


To evaluate the correlation of different hematological parameters in lupus patients with SLE disease activity index (SLEDAI), the Systemic Lupus International Collaboration Clinics/American College of Rheumatology Damage Index (SLICC/ACR DI), and some laboratory data related to kidney functions in active patients with nephritis.
Material and methods80 inactive SLE patients (SLEDAI score<10 points), and 80 active patients (SLEDAI≥10 points) were enrolled in this study. All patients underwent full medical history taking, clinical evaluation including calculation of SLEDAI and SLICC/ACR DI scores, and laboratory investigations including complete blood count. The two groups were compared regarding different disease parameters. Correlations of some hematological parameters with SLEDAI, SLICC/ACR DI scores and some laboratory data related to kidney function in patients with nephritis were made.
ResultsThe active group showed statistically significantly higher mean NLR (P=0.000), NC3R (P=0.000), MLR (P=0.000), PLR (P=0.000), and RDW (P=0.001), and statistically significantly lower mean MPV (P=0.002). The mean MLR (P=0.018) and PLR (P=0.005) were statistically significantly higher in the active patients with nephritis. For both groups, there were no significant correlations between studied parameters and SLEDAI or SLICC/ACR DI, except with NC3R values in the active group which were associated with SLEDAI (r=.221, P=0.049).
ConclusionThe hematological parameters in SLE have promising potential clinical application as a novel activity marker, especially in patients with nephritis.
Evaluar la correlación de diferentes parámetros hematológicos en pacientes con lupus con el índice de actividad de la enfermedad del LES (SLEDAI), el Systemic Lupus International Collaboration Clinics/American College of Rheumatology Damage Index (SLICC/ACR DI y algunos datos de laboratorio relacionados con la función renal en pacientes activos con nefritis.
Material y métodosOchenta pacientes con LES inactivos (puntuación SLEDAI < 10 puntos) y 80 pacientes activos (SLEDAI ≥ 10 puntos) se inscribieron en este estudio. Todos los pacientes se sometieron a una historia clínica completa, evaluación clínica, incluido el cálculo de las puntuaciones SLEDAI y SLICC/ACR DI, e investigaciones de laboratorio, incluido un hemograma completo. Se hizo una comparación entre los dos grupos con respecto a diferentes parámetros de la enfermedad. Se realizaron correlaciones de algunos parámetros hematológicos con las puntuaciones SLEDAI, SLICC/ACR DI y algunos datos de laboratorio relacionados con la función renal en pacientes con nefritis.
ResultadosEl grupo activo mostró una media estadísticamente significativamente más alta de NLR (P=0,000), NC3R (P=0,000), MLR (P=0,000), PLR (P=0,000) y RDW (P=0,001) y una media estadísticamente significativamente más baja de VPM (P=0,002). La media de MLR (P=0,018) y PLR (P=0,005) fue significativamente mayor desde el punto de vista estadístico en los pacientes activos con nefritis. Para ambos grupos, no hubo correlaciones significativas entre los parámetros estudiados y SLEDAI o SLICC/ACR DI, excepto con los valores de NC3R en el grupo activo que se asoció con SLEDAI (r=0,221, P=0,049).
ConclusiónLos parámetros hematológicos en el LES tienen una aplicación clínica potencial prometedora como marcador de actividad novedoso, especialmente en pacientes con nefritis.
Systemic lupus erythematosus (SLE) is a chronic autoimmune inflammatory disease that affects multiple organs and body systems with various forms of clinical presentation, course, and subsequent organ damage.1
Hematological manifestations are one of the most common findings in patients with SLE; they may be the initial manifestations, precede the diagnosis, or occur during the disease course.2
Measurement of disease activity in SLE has a central role in clinical research and daily clinical practice for evaluating the response to treatment and achieving the optimal clinical outcomes.3 Therefore, the need for simple and quick markers to identify disease activity is required. Due to its simplicity and low cost, the complete blood count is routinely performed to evaluate any disease-related activity, medication adverse effects or disease related organ damage.4,5 Blood cell count ratios were found to be more informative than blood cell counts alone.6
Our study aimed to evaluate the correlation of different hematological parameters with disease activity, damage indices measured by SLEDAI and SLICC/ACR DI scores, with further correlation with some laboratory data related to kidney function in those with lupus nephritis.
