




Aplicar 3instrumentos de evaluación de enfermedad avanzada en ancianos ingresados en un centro sociosanitario y evaluar su relación con la mortalidad.
MétodosSe aplicaron los instrumentos NECPAL, índice PROFUND e índice de comorbilidad de Charlson a 87 pacientes.
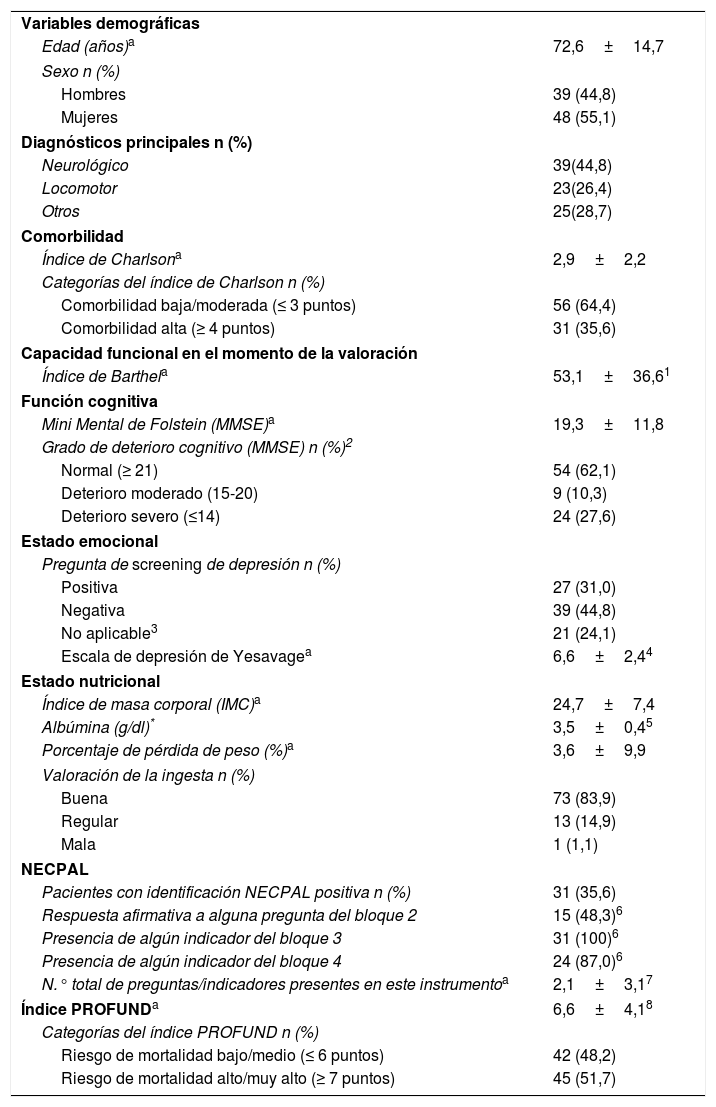
ResultadosEl instrumento NECPAL identificó a 31 pacientes (35,6%) en situación de necesidad de atención paliativa; según el índice PROFUND, 45 (54,7%) tenían riesgo alto/muy alto de mortalidad (≥7 puntos) y según el índice de Charlson, 31 (35,6%) tenían carga de morbilidad alta (≥4 puntos).
Pacientes NECPAL positivos: el 80,5% tenían puntuación ≥7 en índice PROFUND y 48,3% un Charlson ≥ 4; dichas proporciones fueron 34,4 y 28,5% en los NECPAL negativos (p<0,001 y p≤0,06, respectivamente).
Correlaciones entre los 3instrumentos: cuantitativas (Spearman): número de respuestas NECPAL con PROFUND (r=0,57; p<0,001); con Charlson (r=0,214; p=0,047) y entre PROFUND y Charlson (r=0,157; p=0,148).
Cualitativas (kappa) NECPAL (positivo/negativo) con PROFUND (corte 6/7) (0,40; p<0,001), con Charlson (corte 3/4) (0,19; p=0,080) y entre PROFUND y Charlson (0,08; p=0,399).
