


Orbital fractures are common in facial and orbital trauma, with orbital floor and medial wall commonly affected.
ObjectiveThe aim of this study was to evaluate the outcomes of endoscopic repair of medial and inferior orbital wall fracture.
DesignA case series with chart review (observational study), the study was conducted in academic tertiary care medical centers.
MethodsNine patients underwent endoscopic repair of medial and inferior orbital wall fracture between the years May 2013 and August 2016.
ResultsSignificant changes in preoperative eye lid ecchymosis, diplopia, enophathalmus, emphysema and facial hypoesthesia. Other postoperative complication of nasal endoscopy (blandness, hemorrhage, infection, exposure, and extrusion of the graft) were absent in all patients.
ConclusionsEndoscopic repair of medial and inferior orbital wall fracture using porous polyethylene was an easy and fast approach with satisfactory outcomes with avoiding the external incision.
Las fracturas orbitales son frecuentes en los traumatismos faciales y orbitales, en los que frecuentemente se ve afectada la pared orbital media e inferior.
ObjetivoEl objetivo de este estudio fue evaluar los resultados de la reparación endoscópica de la fractura de la pared orbital media e inferior.
DiseñoEstudio de serie de casos con cuadro de revisión (estudio observacional), realizado en centros médicos de cuidados terciarios académicos.
MétodosNueve pacientes sometidos a reparación endoscópica de fractura de pared orbital media e inferior entre mayo de 2013 y agosto de 2016.
ResultadosCambios significativos de equimosis preoperatoria del párpado, diplopía, exoftalmo, enfisema e hipoestesia. No se observaron en los pacientes otras complicaciones postoperatorias de la endoscopia nasal (blandura, hemorragia, infección, exposición y extrusión del injerto).
ConclusionesLa reparación endoscópica de fractura de la pared orbital media e inferior con polietileno poroso resultó una técnica fácil y rápida que evitó la incisión externa.
Orbital fractures are common in facial and orbital trauma, with orbital floor and medial wall commonly affected. The fractures may be either direct or indirect.1 The main symptom is diplopia and sign is the ocular motility which occurs in the direction of the antagonist muscle due to restriction of the entrapped muscle.2 Moreover, the muscle edema, muscle fibrosis, hemorrhage, and motor nerve paralysis are also causes of the limitation.3 The aim of the surgical repair is restoring the traumatized wall, so preventing herniation of the contents of the globe into the maxillary sinus and causes complication.4 Hence, the aim of this study was to evaluate the outcomes of endoscopic repair of medial and inferior orbital wall fracture using porous polyethylene.
MethodsThe study was conducted between May 2013 and August 2016. A case series with chart review (observational study) over 4 years. The study was conducted in academic tertiary care medical centers (Department of ENT and Ophthalmology in Al-Azhar University Hospitals and, Ain-Shams University hospitals in Cairo – Egypt).
Our patients’ inclusion criteria were: 1 – orbital fracture (medial and inferior orbital wall fracture) only, 2 – adult (≥18years old), 3 – patient with diplopia (with no response to medical treatment after 2 week or with radiological evidence of muscle or soft tissue entrapment) and 4 – the defect of the floor ≤20mm. The Exclusion criteria included one or more of the following: 1 – other orbital fracture rather than medial and inferior orbital wall fracture, 2 – medial and inferior orbital wall fracture combined with other facial fractures, 3 – lager bone defect of the floor (≥20mm).
According to the time of operation; we wait at least 2 week for edema subsiding with medical treatment in this period, our indications for urgent interference: diplopia with radiological evidence of muscle or soft tissue entrapment and rapid deterioration of vision, which have no happened in our patient.
All procedures performed in studies involving human participants were in accordance with the ethical standards of our universities and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All patients or their legal guardians signed a preoperative consent for the operation and the conduct of research, to know their rights and duties. The study work was approved by our university ethical committee.
Total of nine patients reported with history of accident having facial trauma associated with orbital wall disruption were included in the study. Out of nine patients, seven were male and two were female.