Patients and methodsIn this cross-sectional study 80 SLE patients with inactive disease (SLEDAI score<10 points) and 80 patients with active disease (SLEDAI≥10 points)7 were consecutively recruited from Rheumatology and Rehabilitation Department, Faculty of Medicine, Cairo University Hospitals, during the period extending from March 2021 to January 2022, after the approval of the Research Ethics Committee, Faculty of Medicine, Cairo University (MS-12-2021). Informed verbal consent was obtained from all participants according to the Declaration of Helsinki. All the included 160 patients fulfilled the 2019 EULAR/ACR classification criteria for SLE.8
Patients with any of the following conditions were excluded from the study:
Patients with current or a previous history of non-SLE related hematological diseases, neoplasm, diabetes mellitus, heart disease, chronic liver disease, hyperthyroidism, splenectomy, thrombocytopenia, inflammatory bowel disease, psoriasis, or acute or chronic infections (hepatitis B, hepatitis C, or human immunodeficiency virus infection).
Patients receiving blood transfusion three months prior to screening or antiplatelet medications e.g., low dose aspirin or clopidogrel.
Pregnant female patients.
All patients were subjected to full medical history taking, thorough clinical evaluation including calculation of SLEDAI and SLICC/ACR DI scores and laboratory investigations including complete blood count with differential white blood cell count.
Comparison between the two groups was done regarding demographic, clinic and laboratory data including hematological parameters (NLR, NC3R, MLR, PLR, RDW, and MPV). In addition, correlations of the previously mentioned hematological parameters with some clinical and laboratory manifestations, SLEDAI and SLICC/ACR DI and further correlation with some laboratory data related to kidney function in patients with lupus nephritis were done.
Statistical analysisData analysis packages were processed using SPSS version 21 for Windows (SPSS Inc., Chicago, Illinois, USA). Qualitative data were presented as number and percentage. Quantitative data were presented by mean and standard deviation.
Parametric and nonparametric tests of significance were done according to the data type. Chi-square test, Student t-test, and Mann–Whitney test were deployed based on data distribution.
Correlations among variables were assessed using the Pearson coefficient. The level of significance was set at p equal to or below 0.05.
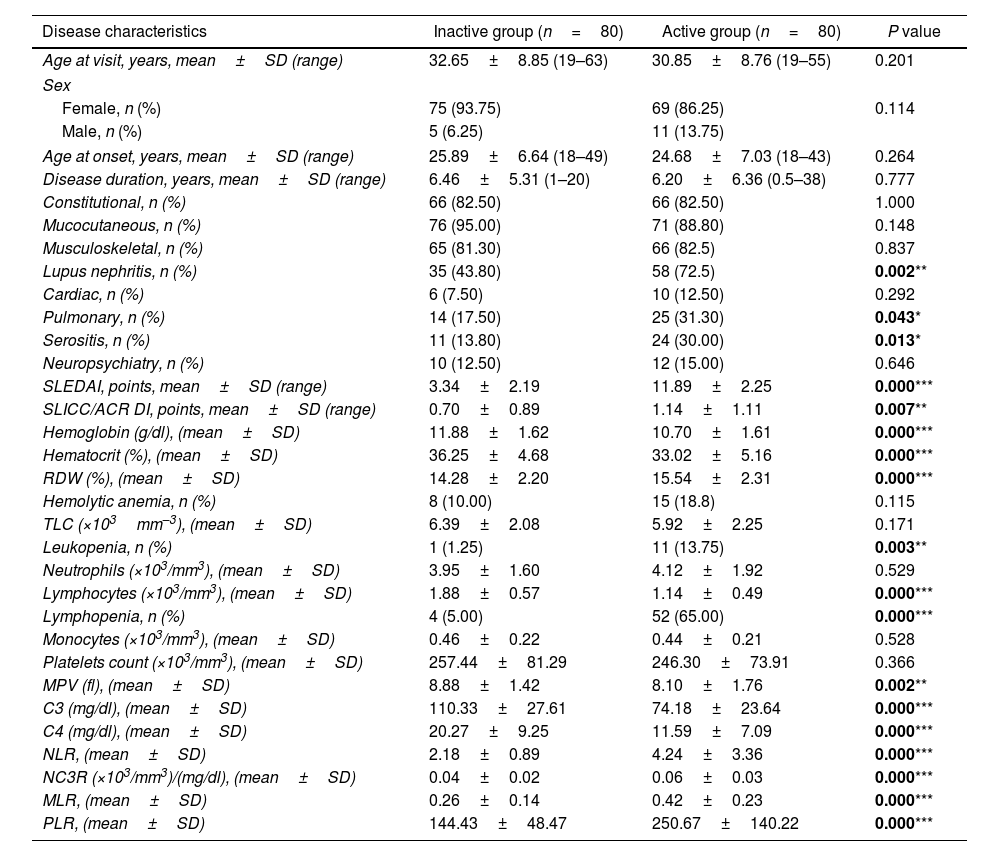
ResultsIn our study Female patients were 144 (90%) while male patients were 16 (10%) with female to male ratio of 9:1. Details of demographic data are shown in Table 1.