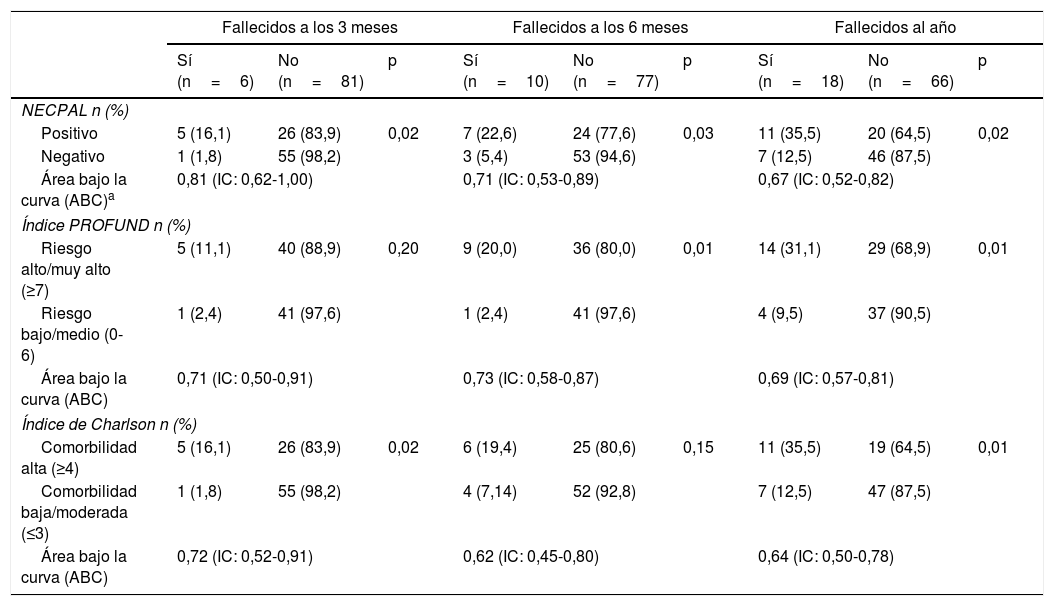
Predicción de mortalidad (área bajo la curva): NECPAL 3 meses 0,81 (IC: 0,62-1,00); 6 meses 0,71 (IC: 0,53-0,89) y 12 meses 0,67 (IC: 0,52-0,82). PROFUND 3 meses 0,71 (IC: 0,50-0,91); 6 meses 0,73 (IC: 0,58-0,87) y 12 meses 0,69 (IC: 0,57-0,81). Charlson 3 meses 0,72 (IC: 0,52-0,91); 6 meses 0,62 (IC: 0,45-0,80) y 12 meses 0,64 (IC: 0,50-0,78).
ConclusionesLos 3instrumentos se relacionaron de forma significativa con una mayor mortalidad. La concordancia entre los resultados de los distintos instrumentos fue baja.
To apply 3advanced chronic disease evaluation tools in elderly patients admitted to an intermediate and long-term care centre, and evaluate its relationship with mortality.
MethodsThe NECPAL tool, PROFUND prognostic index, and Charlson comorbidity index were applied to 87 patients.
ResultsThe NECPAL tool identified 31 patients (35.6%) in need of palliative care, and according to the PROFUND index, 45 (54.7%) had high/very high risk of mortality (≥7 points), and according to Charlson index, 31 (35.6%) had high comorbidity (≥4 points).
Of the NECPAL positive patients, 80.5% had a PROFUND index score ≥7, and 48.3% a Charlson index ≥ 4. These percentages were 34.4% and 28.5% in negative NECPAL patients (P<.001 and P≤.06, respectively).
Correlations between the 3tools: quantitative (Spearman) number of responses in NECPAL with PROFUND (r=.57; P<.001); with Charlson (r=.214; P<.047) and between PROFUND and Charlson (r=.157; P=.148). Qualitative (kappa) NECPAL (positive/negative) with PROFUND (cut-off 6/7) (0.40; P<.001), and Charlson (cut-off 3/4) (0.19; P=.080) and between PROFUND and Charlson (0.08; P=.399).
Mortality prediction (area under the curve): NECPAL 3 months 0.81 (95% CI: 0.62-1.00); 6 months 0.71 (95% CI: 0.53-0.89) and 12 months 0.67 (95% CI: 0.52-0.82). PROFUND 3 months 0.71 (95% CI: 0.50-0.91); 6 months 0.73 (95% CI: 0.58-0.87), and 12 months 0.69 (95% CI: 0.57-0.81). Charlson 3 months 0.72 (95% CI: 0.52-0.91); 6 months 0.62 (95% CI: 0.45-0.80), and 12 months 0.64 (95% CI: 0.50-0.78).
ConclusionsThe 3tools were significantly associated with high mortality. A low concordance was found between the results of the different tools.
Artículo

Comprando el artículo el PDF del mismo podrá ser descargado
Precio 19,34 €
Comprar ahora