Patient assessmentPre- and post-operative clinical assessment of the patients by ophthalmologist and endoscopic nasal assessment was done by the rhinologist. In addition, the patients were evaluated by computed tomography (CT) scan paranasal sinuses (PNS) to see the size and site of the fracture. All of the pre- and post-operative details were recorded for further analysis of the data as in Table 1.
Patients chart review show (symptoms and signs in the pre and post- operative periods).
| Items | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | ≠ age (Y.M) | ≠ area | ≠ sex | ≠ the fractured bone | Preoperative eyelid ecchymosis | Postoperative eyelid ecchymosis | Preoperative diplopia | Postoperative diplopia | Preoperative enophathalmus | Postoperative enophathalmus | Preoperative emphysema | Postoperative emphysema | Preoperative hypoesthesia | Postoperative hypoesthesia | Other postoperative complication | HESS score postoperativea | HESS score preoperativea | ±Preoperative diplopia chart | ±Postoperative diplopia chart |
| 1 | 45.2 | R | M | M&I | + | − | + | − | − | − | + | − | + | − | − | 89 | 2114 | 1 | 2 |
| 2 | 36.5 | R | M | I | + | − | + | − | − | − | − | − | − | − | − | 78 | 1245 | 0 | 3 |
| 3 | 53.8 | R | M | I | + | − | + | − | − | − | − | − | − | − | − | 63 | 1752 | 2 | 3 |
| 4 | 56.4 | R | M | I | + | − | + | − | + | − | − | − | + | − | − | 92 | 1113 | 1 | 3 |
| 5 | 34.2 | U | M | M | + | − | + | − | − | − | + | − | − | − | − | 51 | 651 | 1 | 2 |
| 6 | 24.9 | R | F | I | + | − | + | − | − | − | + | − | − | − | − | 63 | 736 | 0 | 2 |
| 7 | 25.2 | R | F | M | − | − | + | − | − | − | _ | − | − | − | − | 67 | 1823 | 1 | 2 |