The disease characteristics of the studied groups.
| Disease characteristics | Inactive group (n=80) | Active group (n=80) | P value |
|---|---|---|---|
| Age at visit, years, mean±SD (range) | 32.65±8.85 (19–63) | 30.85±8.76 (19–55) | 0.201 |
| Sex | |||
| Female, n (%) | 75 (93.75) | 69 (86.25) | 0.114 |
| Male, n (%) | 5 (6.25) | 11 (13.75) | |
| Age at onset, years, mean±SD (range) | 25.89±6.64 (18–49) | 24.68±7.03 (18–43) | 0.264 |
| Disease duration, years, mean±SD (range) | 6.46±5.31 (1–20) | 6.20±6.36 (0.5–38) | 0.777 |
| Constitutional, n (%) | 66 (82.50) | 66 (82.50) | 1.000 |
| Mucocutaneous, n (%) | 76 (95.00) | 71 (88.80) | 0.148 |
| Musculoskeletal, n (%) | 65 (81.30) | 66 (82.5) | 0.837 |
| Lupus nephritis, n (%) | 35 (43.80) | 58 (72.5) | 0.002** |
| Cardiac, n (%) | 6 (7.50) | 10 (12.50) | 0.292 |
| Pulmonary, n (%) | 14 (17.50) | 25 (31.30) | 0.043* |
| Serositis, n (%) | 11 (13.80) | 24 (30.00) | 0.013* |
| Neuropsychiatry, n (%) | 10 (12.50) | 12 (15.00) | 0.646 |
| SLEDAI, points, mean±SD (range) | 3.34±2.19 | 11.89±2.25 | 0.000*** |
| SLICC/ACR DI, points, mean±SD (range) | 0.70±0.89 | 1.14±1.11 | 0.007** |
| Hemoglobin (g/dl), (mean±SD) | 11.88±1.62 | 10.70±1.61 | 0.000*** |
| Hematocrit (%), (mean±SD) | 36.25±4.68 | 33.02±5.16 | 0.000*** |
| RDW (%), (mean±SD) | 14.28±2.20 | 15.54±2.31 | 0.000*** |
| Hemolytic anemia, n (%) | 8 (10.00) | 15 (18.8) | 0.115 |
| TLC (×103mm–3), (mean±SD) | 6.39±2.08 | 5.92±2.25 | 0.171 |
| Leukopenia, n (%) | 1 (1.25) | 11 (13.75) | 0.003** |
| Neutrophils (×103/mm3), (mean±SD) | 3.95±1.60 | 4.12±1.92 | 0.529 |
| Lymphocytes (×103/mm3), (mean±SD) | 1.88±0.57 | 1.14±0.49 | 0.000*** |
| Lymphopenia, n (%) | 4 (5.00) | 52 (65.00) | 0.000*** |
| Monocytes (×103/mm3), (mean±SD) | 0.46±0.22 | 0.44±0.21 | 0.528 |
| Platelets count (×103/mm3), (mean±SD) | 257.44±81.29 | 246.30±73.91 | 0.366 |
| MPV (fl), (mean±SD) | 8.88±1.42 | 8.10±1.76 | 0.002** |
| C3 (mg/dl), (mean±SD) | 110.33±27.61 | 74.18±23.64 | 0.000*** |
| C4 (mg/dl), (mean±SD) | 20.27±9.25 | 11.59±7.09 | 0.000*** |
| NLR, (mean±SD) | 2.18±0.89 | 4.24±3.36 | 0.000*** |
| NC3R (×103/mm3)/(mg/dl), (mean±SD) | 0.04±0.02 | 0.06±0.03 | 0.000*** |
| MLR, (mean±SD) | 0.26±0.14 | 0.42±0.23 | 0.000*** |
| PLR, (mean±SD) | 144.43±48.47 | 250.67±140.22 | 0.000*** |
n: number, SD: standard, SLEDAI: Systemic Lupus Erythematosus Disease Activity Index, SLICC/ACR DI: Systemic Lupus International Collaboration Clinics/American College of Rheumatology Damage Index, C3: complement 3, C4: complement 4, MPV: mean platelet volume, RDW: red cell distribution width, TLC: total leukocytic count, MLR: monocyte to lymphocyte ratio, NC3R: neutrophil to C3 ratio, NLR: neutrophil to lymphocyte ratio, PLR: platelet to lymphocyte ratio.
