ASD, ADHD, and DS), as well as (3) to differentiate between different profiles of pragmatic impairment.
We hope that the improvement of our knowledge of the communicative and linguistic profiles of these frequent impairments (ASD, ADHD and DS) through the CCC-2 will favor the implementation of appropriate interventions.
MethodParticipantsThe criteria to include children in the study were that they all had to have oral language and be able to combine at least 3 words. Galician had to be their dominant language, and no hearing loss or comorbid impairment could be present.
The children with ASD and ADHD had to have an average IQ (>85). The children from the DS group included children with low IQ, because this is a characteristic associated with this profile. The group of ASD was made up of children with High Functioning and Asperger syndrome.
A group of 48 TD children was chosen to establish the normative scores of the instrument. For the remaining analyses, and to compare groups with a similar number of participants, 10 children were randomly selected from the 48 TD children, and these formed the control group (CG). The group of ASD was formed by 11 children, the ADHD group by 10, and the DS group by 9 children.
The children were previously diagnosed by experts, as reported by the parents.
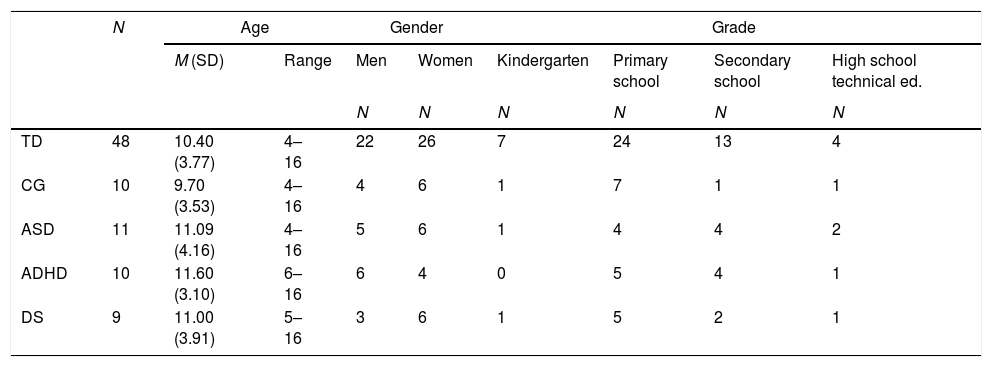
The characteristics of the 5 groups of children can be observed in Table 1.
Sociodemographic characteristics of the children.
| N | Age | Gender | Grade | ||||||
|---|---|---|---|---|---|---|---|---|---|
| M (SD) | Range | Men | Women | Kindergarten | Primary school | Secondary school | High school technical ed. | ||
| N | N | N | N | N | N | ||||
| TD | 48 | 10.40 (3.77) | 4–16 | 22 | 26 | 7 | 24 | 13 | 4 |
| CG | 10 | 9.70 (3.53) | 4–16 | 4 | 6 | 1 | 7 | 1 | 1 |
| ASD | 11 | 11.09 (4.16) | 4–16 | 5 | 6 | 1 | 4 | 4 | 2 |
| ADHD | 10 | 11.60 (3.10) | 6–16 | 6 | 4 | 0 | 5 | 4 | 1 |
| DS | 9 | 11.00 (3.91) | 5–16 | 3 | 6 | 1 | 5 | 2 | 1 |
The ASD, ADHD, DS and CG children were equivalent in terms of age (F=.48; df=3,36; p=.70), gender (χ2=1.51; df=3; p=.68) and educational level (χ2=4.67; df=9; p=.86).