| 8 | 36.5 | U | M | M&I | + | − | + | + | + | + | + | − | + | + | − | 1521 | 2096 | 0 | 0 |
| 9 | 43.6 | U | M | M&I | + | − | + | − | + | − | − | − | − | − | − | 115 | 1981 | 2 | 3 |
Notes: ≠ area: U=urban, R=rural; sex: M=male, F=female; the fractured bone: M=medial, I=inferior (floor).
The operation was performed under general anesthesia with the patient in a supine position. The uncinate is resected with 3–4mm of uncinate is left intact superiorly to prevent frontal recess stenosis. This exposed the natural ostium of the maxillary sinus and an antrostomy is performed in a posterior and inferior direction. The size and fracture configuration are defined using a 30°, 4-mm endoscope.
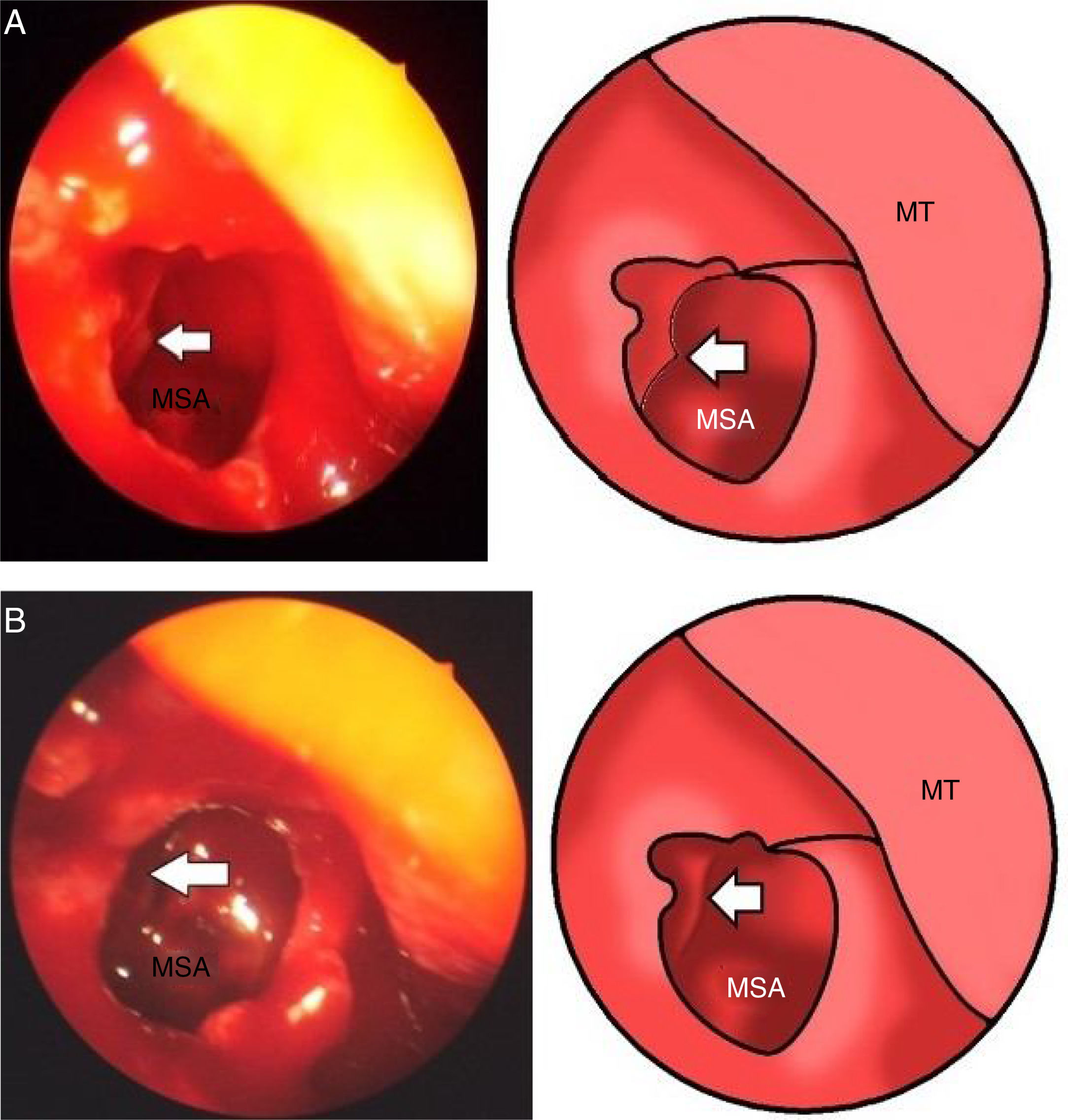
The purpose of the maxillary antrostomy is to explore the floor of orbit and to prevent the potential development of chronic maxillary sinusitis due to traumatic obstruction of the sinus ostia (Fig. 1A). Once the fracture of the floor is noted the reduction was done (Fig. 1B).
 Operative endoscopic view show maxillary sinus antrostomy (MSA) explored the floor of orbit and the fracture of the floor is noted (arrow), and middle turbinate (MT). (B) Operative endoscopic view show maxillary sinus antrostomy (MSA), the reduction of fracture was done (arrow), and middle turbinate (MT).")
(A) Operative endoscopic view show maxillary sinus antrostomy (MSA) explored the floor of orbit and the fracture of the floor is noted (arrow), and middle turbinate (MT). (B) Operative endoscopic view show maxillary sinus antrostomy (MSA), the reduction of fracture was done (arrow), and middle turbinate (MT).
