













Tooth-bone discrepancy, or crowding in the lower arch, is traditionally corrected by removing first or second premolars; the extraction of a lower incisor is an uncommon approach but presents another treatment alternative. Treatment goal: to present the case report of a patient who was given this alternative treatment. The patient had 15 years 4 months of age. The intraoral analysis revealed a normodivergent skeletal class I with bilateral molar class I, bilateral canine class I, decreased overbite, and increased overjet. She had lower moderate and mild upper crowding as well as a habit of digital suction. Treatment time was one year and four months.
La discrepancia de longitud, o el apiñamiento en la arcada inferior, tradicionalmente se corrige por medio de la extracción de primeros o segundos premolares; la extracción de un incisivo inferior es un enfoque poco común pero es otra alternativa sobre todo en el arco mandibular.
ObjetivoPresentar el tratamiento de una paciente de ortodoncia con estas características, a la cual se le da este tratamiento, de 15 años cuatro meses de edad. Al análisis intraoral, es clase I esquelética, normodivergente, con clase I molar bilateral, clase I canina bilateral, con el overbite disminuido, y overjet aumentado, tiene apiñamiento moderado inferior, y leve superior, presenta hábito de succión digital. El tiempo que duró el tratamiento fue de un año cuatro meses.
Jackson describes a case in which two lower incisors were extracted at different times to solve mandibular crowding.1 Since then, a series of clinical cases have been treated with this option.2,3 Authors such as: Canut, Bahreman, have listed specific criteria for the removal of a mandibular incisor such as: permanent dentition, minimum growth potential, class I molar relationship, a harmonious soft tissue profile, minimal to moderate overbite, little or no crowding in the upper arch, a Bolton discrepancy.2,4 Agood diagnosis is highly recommended with this kind of treatment.5,6 On the other hand, the removal of a mandibular incisor has several advantages over premolar extractions. First, treatment time may be reduced especially if the crowding is limited only to the anterior segment.5 Second, it offers a stable result in the anterior region because the expansion is not necessary and canine width is not altered.3 Finally, since it requires little retraction in comparison with the therapy of premolars removal, the anteroposterior position of the lower incisors is not changed which maintains a harmonious profile.4 This treatment also offers us a series of disadvantages: if there is a Bolton discrepancy, space closure will result in a greater overjet, in addition to altering the interproximal papillae, which can cause black triangles.7
CASE REPORTDuring clinical evaluation, the patient reported as reason for consultation «I have crooked teeth». In the initial radiographic studies, the lateral head film showed normodivergency and a mild proclination of the upper and lower incisors (Figure 1). In the panoramic radiograph no pathological data were noted; the patient had 28 permanent teeth, formation of the lower third molars and agenesis of the upper (Figure 2).
Initial records

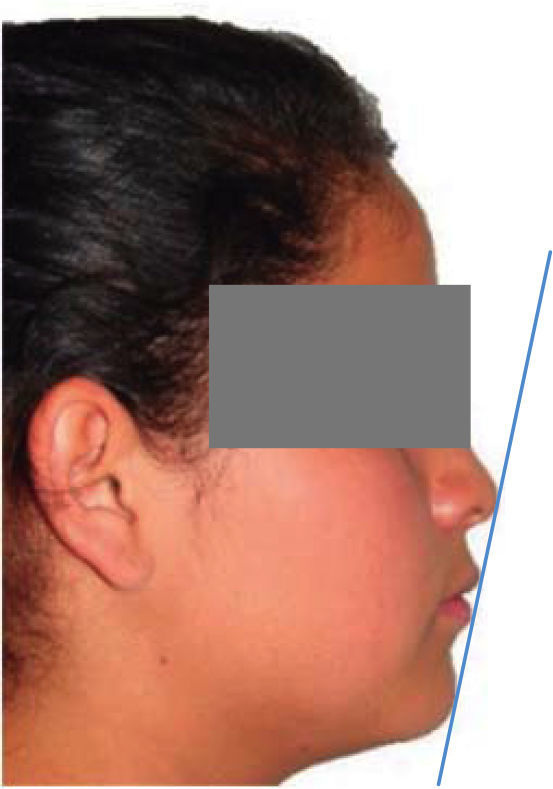
In the facial analysis of the photographs of the patient, the profile was assessed, and it was found to be adequate. The dental midline was diverted 0.5mm to the right in relation to the facial; facial fifths and thirds were proportional. All these were meaningful data in decision-making for the treatment plan (Figure 3), facial midline (Figure 4), and aesthetic line of Ricketts, E line.


When performing the intraoral analysis the objectives posed to cover were observed: elimination of upper mild and lower moderate anterior crowding, to correct the lack of coincidence between the upper and lower dental midlines. The patient was in canine and molar class I, which would be maintained. Another aspect to highlight was the 6mm overjet caused by the habit and the upper and lower triangular arch form intraoral front (Figure 5), in the intraoral photographs, right, and left side (Figures 6 and 7).
Treatment plan