Regarding the clinical and laboratory data, We found that the active group has statistically significantly lower mean hemoglobin level, hematocrit and MPV (P=0.00, 0.00 and 0.002); and higher mean of RDW, NLR, NC3R, MLR and PLR (P=0.00, P=0.00, P=0.00, P=0.00 and P=0.00) respectively further details are shown in Table 1.
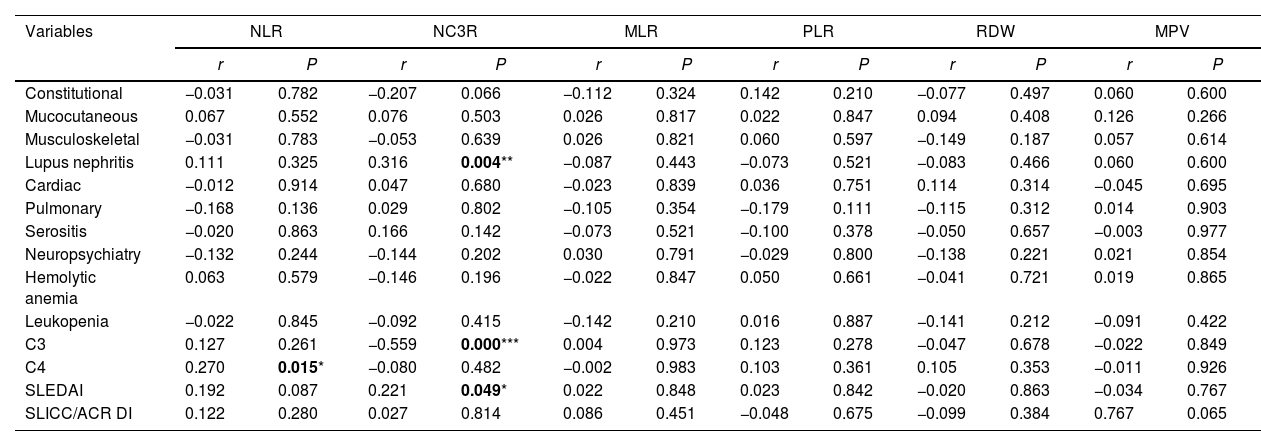
Correlations between the hematological parameters and the clinical and laboratory findings of the active groupThe NC3R showed direct correlation with lupus nephritis and SLEDAI scores (r=0.316, P=0.004; and r=0.221, P=0.049, respectively). The NC3R of the active group was inversely correlated with C3 levels (r=−0.559, P=0.000). Moreover, there was a direct correlation between NLR and C4 levels of the active SLE group (r=0.270, P=0.015) as shown in Table 2.
Correlations of the hematological parameters with the clinical and laboratory findings of the active group.