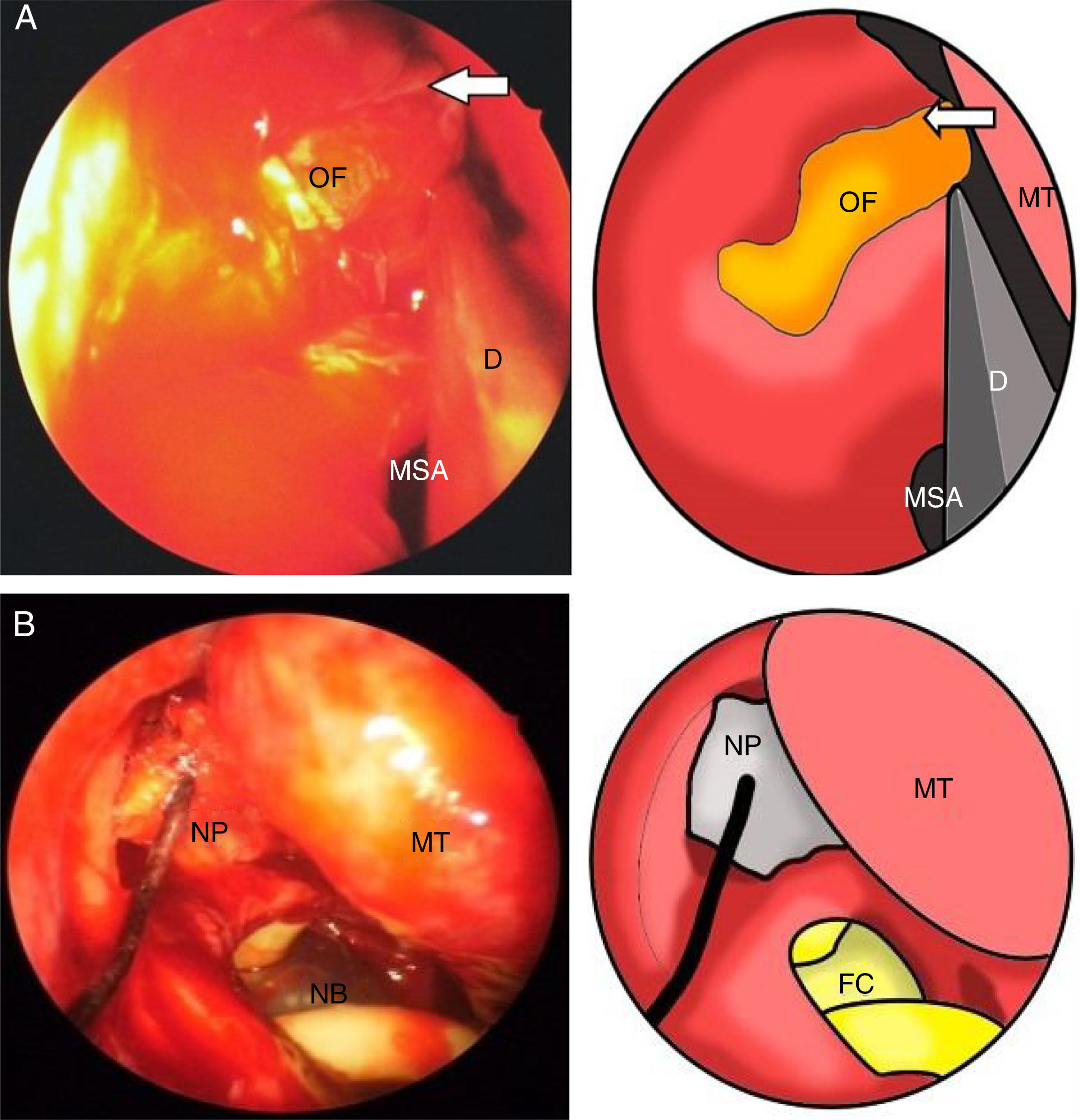
The bone fragments at the site of ethmoidal bulla were then removed to expose the lamina papyracea defect (Fig. 2A). The orbital contents are reduced and held in place with a retractor with adequate reduction.
 Operative endoscopic view show the bone fragments entered medially and removed to expose the lamina papyracea defect (arrow), MSA=maxillary sinus antrostomy, D=dissector. (B) Operative endoscopic view show following to the Medpore® implantation and nasal pack (NP) inserted and a Foley's catheter (FC/NB) size 12 was inserted in the maxillary sinus to support the floor, maxillary sinus ostium (MSO), middle turbinate (MT).")
(A) Operative endoscopic view show the bone fragments entered medially and removed to expose the lamina papyracea defect (arrow), MSA=maxillary sinus antrostomy, D=dissector. (B) Operative endoscopic view show following to the Medpore® implantation and nasal pack (NP) inserted and a Foley's catheter (FC/NB) size 12 was inserted in the maxillary sinus to support the floor, maxillary sinus ostium (MSO), middle turbinate (MT).