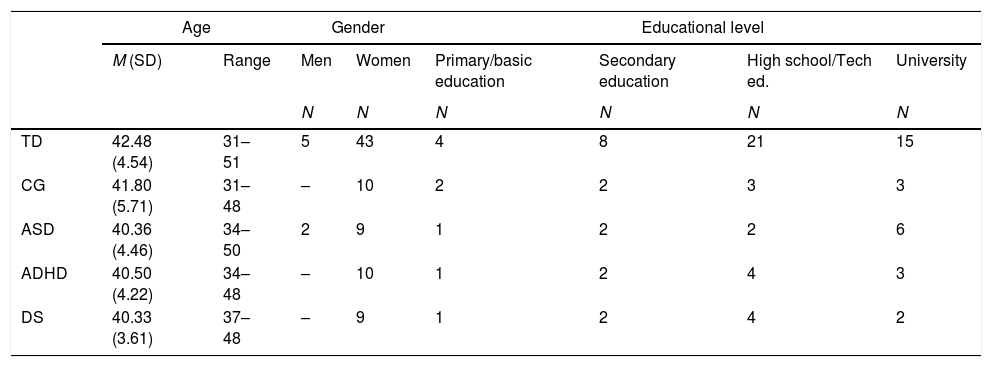
Regarding the respondents, most of them were mothers. One hundred percent of the respondents in the groups of ADHD, DS and CG children were mothers, while 10.4% of the respondents were fathers in the TD children group. For the group of ASD children, 54.5% were teachers (4 men and 6 women). Demographic characteristics of the respondents are displayed in Table 2. The respondents were equivalent in terms of age (F=.24; df=3,36; p=.87), gender (χ2=5.55; df=3; p=.14) and educational level (χ2=3.70; df=9; p=.93).
Sociodemographic characteristics of the informants.
| Age | Gender | Educational level | ||||||
|---|---|---|---|---|---|---|---|---|
| M (SD) | Range | Men | Women | Primary/basic education | Secondary education | High school/Tech ed. | University | |
| N | N | N | N | N | N | |||
| TD | 42.48 (4.54) | 31–51 | 5 | 43 | 4 | 8 | 21 | 15 |
| CG | 41.80 (5.71) | 31–48 | – | 10 | 2 | 2 | 3 | 3 |
| ASD | 40.36 (4.46) | 34–50 | 2 | 9 | 1 | 2 | 2 | 6 |
| ADHD | 40.50 (4.22) | 34–48 | – | 10 | 1 | 2 | 4 | 3 |
| DS | 40.33 (3.61) | 37–48 | – | 9 | 1 | 2 | 4 | 2 |
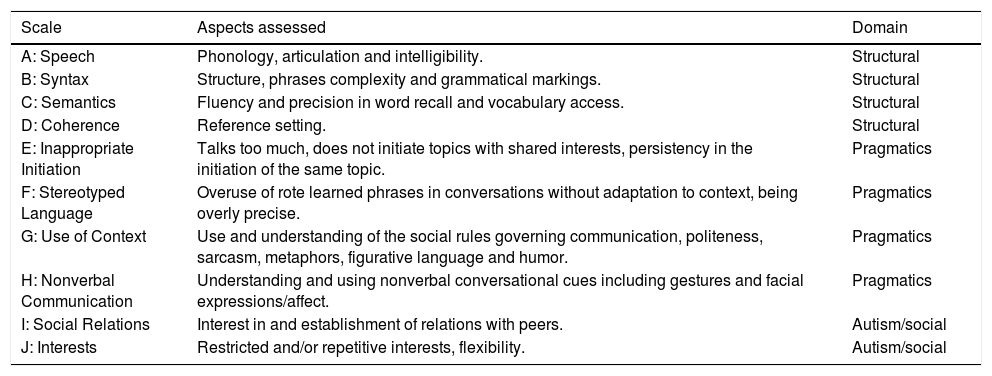
The instrument used was the Galician version of the CCC-2, which has 70 items, distributed into 10 scales (see Table 3). Scales A–D assess structural domain abilities of language, while scales E–H assess pragmatic domain abilities. Scales I and J gather information on social communication. Each scale has 5 items concerning difficulties and 2 items concerning strengths.
Scales of the CCC-2.a
| Scale | Aspects assessed | Domain |
|---|---|---|
| A: Speech | Phonology, articulation and intelligibility. | Structural |
| B: Syntax | Structure, phrases complexity and grammatical markings. | Structural |
| C: Semantics | Fluency and precision in word recall and vocabulary access. | Structural |
| D: Coherence | Reference setting. | Structural |
| E: Inappropriate Initiation | Talks too much, does not initiate topics with shared interests, persistency in the initiation of the same topic. | Pragmatics |
| F: Stereotyped Language | Overuse of rote learned phrases in conversations without adaptation to context, being overly precise. | Pragmatics |
| G: Use of Context | Use and understanding of the social rules governing communication, politeness, sarcasm, metaphors, figurative language and humor. | Pragmatics |
| H: Nonverbal Communication | Understanding and using nonverbal conversational cues including gestures and facial expressions/affect. | Pragmatics |
| I: Social Relations | Interest in and establishment of relations with peers. | Autism/social |
| J: Interests | Restricted and/or repetitive interests, flexibility. | Autism/social |
Responses are given by parents, teachers or any person who has had frequent contact with the child, and are gathered through a Likert type scale of 4 points, based on the frequency of the behaviors asked for.