| Variables | NLR | NC3R | MLR | PLR | RDW | MPV | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| r | P | r | P | r | P | r | P | r | P | r | P | |
| Constitutional | −0.031 | 0.782 | −0.207 | 0.066 | −0.112 | 0.324 | 0.142 | 0.210 | −0.077 | 0.497 | 0.060 | 0.600 |
| Mucocutaneous | 0.067 | 0.552 | 0.076 | 0.503 | 0.026 | 0.817 | 0.022 | 0.847 | 0.094 | 0.408 | 0.126 | 0.266 |
| Musculoskeletal | −0.031 | 0.783 | −0.053 | 0.639 | 0.026 | 0.821 | 0.060 | 0.597 | −0.149 | 0.187 | 0.057 | 0.614 |
| Lupus nephritis | 0.111 | 0.325 | 0.316 | 0.004** | −0.087 | 0.443 | −0.073 | 0.521 | −0.083 | 0.466 | 0.060 | 0.600 |
| Cardiac | −0.012 | 0.914 | 0.047 | 0.680 | −0.023 | 0.839 | 0.036 | 0.751 | 0.114 | 0.314 | −0.045 | 0.695 |
| Pulmonary | −0.168 | 0.136 | 0.029 | 0.802 | −0.105 | 0.354 | −0.179 | 0.111 | −0.115 | 0.312 | 0.014 | 0.903 |
| Serositis | −0.020 | 0.863 | 0.166 | 0.142 | −0.073 | 0.521 | −0.100 | 0.378 | −0.050 | 0.657 | −0.003 | 0.977 |
| Neuropsychiatry | −0.132 | 0.244 | −0.144 | 0.202 | 0.030 | 0.791 | −0.029 | 0.800 | −0.138 | 0.221 | 0.021 | 0.854 |
| Hemolytic anemia | 0.063 | 0.579 | −0.146 | 0.196 | −0.022 | 0.847 | 0.050 | 0.661 | −0.041 | 0.721 | 0.019 | 0.865 |
| Leukopenia | −0.022 | 0.845 | −0.092 | 0.415 | −0.142 | 0.210 | 0.016 | 0.887 | −0.141 | 0.212 | −0.091 | 0.422 |
| C3 | 0.127 | 0.261 | −0.559 | 0.000*** | 0.004 | 0.973 | 0.123 | 0.278 | −0.047 | 0.678 | −0.022 | 0.849 |
| C4 | 0.270 | 0.015* | −0.080 | 0.482 | −0.002 | 0.983 | 0.103 | 0.361 | 0.105 | 0.353 | −0.011 | 0.926 |
| SLEDAI | 0.192 | 0.087 | 0.221 | 0.049* | 0.022 | 0.848 | 0.023 | 0.842 | −0.020 | 0.863 | −0.034 | 0.767 |
| SLICC/ACR DI | 0.122 | 0.280 | 0.027 | 0.814 | 0.086 | 0.451 | −0.048 | 0.675 | −0.099 | 0.384 | 0.767 | 0.065 |
C3: complement 3, C4: complement 4, MLR: monocyte to lymphocyte ratio, MPV: mean platelet volume, NC3R: neutrophil to C3 ratio, NLR: neutrophil to lymphocyte ratio, PLR: platelet to lymphocyte ratio, RDW: red cell distribution width, SLEDAI: Systemic Lupus Erythematosus Disease Activity Index, SLICC/ACR DI: Systemic Lupus International Collaboration Clinics/American College of Rheumatology Damage Index.
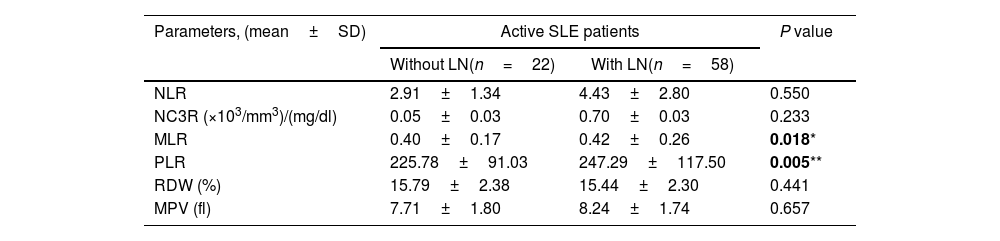
Among the active group, lupus nephritis was found in 58 patients. The mean of MLR and PLR was significantly higher in the active SLE nephritis patients compared to those without nephritis (P=0.018 and P=0.005, respectively) Table 3.
Comparison between the studied parameters in patients with and without lupus nephritis.
| Parameters, (mean±SD) | Active SLE patients | P value | |
|---|---|---|---|
| Without LN(n=22) | With LN(n=58) | ||
| NLR | 2.91±1.34 | 4.43±2.80 | 0.550 |
| NC3R (×103/mm3)/(mg/dl) | 0.05±0.03 | 0.70±0.03 | 0.233 |
| MLR | 0.40±0.17 | 0.42±0.26 | 0.018* |
| PLR | 225.78±91.03 | 247.29±117.50 | 0.005** |
| RDW (%) | 15.79±2.38 | 15.44±2.30 | 0.441 |
| MPV (fl) | 7.71±1.80 | 8.24±1.74 | 0.657 |
LN: lupus nephritis, MLR: monocyte to lymphocyte ratio, MPV: mean platelet volume, n: number, NC3R: neutrophil to C3 ratio, NLR: neutrophil to lymphocyte ratio, PLR: platelet to lymphocyte ratio, RDW: red cell distribution width, SD: standard deviation, SLE: systemic lupus erythematosus.