To eradicate the habit of digital suction, a palatal grid was placed for two months. Afterwards, the appliance was withdrawn and Roth prescription brackets were placed giving instructions for the removal of the lower right lateral incisor.
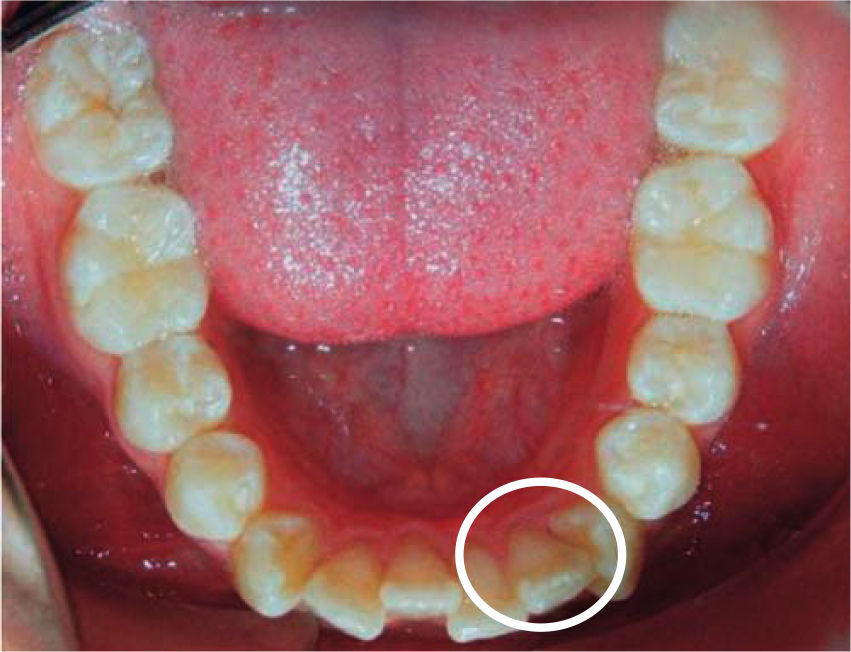
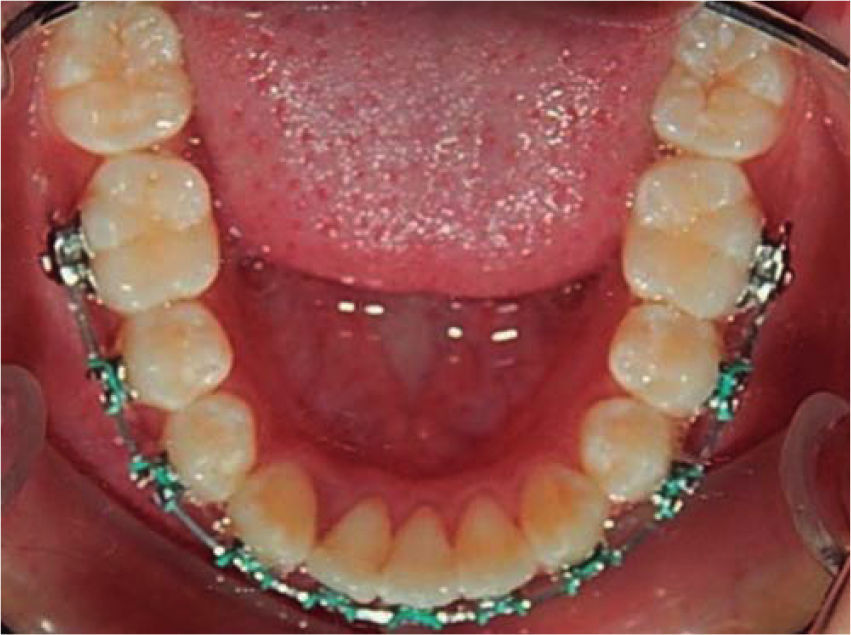
Alignment and leveling was begun on both the upper and lower arches, with stripping sessions in the upper arch and closure of the extraction space in the lower arch. After the alignment and leveling (Figure 8), lower occlusal photograph indicating the tooth to be extracted, in the lower occlusal image of progress after space closure (Figure 9).
Final records

The objectives were met: the E line was improved, bilateral molar and canine class I were maintained, a better arch form on both the upper and lower arch was achieved and therefore, a normal overjet and overbite as well. Good intercuspation was obtained, as it may be observed in the intraoral photographs: final front view (Figures 10 to 12), in the right and left side.



In the final lower occlusal photograph, the fixed retainer from canine to canine may be observed (Figure 13).
RESULTS
As it may be observed in this case the set objectives were achieved. The patient ended with excellent aesthetics and a harmonious smile. Total treatment time was one year and four months. A comparison between the initial and final smile is shown in figure 14. Although the extraction of a lower incisor is not a very common treatment, it may provide an excellent result if a good diagnosis is done.
DISCUSSION
Canut2 points out the aspects to be considered for this type of treatment, which were taken as reference for the procedure: X-rays, models and intra and extra oral photographs, were obtained in order to follow those guidelines. Uribe8 suggested that the extraction of a mandibular incisor is the most appropriate treatment in patients who do not require modifications in the anteroposterior buccal segments, as was our patient, and for whom this option was ideal since one of the goals was to maintain that anteroposterior relationship. On the other hand Faerovig7 points out that a great disadvantage with this treatment lies in the interproximal papillae, which may be flattened and may lead to the development of «black triangles». This was the reason why this case was handled with extreme care, in order to obtain optimal aesthetics.
CONCLUSIONSThe extraction of a mandibular incisor is an effective treatment in patients who meet the requirements established by the literature and who are aware of it in order to obtain excellent results, since a wrong diagnosis can lead to unwanted side effects and will directly affect the aesthetics of the patient.