Different composite scores can be calculated. The General Communication Composite (GCC) is the result of the addition of the scores obtained in the first 8 scales (A–H). This index allows us to identify those children or adolescents with clinically significant problems of communication. Given that there are no scaled scores for the Galician version, and we work only with direct scores, high scores indicate higher levels of language impairment. A Social Interaction Deficit Index (SIDC) can also be obtained, which is the result of the difference between (E+H+I+J)−(A+B+C+D), which indicates to what extent pragmatic abilities are higher or not, in relation to structural abilities. A positive value would indicate higher pragmatic difficulties, which makes a difference with the English version since scaled scores are provided (Bishop, 2003).
In addition to these two composite scores, and following the criteria of Philofsky et al. (2007), we have also calculated a General Pragmatic Index (GPI). (E+F+G+H), a General Structural Index (GSI) (A+B+C+D), and a Social Communication Index (SCI) (I+J).
ProcedureThe Galician CCC-2 was administered individually in a cross-sectional design. Previous informed consent was obtained from the parents, as well as sociodemographic information.
The TD sample was gathered by phone at home or at school venues. The children with previous diagnosis of impairment were contacted through associations or private psychology clinics.
AnalysisThe statistical package SPSS 20.0 version was used for the analyses.
First, the reliability (internal consistency) of the instrument was checked through Cronbach's alpha coefficient.
A discriminant analysis was performed to check the capacity of the Galician CCC-2 to classify the participants in the 3 different clinical groups (ASD, ADHD and DS) and the CG, from the scores obtained in the GCC and the SIDC. Descriptive results were also obtained for the TD group.
Comparisons were made among the CG, ASD, ADHD and DS groups through different ANOVA analyses with the 10 scales and the 5 composite scores as dependent variables, using the diagnostic group as grouping factor. Bonferroni's post hoc analyses were carried out when equal variance was assumed, and the Games-Howell test when there were not equal variances. Size effects were also calculated for every scale and composite score.
ResultsThe study of reliability with the ASD, ADHD and DS and CG showed a Cronbach's alpha score of .91 for the 10 scales together. The internal consistency for each scale is shown in Table 4.
Cronbach's alpha and norming scores (mean and standard deviation) for the different scales and composite scores obtained in the TD group.
| Scale | A | B | C | D | E | F | G | H | I | J | GCC | SIDC | GPI | GSI | SCI |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cronbach's Alpha | .95 | .90 | .64 | .84 | .79 | .81 | .82 | .81 | .69 | .78 | |||||
| M | .73 | .50 | 1.69 | .90 | 2.98 | 1.12 | 1.79 | 1.12 | 1.29 | 3.19 | 10.83 | 4.77 | 7.02 | 3.81 | 4.48 |
| SD | 1.28 | 1.11 | 1.49 | 1.23 | 2.35 | 1.66 | 1.76 | 1.10 | 1.53 | 2.69 | 8.63 | 4.90 | 5.33 | 4.10 | 3.16 |
Note: Range: 0–21 for scales A–J; 0–168 for GCC; 84–168 for SIDC; 0–84 for GPI and GSI; 0–42 for SCI.
Discriminant analysis indicated that the Galician CCC-2 correctly classified 97.5% of the participants into the CG or any of the three clinical groups (ASD, ADHD and DS) from the scores obtained in the GCC and the SIDC scores. In addition, the Galician CCC-2 discriminates among the different clinically significant profiles, correctly classifying 92.5% of the participants.
Mean and standard deviation of direct scores obtained by the TD group (n=48) were calculated, for them to serve as a reference point. These are displayed in Table 4.
In general terms, the level of language difficulties (GCC) is low in the TD group, with low mean scores in every scale (see Table 4), which indicate good ability.