The orbital implant which is porous polyethylene (Medpore®, 0.85mm, Porex Surgical Products); is then cut to the appropriate shape and size to cover the orbital floor and lamina papyracea defect. The implant was introduced through the endoscopes for visualization. Following to that implantation an absorbable (MeroPack®-Medtronic) nasal pack was inserted and a Foley's catheter size 12 was inserted in the maxillary sinus to support the floor (Fig. 2B).
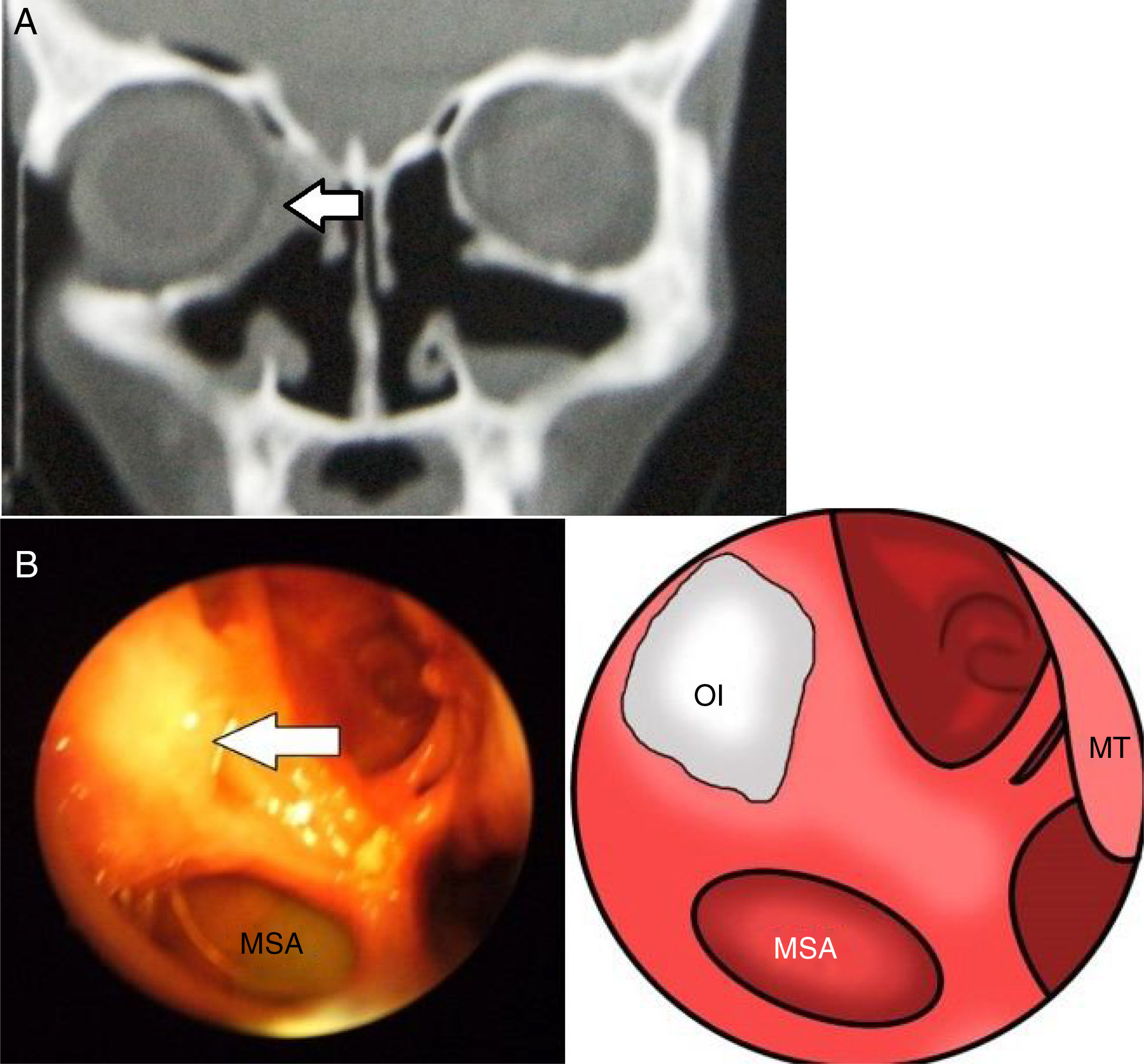
Post-operatively, nasal saline irrigations are started and the Foley's catheter removed after 2 weeks, with CT scans PNS after one month, as shown in (Fig. 3A and B). Visual acuity, range of motion, diplopia chart, HESS score and Hertel measurements are carefully followed in the postoperative period.