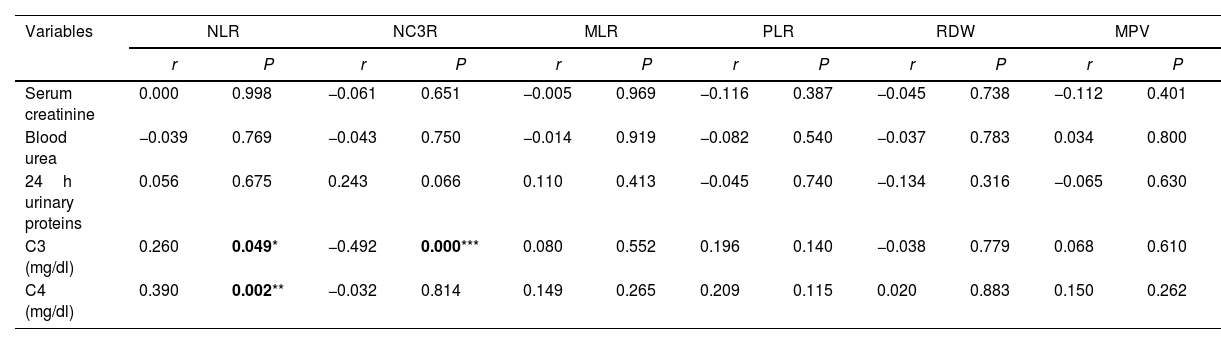
The NLR showed direct correlation with C3 and C4 (r=0.260, P=0.049; and r=0.390, P=0.002, respectively). Moreover, NC3R was inversely correlated to C3 (r=−0.492, P=0.000) as shown in Table 4.
Correlations of the hematological parameters with laboratory findings related to kidney functions in active systemic lupus erythematosus patients with nephritis.a
| Variables | NLR | NC3R | MLR | PLR | RDW | MPV | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| r | P | r | P | r | P | r | P | r | P | r | P | |
| Serum creatinine | 0.000 | 0.998 | −0.061 | 0.651 | −0.005 | 0.969 | −0.116 | 0.387 | −0.045 | 0.738 | −0.112 | 0.401 |
| Blood urea | −0.039 | 0.769 | −0.043 | 0.750 | −0.014 | 0.919 | −0.082 | 0.540 | −0.037 | 0.783 | 0.034 | 0.800 |
| 24h urinary proteins | 0.056 | 0.675 | 0.243 | 0.066 | 0.110 | 0.413 | −0.045 | 0.740 | −0.134 | 0.316 | −0.065 | 0.630 |
| C3 (mg/dl) | 0.260 | 0.049* | −0.492 | 0.000*** | 0.080 | 0.552 | 0.196 | 0.140 | −0.038 | 0.779 | 0.068 | 0.610 |
| C4 (mg/dl) | 0.390 | 0.002** | −0.032 | 0.814 | 0.149 | 0.265 | 0.209 | 0.115 | 0.020 | 0.883 | 0.150 | 0.262 |
C3: complement 3, C4: complement 4, MLR: monocyte to lymphocyte ratio, MPV: mean platelet volume, NC3R: neutrophil to C3 ratio, NLR: neutrophil to lymphocyte ratio, PLR: platelet to lymphocyte ratio, RDW: red cell distribution width.
SLE is a multisystem autoimmune disease with a wide spectrum of manifestations that vary greatly between patients and even in the same patient over time.9
Because of the predilection toward different changes in blood cell lines in SLE, blood cell count ratios tend to be more informative than blood cell counts (CBC) per se.10 Novel CBC-derived parameters are thoroughly studied as proposed markers to correlate with activity and prognosis in various rheumatic and non-rheumatic diseases.11
The studied hematological parameters were distinguishably featuring the active and inactive SLE patients; Patients with active SLE had higher values of NLR, NC3R, MLR, PLR, and RDW and lower value of MPV compared to patients with inactive SLE. The higher values of NLR, MLR, and PLR may be explained by lymphopenia and antilymphocyte antibodies that are more prone to occur in active SLE.12,13 Moreover, consumed complement levels indicate high disease activity.14 The significant decrease in C3 levels of the active SLE, especially active nephritis patients compared to the inactive SLE explains the increase in NC3R of the active SLE group.