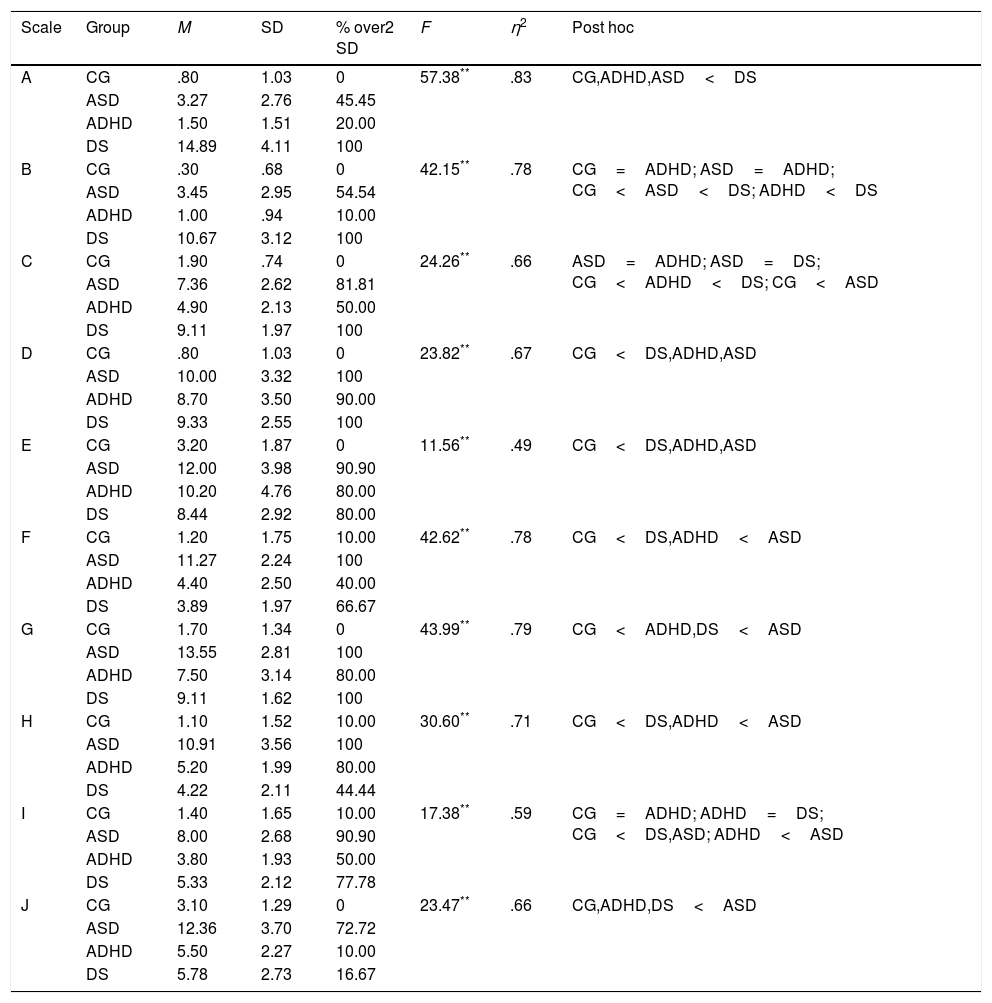
Table 5 shows the descriptive statistics of each group in the 10 CCC-2 scales, the percentage of participants who deviate over 2 SD scores from the reference values of the TD participants, and the results of the ANOVA analyses performed in order to test differences in the 10 scales between the CG group and the 3 clinical groups.
Descriptive results and ANOVA comparisons among the CG, ASD, ADHD and DS groups in the 10 scales of the Galician CCC-2.