 Postoperative CT scan show the reconstruction of both medial and inferior wall of orbit (Medpore®) implantation is not radiopaque (the arrow). (B) Postoperative endoscopic view show maxillary sinus antrostomy (MSA) and the reconstruction of both medial and inferior wall of orbit with (Medpore®) implantation (the arrow).")
(A) Postoperative CT scan show the reconstruction of both medial and inferior wall of orbit (Medpore®) implantation is not radiopaque (the arrow). (B) Postoperative endoscopic view show maxillary sinus antrostomy (MSA) and the reconstruction of both medial and inferior wall of orbit with (Medpore®) implantation (the arrow).
Nine patients presented with medial orbital wall, floor or both fracture. The average follow-up in this study was 18 months (range 12–28 months). The age of patients ranged from 24.2 to 63.5 years and mean±SD of age (40.5±13.157) years old. Signs and symptoms of patients were recorded to Table 1. The cause of blowout fracture was motor vehicle accident in 7 (77.7%) patients and work-related incidents in two (22.2%) cases, sports injuries in one (11.1%) cases.
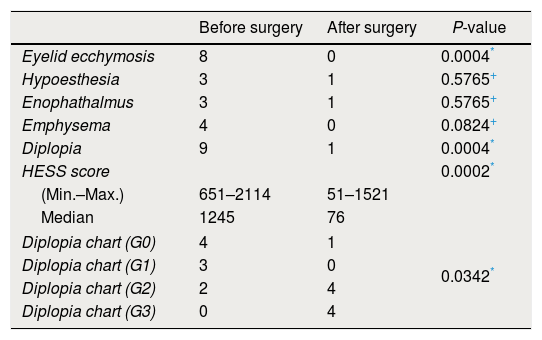
Regarding the type of fracture; the medial wall and the inferior wall (floor) was involved 3 (33.3%) patients, the inferior wall (floor) only alone was involved 4 (44.4%) patients and the medial wall was involved 2 (22.2%) patients. By analysis of data as described in Table 2 we found that: 1 – preoperative eye lid ecchymosis was in 8 (88.8%) patients while postoperative eye lid ecchymosis was absent in all patients (0%). 2 – Preoperative enophathalmus was in 3 patients (33.3%) while postoperative enophathalmus was in one patient (11.1%). 3 – Preoperative emphysema was in 4 patients (44.4%) while postoperative emphysema was absent in all patients (0%). 4 – Preoperative facial hypoesthesia was in 3 patients (33.3%) while postoperative facial hypoesthesia was in one patient (11.1%). 5 – Preoperative diplopia was in all patients (100%) while postoperative diplopia was in one patient (11.1%). 6 – By using a HESS scoring for diplopia (objective method) we found the range of diplopia score was from Min. 651 to Max. 2114 (median=1245) and three weeks after operation the range of diplopia score was from Min. 51 to Max. 1521 (median=76) with significant changes (P-value=0.0002) between the pre- and post-operative scoring. 7 – Moreover, by using a diplopia chart (subjective method) we found with significant changes (P-value=0.0342) between the pre- and post-operative score.
Changes between the preoperative and postoperative (1 year) clinical finding.
| Before surgery | After surgery | P-value | |
|---|---|---|---|
| Eyelid ecchymosis | 8 | 0 | 0.0004* |
| Hypoesthesia | 3 | 1 | 0.5765+ |
| Enophathalmus | 3 | 1 | 0.5765+ |
| Emphysema | 4 | 0 | 0.0824+ |
| Diplopia | 9 | 1 | 0.0004* |
| HESS score | 0.0002* | ||
| (Min.–Max.) | 651–2114 | 51–1521 | |
| Median | 1245 | 76 | |
| Diplopia chart (G0) | 4 | 1 | 0.0342* |
| Diplopia chart (G1) | 3 | 0 | |
| Diplopia chart (G2) | 2 | 4 | |
| Diplopia chart (G3) | 0 | 4 | |
Other postoperative complication (blindness, hemorrhage, infection, exposure, pyogenic granuloma formation, postoperative mydriasis, epiphora, worsening diplopia, and lid malpositioning and extrusion of the graft) were absent in all patients (0%).