The elevated RDW in active SLE may be explained by impaired cell maturation of erythroid progenitor or decreased production or activity of erythropoietin in the bone marrow.15 On the other hand, decreased MPV levels may be explained as a consequence of platelets’ ultrastructural abnormalities such as blebbing and decreased size by cytoskeleton and microtubule rearrangements in active SLE.16 Furthermore, activated platelets are consumed preferentially at the site of inflammation, and consequently high platelet turnover is reflected as low MPV value during active SLE disease.17
Some studies have suggested that NLR is closely correlated with the presence of SLE and its activity.18,19 However, the study reported by Chandrashekara and his colleagues found that the active SLE may not always be predicted by the elevated NLR and that the NLR and SLEDAI did not have a consistent association.20
A few studies investigated the relationship of NC3R and MLR with SLE. Yu and his colleagues found that NC3R was higher in SLE patients with SLEDAI score≥10 compared to SLE patients with SLEDAI score<10, which agrees with our results.21 Also, a retrospective analysis of 136 patients with SLE revealed high MLR values in patients with high SLEDAI scores.22
Regarding PLR, various studies have suggested that PLR is closely correlated with the presence of SLE and its activity.3,11,23–25 Which goes hand in hand with our results.
The RDW and MPV showed diagnostic and prognostic values in various rheumatological diseases.26 In a study recruiting 60 SLE patients, the RDW values were significantly higher in the active patients compared with the inactive patients, and it was concluded that RDW in SLE patients can serve as a useful index to estimate the disease activity.27 Similarly, a previous study found that the level of RDW in active SLE group was significantly higher than that in the inactive SLE.28
On reviewing the literature, there were contradictory results regarding MPV value and disease activity. Our study showed significantly lower MPV values in the active SLE patients compared to the inactive group, which goes hand by hand to that found by Fitri and her colleagues showed significantly lower MPV values in the active SLE patients compared to the inactive group,29 which is not the case in a previous study.30
In this study the correlation of the hematological parameters with the SLEDAI, the SLICC/ACR DI, and the clinical and laboratory findings of each studied group has been reported.
The NC3R in the active groups showed direct association with lupus nephritis. And, exclusively, the NC3R of the active group showed a direct correlation with SLEDAI scores. In agreement with our results, Yu and his colleagues found that NC3R had a direct association with the SLEDAI scores (r=0.353, P<0.01).21
There was an inverse relationship between the PLR and SLICC/ACR DI. Similarly, to that found by El-Said and her colleagues.24
Regarding the renal involvement, the mean of MLR and PLR was significantly higher in the active SLE nephritis patients compared to active SLE patients without nephritis. The change in lymphocyte, monocyte, and platelet levels with the exacerbation of systemic inflammatory response may be able to better characterize lupus activity and lupus nephritis.31 Liu and his colleagues demonstrated that the levels of MLR and PLR were significantly increased in lupus nephritis patients without infection as compared with those in healthy controls.32 Consistent with our findings, Qin and his colleagues demonstrated significantly higher PLR levels in SLE patients with nephritis than in those without nephritis.33 Our findings showed insignificantly high NLR levels in SLE patients with active nephritis; however, Qin and his colleagues showed significantly high NLR levels in SLE patients with nephritis.
Our study showed that NLR in patients with renal involvement had direct significant association with C3 and C4, while no correlation was found between NLR and serum creatinine. Correlation analysis of Tang and his colleagues found similar results; however, in contrast with our findings, they reported direct significant correlation between NLR and serum creatinine.34
In the current study there was an inverse relationship between NC3R and C3, which was explained by reduction of complement level during disease flare because of its activation by immune complexes.35 Therefore, NC3R may clearly distinguish the degree of SLE activity in lupus nephritis.
ConclusionThe commonly used complete blood cell parameters NLR, NC3R, MLR, PLR, RDW, and MPV were found to be useful for determining active disease especially in patients with active lupus nephritis.
LimitationsThe limitations of this research may be attributable to the small patient's number. Further longitudinal observations, preferably multicenter studies, are needed.
Ethical considerationThis research was considered a minimal risk and obtained authorization from the Research ethics Committee of the faculty of medicine, Cairo University (code MS-12-2021). Verbal consent were taken from all patients participated in the study. Hopeful that our research be published in your respectable journal.
FundingNo funding was given to this research.
Conflict of interestThere is no conflict of interest associated with the manuscript and no funding was given.