| Scale | Group | M | SD | % over2 SD | F | η2 | Post hoc |
|---|---|---|---|---|---|---|---|
| A | CG | .80 | 1.03 | 0 | 57.38** | .83 | CG,ADHD,ASD<DS |
| ASD | 3.27 | 2.76 | 45.45 | ||||
| ADHD | 1.50 | 1.51 | 20.00 | ||||
| DS | 14.89 | 4.11 | 100 | ||||
| B | CG | .30 | .68 | 0 | 42.15** | .78 | CG=ADHD; ASD=ADHD; CG<ASD<DS; ADHD<DS |
| ASD | 3.45 | 2.95 | 54.54 | ||||
| ADHD | 1.00 | .94 | 10.00 | ||||
| DS | 10.67 | 3.12 | 100 | ||||
| C | CG | 1.90 | .74 | 0 | 24.26** | .66 | ASD=ADHD; ASD=DS; CG<ADHD<DS; CG<ASD |
| ASD | 7.36 | 2.62 | 81.81 | ||||
| ADHD | 4.90 | 2.13 | 50.00 | ||||
| DS | 9.11 | 1.97 | 100 | ||||
| D | CG | .80 | 1.03 | 0 | 23.82** | .67 | CG<DS,ADHD,ASD |
| ASD | 10.00 | 3.32 | 100 | ||||
| ADHD | 8.70 | 3.50 | 90.00 | ||||
| DS | 9.33 | 2.55 | 100 | ||||
| E | CG | 3.20 | 1.87 | 0 | 11.56** | .49 | CG<DS,ADHD,ASD |
| ASD | 12.00 | 3.98 | 90.90 | ||||
| ADHD | 10.20 | 4.76 | 80.00 | ||||
| DS | 8.44 | 2.92 | 80.00 | ||||
| F | CG | 1.20 | 1.75 | 10.00 | 42.62** | .78 | CG<DS,ADHD<ASD |
| ASD | 11.27 | 2.24 | 100 | ||||
| ADHD | 4.40 | 2.50 | 40.00 | ||||
| DS | 3.89 | 1.97 | 66.67 | ||||
| G | CG | 1.70 | 1.34 | 0 | 43.99** | .79 | CG<ADHD,DS<ASD |
| ASD | 13.55 | 2.81 | 100 | ||||
| ADHD | 7.50 | 3.14 | 80.00 | ||||
| DS | 9.11 | 1.62 | 100 | ||||
| H | CG | 1.10 | 1.52 | 10.00 | 30.60** | .71 | CG<DS,ADHD<ASD |
| ASD | 10.91 | 3.56 | 100 | ||||
| ADHD | 5.20 | 1.99 | 80.00 | ||||
| DS | 4.22 | 2.11 | 44.44 | ||||
| I | CG | 1.40 | 1.65 | 10.00 | 17.38** | .59 | CG=ADHD; ADHD=DS; CG<DS,ASD; ADHD<ASD |
| ASD | 8.00 | 2.68 | 90.90 | ||||
| ADHD | 3.80 | 1.93 | 50.00 | ||||
| DS | 5.33 | 2.12 | 77.78 | ||||
| J | CG | 3.10 | 1.29 | 0 | 23.47** | .66 | CG,ADHD,DS<ASD |
| ASD | 12.36 | 3.70 | 72.72 | ||||
| ADHD | 5.50 | 2.27 | 10.00 | ||||
| DS | 5.78 | 2.73 | 16.67 |
aScore variation between 0 and 21.
The DS group obtains higher mean scores than the other groups in the first three scales (A–C), indicating that these aspects of the structural domain are highly impaired in the DS participants. The high mean score obtained in scale A (Speech) is remarkable. Although scale D (Coherence) also evaluates a structural aspect of language, in this case the groups ASD and ADHD obtain similar scores to those of the DS group (high scores). In scales E–H (pragmatics) the ASD group obtained the highest mean scores, indicating a more serious pragmatic impairment in this group. In scales F, G and H, the mean scores obtained by the ASD group are significantly higher when compared to the other groups. In scale E (Inappropriate initiation), however, the ADHD and the DS groups obtained results similar to those of the ASD group, indicating that these groups share a common impairment in this scale ability. In the four pragmatic scales, the group of DS children does not have significant differences with the ADHD group. Finally, the mean scores obtained by the ASD group in scales I and J (social communication and interests) are significantly higher in comparison to the other groups, as expected.
