






Nursing homes are becoming increasingly important as end-of-life care facilities. However, many older adults want to stay in their homes as they age.
ObjectiveTo assess the feasibility of a deinstitutionalization process on selected institutionalized older adults who are willing to initiate the process.
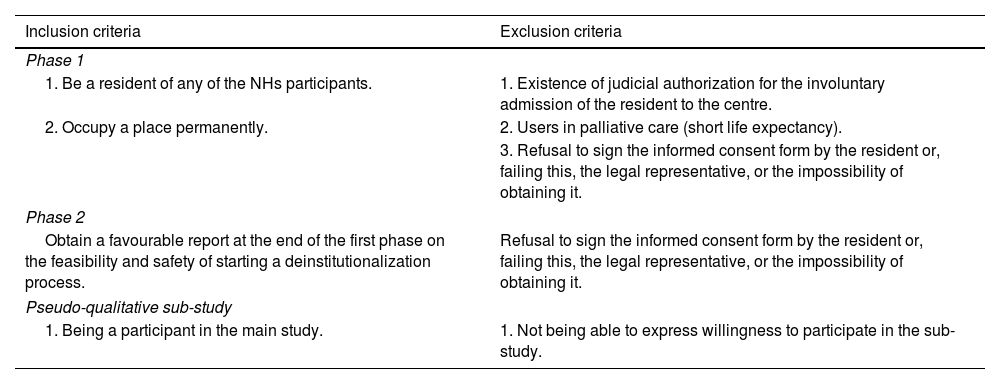
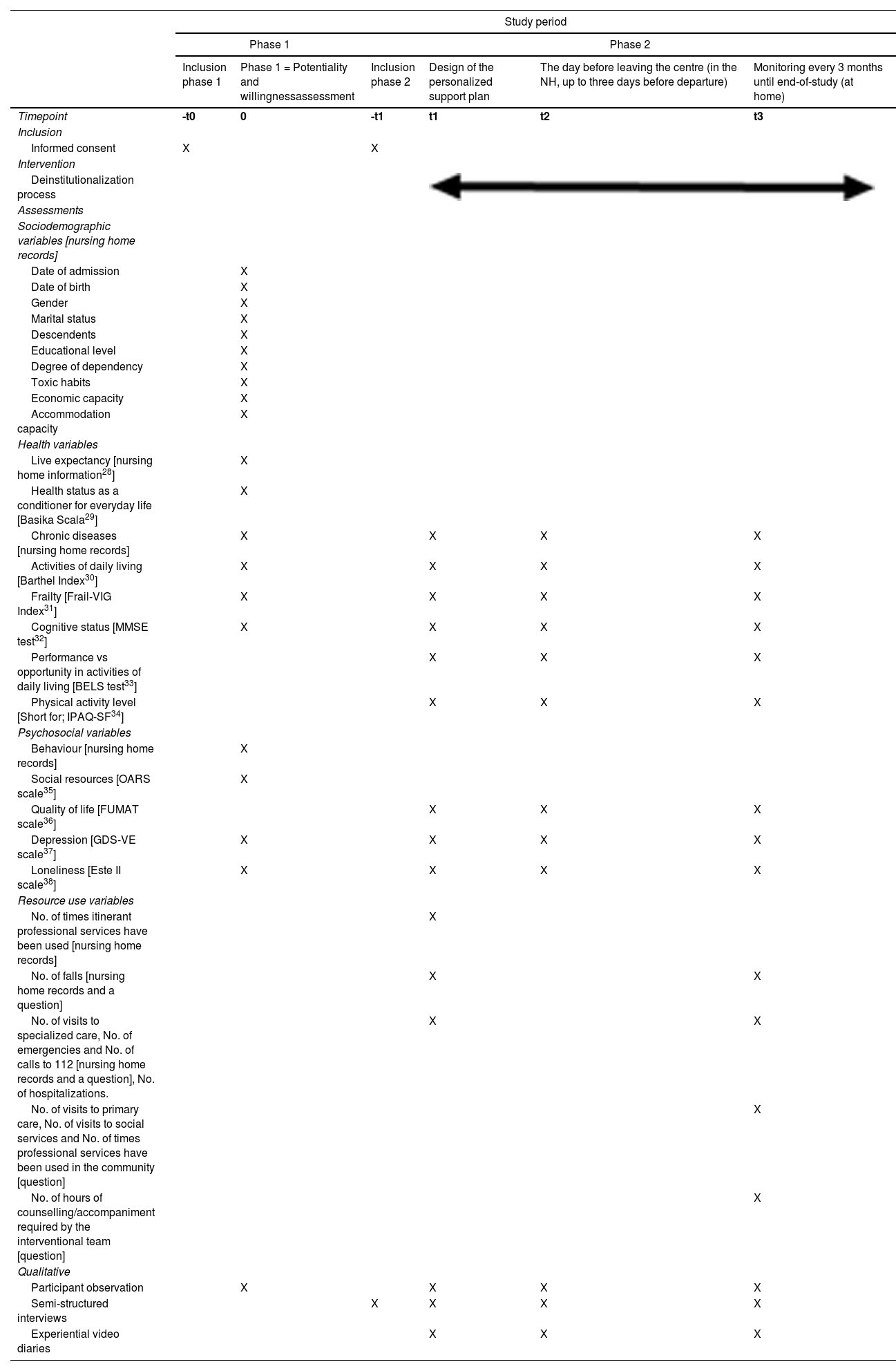
MethodsThis study, divided into two phases, will be carried out over 15 months on 241 residents living in two nursing homes in Navarra (Spain). The first phase has a cross-sectional design. We will identify the factors and covariates associated with feasibility and willingness to participate in a deinstitutionalization process by bivariate analysis, essential resources for the process and residents to participate in the process. The second phase has a complex interventional design to implement a deinstitutionalization process. An exploratory descriptive and comparative analysis will be carried out to characterize the participants, prescribed services and the impact deinstitutionalization intervention will have over time (quality of life will be the main outcome; secondary variables will be health, psychosocial, and resource use variables). This study will be accompanied by a pseudo-qualitative and emergent sub-study to identify barriers and facilitators concerning the implementation of this process and understand how intervention components and context influence the outcomes of the main study. Intervention components and the way the intervention is implemented will be of great relevance in the analysis.
DiscussionAlternatives to institutionalization with adapted accommodation and community support can allow people who wish to return to the community.
Trial registrationNCT05605392.