DiscussionSmith and Regan proposed the mechanism of fracture; as compression of the globe increases the hydraulic pressure then it exerts on the weak orbital wall (floor and medial wall), which if sufficient fracture occurs. The timing of repair of indirect orbital floor fractures has been the subject of numerous reports.5
Dal Canto and Linberg found that no statistical difference in postoperative binocular diplopia when comparison of early versus late fracture repair was carried out.6 Lelli et al. stated that, the emergent conditions that require urgent surgical repair are: (1) diplopia with radiological evidence of muscle or soft tissue entrapment and (2) “white-eyed” fractures in patients less than 18 years of age with vertical limitation of eye movement and radiological.7 Regarding to our research wait at least two week for edema subsiding with medical treatment in this period, our indications for urgent interference were the indication stated by Lelli et al. and rapid deterioration of vision, which have no happened in our patient.
Ilankovan et al. reported the use calvarial bone.8 Also, Nishiike et al. reported the use of antral bone,9 and endochondral bone grafts was used by Ezzat et al.10 It is known that porous polyethylene has high biocompatibility with human host tissues, as many clinical application cases have been reported in medical literature. Porous polyethylene is enough inert and tolerative against a host defense system, especially enzyme and immune system of host, so porous polyethylene would not be degraded easily in a physiologic environment. The multi-porous structure of Medpor provides a settling space to new bone tissue cells as a good regenerating environment tube integrated with host bone tissue. The porous structure allows prominent vascularization and connective tissue in growth among the space too. However, the disadvantages of porous polyethylene were; not radiopaque (not visible on postoperative images), therefore we depend mainly on the postoperative endoscopic evaluation beside the CT scan. Lack of rigidity is also a problem specially when a very thin wafer of porous polyethylene is used therefore we used the 0.85mm thickness. Ceylan et al. described using porous polyethylene (Medpore®) implant with no complication related to use of it.11 Regarding our research we also fund that using porous polyethylene implant has no complication related to use of it. Moreover Jin et al. reported using either alloplastic, autologous or both materials in the orbital wall repair.12
Lee and Nunery used titanium implants in patients who presented with diplopia and/or cicatricial eyelid retraction after repair of orbital fracture. In 10 patients; 6 had cicatricial eyelid retraction and 9 patients had extraocular motility restriction and resulting diplopia.13 However in our research we found the preoperative diplopia was in all patients subjectively by diplopia chart and objectively by HESS scores.14 The range of HESS score was from 651 to 2114 and 3 weeks after operation; the range of diplopia score was from 51 to 115 except one patient and his HESS score was 1521, and with diplopia chart a significant changes (P-value=0.0342) was found between the pre- and post-operative score. The enopthalmous was in the same patient with diplopia and the facial (11.1%). This also correlated with Balaji who stated that of the 69 RD cases (after a primary surgery) surgically intervened, 8 cases (11.6%) had RD even after the secondary surgery.15 In our research we did not fund any of this complication as shown in Table 1. Hence best advantage of endoscopic repair is lesser muscle trauma during floor or medial wall reconstruction.
Moreover, we found that one of the advantage of the use of endoscopy was to: 1 – Visualize the transition zone between the medial orbital wall and the orbital floor which is difficult to be visualized intraoperatively in sub-conjunctival approach. 2 – Confirm that the implant in its optimal location, through the direct visualization of its place. Whoever, the limitation of the use of endoscopy was; it is not easily to repair of floor fracture larger than 20mm, because the difficulty of accessibility to insert the porous polyethylene.
ConclusionEndoscopic repair of medial and inferior orbital wall fracture using porous polyethylene was an easy and fast approach with satisfactory outcomes with avoiding the external incision.
Ethical approvalAll procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consentInformed consent was obtained from all individual participants included in the study.
Conflict of interestThe authors declare that there are no conflicts of interest.