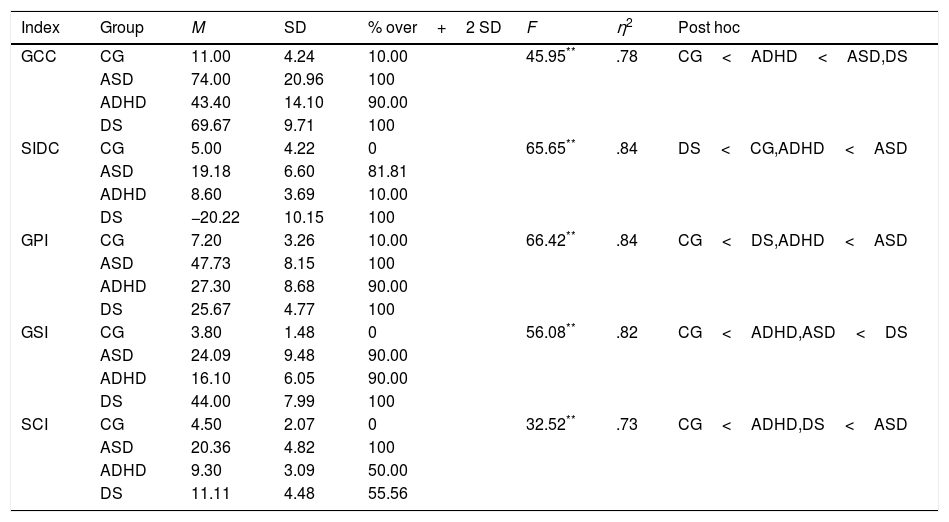
Table 6 shows the descriptive results of each group in composite scores, the percentage of participants who deviate over 2 SD scores from the reference values of the TD participants, and the results of the ANOVA analyses performed to test differences in the composite scores between the CG group and the 3 clinical groups.
Descriptive results and ANOVA comparisons among the CG, ASD, ADHD and DS groups in the different composite scores of the Galician CCC-2.
| Index | Group | M | SD | % over+2 SD | F | η2 | Post hoc |
|---|---|---|---|---|---|---|---|
| GCC | CG | 11.00 | 4.24 | 10.00 | 45.95** | .78 | CG<ADHD<ASD,DS |
| ASD | 74.00 | 20.96 | 100 | ||||
| ADHD | 43.40 | 14.10 | 90.00 | ||||
| DS | 69.67 | 9.71 | 100 | ||||
| SIDC | CG | 5.00 | 4.22 | 0 | 65.65** | .84 | DS<CG,ADHD<ASD |
| ASD | 19.18 | 6.60 | 81.81 | ||||
| ADHD | 8.60 | 3.69 | 10.00 | ||||
| DS | −20.22 | 10.15 | 100 | ||||
| GPI | CG | 7.20 | 3.26 | 10.00 | 66.42** | .84 | CG<DS,ADHD<ASD |
| ASD | 47.73 | 8.15 | 100 | ||||
| ADHD | 27.30 | 8.68 | 90.00 | ||||
| DS | 25.67 | 4.77 | 100 | ||||
| GSI | CG | 3.80 | 1.48 | 0 | 56.08** | .82 | CG<ADHD,ASD<DS |
| ASD | 24.09 | 9.48 | 90.00 | ||||
| ADHD | 16.10 | 6.05 | 90.00 | ||||
| DS | 44.00 | 7.99 | 100 | ||||
| SCI | CG | 4.50 | 2.07 | 0 | 32.52** | .73 | CG<ADHD,DS<ASD |
| ASD | 20.36 | 4.82 | 100 | ||||
| ADHD | 9.30 | 3.09 | 50.00 | ||||
| DS | 11.11 | 4.48 | 55.56 |
The GCC score obtained by the CG is significantly lower than any of the other three clinical groups, while GCC scores of the ASD and the DS groups were higher, indicating greater linguistic impairment.
The SIDC index reveals negative values in the DS children, indicating the prevalence of structural over social pragmatic impairments in this group. All the other groups show positive values in the SIDC (we do not use scaled scores, at difference with the manual of the English version), which indicates that socio-pragmatic difficulties are more important than the structural ones. The difference between the scores obtained in the structural scales and the pragmatic scales is particularly significant in the case of the ASD group.
In relation to the GPI, Table 6 shows that ASD children show the highest pragmatic impairment level, while DS children show the highest structural impairment in the GSI. With regard to social communication (SCI), all the clinical groups (ASD, ADHD, DS) show significant differences in relation to the CG, although the differences are higher in the case of the ASD group.