Las residencias de personas mayores cobran cada vez más importancia como centros de atención al final de la vida. Sin embargo, muchos adultos mayores desean permanecer en sus casas mientras envejecen.
ObjetivoSe pretende evaluar la viabilidad de un proceso de desinstitucionalización en adultos mayores seleccionados que viven en las residencias y que expresen la voluntad para iniciar el proceso.
MétodosEste estudio, dividido en dos fases, se llevará a cabo durante 15 meses en 241 sujetos que viven en dos residencias de personas mayores en Navarra (España). La primera fase tiene un diseño transversal en donde se identificarán los factores y covariables asociadas a la viabilidad y voluntad para participar en un proceso de desinstitucionalización a través de un análisis bivariante, los recursos imprescindibles para el proceso y los residentes que quieran participar en él. La segunda fase tiene un diseño de intervención compleja en la que se implementa un proceso de desinstitucionalización. Se realizará un análisis exploratorio descriptivo y comparativo para caracterizar a los participantes, los servicios prescritos y el efecto de la intervención de desinstitucionalización a lo largo del tiempo (la calidad de vida será la variable principal; las secundarias serán las referentes a la salud, las psicosociales y de uso de recursos). Este estudio irá acompañado de un subestudio pseudocualitativo y emergente para identificar las barreras y los elementos facilitadores relativos a la implementación de este proceso y comprender cómo los componentes de la intervención y el contexto influyen en los resultados del estudio principal. Los componentes de la intervención y su ejecución serán de gran relevancia en el análisis.
DiscusiónLas alternativas a la institucionalización con viviendas adaptadas y apoyos comunitarios pueden permitir a las personas que así lo desean el retorno a la comunidad.
Registro del estudioNCT05605392.