Discussion- 1)
Given that we introduced modifications in the original version of the CCC-2 to adapt it to the morphology, syntax, vocabulary and use of the Galician language, we analyzed the psychometric properties of the Galician version. Internal consistency values ranged between .64 and .95 in the different scales, which are very similar to those found by Bishop (2003) in the original version, who found values over .65. The reliability found for the overall scales (α=.91) is practically identical to that found for the Spanish version (α=.92) (Mendoza & Garzón, 2012). Therefore, the instrument shows pretty good reliability.
- 2)
The results obtained by the TD group in the GCC and the SIDC as well as in the different scales indicate a low level of linguistic problems. Although the mean score in the GCC is very low, it is not equal to zero, which indicates slight difficulties in the group of school age children with normal development (TD group). The positive values of the SIDC (we do not use scaled scores) indicate that these difficulties are of a pragmatic type, which coincides with the pattern found by Bishop (2003), Helland et al. (2009) and Mendoza and Garzón (2012) in English, Norwegian and Spanish children respectively. The consistency of the results found in different contexts points to a greater difficulty for the learning of pragmatic abilities, since the children have to learn what the adequate behavior is in function of the context, the interlocutor and the communicative intention, because no definite rules exist that regulate its use.
If attention is focused on the scores obtained in the 10 scales, the TD group obtains better proficiency in the structural abilities related with Syntax (B), Speech (A) and Coherence (D). These scales were also reported by Mendoza and Garzón (2012) as those with lower (better) mean scores. The greatest problems are observed in Interests (J) and Inappropriate Initiation (E), which indicates the tendency of school age children to focus on certain activities and topics of their own interest. In a similar way, Bishop (2003), Mendoza and Garzón (2012) and Philofsky et al. (2007) have reported the greatest problems of TD children in these two scales, which suggests these abilities are achieved later in the developmental process.
- 3)
The Galician CCC-2 has demonstrated its capacity to identify linguistic and communicative profiles for the different clinical groups.
In the case of ASD children pragmatic impairment clearly predominates. The greatest difficulties are observed in use of context (G), particularly the capacity to interpret figurative language. They also have problems to initiate conversations (E), with a predominance of repetitive initiations of topics of their own interests. The use of stereotyped language (F) is also a characteristic of ASD children. Difficulties in non-verbal communication (H) are evident in the inadequate use of gestures and facial expressions, as well as in the difficulties to understand others’ emotions. Restriction of interests (J) is particularly prominent in the selection of activities as well as in conversational topics. In the structural level, phonology (A) and syntax (B) seem to be strengths of the ASD group, in contrast with difficulties in semantics (C) and, particularly, coherence (D), because ASD children do not take into account the interlocutor's knowledge and use referents unknown to the interlocutor. School children with ASD differ from the CG children in all scales except speech (A). In this regard, Baixauli (2016) found differences in all the scales, and Helland et al. (2012) and Mendoza and Garzón (2012) found differences in all the scales with the exception of speech and syntax.
In the case of ADHD children pragmatic deficit predominates in relation to structural deficit, and differences in coherence (D) stand out, as they use unspecific referents and disorganized discourse. ADHD children have special difficulties in introducing topics (E), talking excessively and on topics of their own interests. They also show difficulties in the use of context (G), particularly in the understanding of nonliteral meanings. In the nonverbal communication scale (H), these children ignore the others’ interventions and focus their gaze on other tasks instead of on the interlocutor. In the semantics scale (C) ADHD children show limited precision in the selection of words. In this study, the ADHD group differs from the CG in scales C–H. Väisänen et al. (2014) found differences between ADHD and CG groups in all scales, while Helland et al. (2012) found differences in all scales except scale B, and Geurts and Embrechts (2008) found differences only in scales D, E, G, H, I, J. Our results, therefore are quite coincident with those found in other studies.
With DS children, a clear predominance of deficits in structure and content was observed. Phonological aspects of language (speech) (A) are those with the greatest impairment. Simplification of words and articulation problems are the most frequent. Difficulties in syntax (B) are also common, with the production of short and less complex utterances. The most relevant difficulties in coherence (D) are difficulties in specifying the referent, and the most relevant in semantics (3) is the scarce precision in choosing words. In pragmatics, the main impairments are found in the use of context (G), particularly the understanding of jokes. The group of DS children differs from the CG in all the scales, with the exception of interests (J). Although pragmatic abilities are a relative strength, they are also affected. Mendoza and Garzón found a similar pattern, with differences in all scales except scales I (social relations) and J (interests).
This study confirms the capacity of the Galician CCC-2 to identify if there are linguistic and communicative impairments or not through the GCC. Thus, the GCC scores are significantly higher in the clinical groups than in the CG. The capacity of the GCC index to identify linguistic impairments was repeatedly confirmed in other studies (Bishop, 2003; Geurts & Embrechts, 2008; Helland et al., 2009, 2012; Mendoza & Garzón, 2012; Väisänen et al., 2014). In the same vein, the GCC discriminates the profiles of the ADHD from the ASD and DS children, the first showing a lower alteration. However, the CCC-2 is unable to differentiate between the ASD and the DS children because both groups show a similarly high impairment level, as Mendoza and Garzón (2012) also found.
The utility of the SIDC index to identify different profiles of impairment with pragmatic impairment was also confirmed. The preponderance of structural impairments in DS children and of pragmatic impairments (high positive values) in ASD and ADHD was clearly established. ASD children show the greatest difficulties in pragmatics in relation to structural abilities, significantly differing from the other groups. The ADHD children show a higher impairment of pragmatic than of structural abilities as well, although the discrepancy between these abilities is lower in comparison to ASD children. This result agrees with other studies which also point to a similar profile of alteration in ASD and ADHD children, with slighter levels of impairment in the latter (Geurts, Broeders, & Nieuwland, 2010). The difference in the SIDC between the ADHD and the CG does not reach significance, however, which coincides with the findings of Helland et al. (2012). In any case, the absence of discrepancy between the ADHD group and the CG in the SIDC does not make any sense, since the CGs group does not show difficulties in the GCC. The SIDC discriminates among the three clinical groups with difficulties in the GCC and permits the discrimination between the DS in relation to the ADHD as well as to the ASD groups.
The SIDC does not directly compare the four structural scales and the four pragmatic scales. This index was introduced in the second edition of the CCC, substituting the GPI, because the latter did not differentiate among different profiles (Bishop, 2003). Our study confirms these results: the three clinical groups show significant differences among themselves in the SIDC, but the GPI does not discriminate between the DS and the ADHD. This latter result is because, although DS children have very high structural impairment, they also have pragmatic impairment, since pragmatic abilities depend in part on structural knowledge (Perkins, 2010).
The CCC-2 distinguishes different profiles characterized by a predominance of pragmatic alteration. Significant differences were found between the ASD and the ADHD in the main indexes of the instrument (GCC and SIDC). The children with ASD show higher impairments in scales F to J, which indicate not only higher pragmatic impairment, but also impairment in those aspects typically related with autism (difficulties in social relationships and restricted interests). These results agree with those found by Baixauli (2016) and, partially, with those found by Helland et al. (2012) and by Geurts and Embrechts (2008), who found differences in scales F and H, and G, H and I, respectively. The results we found are a combination of the findings of these last two studies, and are related to the diagnosis criteria of the ASD (pragmatic impairment, difficulties in social relationships and restricted interests).
When comparing the ASD and the ADHD groups with the CG, the ASD shows deficiencies in comparison with the CG in scales B, I and J, while the ADHD does not. This confirms the utility of scales I and J for the identification of school children with autism.
ConclusionsThe Galician CCC-2 demonstrated its capacity for screening school age children with linguistic and communicative difficulties, distinguishing different profiles of impairment.
This study also has practical implications for psychologists, speech therapists, educational counselors and other professionals working with ASD, ADHD and DS. The existence of communicative disorders in these groups is confirmed, suggesting that the evaluation of this aspect should be incorporated routinely to the process of assessment. This can contribute to a better adapt the intervention process, improving the effects of these interventions.
One limitation of this study is the reduced size of the sample, which recommends caution when generalizing the results found.
Linguistic abilities could also have been analyzed through other standardized tests in order to verify the findings.
Future research should incorporate other clinical groups (such as children with specific language impairment), and gather information from different informants (parents, teachers) to test cross-referee reliability.
The elaboration of normative scales for the Galician version (as well as for the Spanish version) should also be a topic for future research.
Conflict of interestsThe authors declare no conflict of interests.

