


The main goal of our study is to compare the hamstring/quadriceps (H/Q) ratio at different knee angles between level-matched male and female soccer players and to determine whether differences in the H/Q ratio exist between the dominant and the non-dominant leg.
MethodsA cross-sectional study design was used to compare an isometric H/Q ratio and functional isokinetic ratio (between hamstring in eccentric contraction and quadriceps in concentric contraction) between males (n=14) and females (n=14). These ratios were studied at two different speeds of movement (60°s−1 and 180°s−1) and in five different positions (40°, 50°, 60°, 70° and 80° degrees of knee flexion).
ResultsOur results showed no differences in the H/Q ratio between genders. The ratio in the dominant leg showed an average of 9% higher values. The ratios were an average of 53.4% lower in positions near flexion than in positions near extension.
ConclusionsFor both men and women, the results showed lower ratios in the non-dominant leg compared to the dominant leg. At higher velocities, the force ratios were higher, while in more knee-flexed positions, the ratios were lower. Finally, we did not find differences in ratios between men and women.
El objetivo principal del estudio es comparar el ratio de fuerza isquiotibial/cuádriceps (ratio H/Q) en diferentes ángulos de rodilla entre jugadores de fútbol de niveles similares y determinar si existen diferencias en dicho ratio entre la pierna dominante y la no dominante.
MétodosSe utilizó un diseño transversal para comparar el ratio isométrico H/Q y el ratio funcional isocinético (ratio entre la fuerza durante una contracción excéntrica de isquiotibial y la fuerza durante una contracción concéntrica de cuádriceps) entre hombres (n=14) y mujeres (n=14). Estos ratios se estudiaron en dos velocidades (60° s−1 y 180° s−1) y en 5 posiciones diferentes (40, 50, 60, 70 y 80 grados de flexión de rodilla).
ResultadosNuestros resultados no mostraron diferencias significativas en el ratio H/Q entre sexos. El ratio en la pierna dominante mostró valores un 9% más altos que en la pierna no dominante. Los ratios fueron de media un 53.4% más bajos en posiciones cercanas a la flexión que en posiciones cercanas a la extensión.
ConclusionesPara ambos sexos los resultados mostraron ratios más bajos en la pierna no dominante comparado con la pierna dominante. A velocidades superiores, los ratios de fuerza fueron mayores, mientras que en posiciones de mayor flexión de rodilla los ratios fueron menores. Por último, no se encontraron diferencias significativas en los ratios entre hombres y mujeres.
O principal objetivo do nosso estudo é comparar a relação de força entre Isquiotibiais/Quadríceps (H/Q) em diferentes ângulos do joelho entre jogadores de futebol (masculino e feminino) de níveis semelhantes para determinar se existem diferenças na relação entre H/Q entre o membro dominante e a não-dominante.
MétodoU estudo de delineamento transversal foi utilizado para comparar a relação isométrica entre H/Q e isocinética funcional (razão entre a força dos isquiotibiais em contração excêntrica e do quadríceps em contração concêntrica, durante a extensão do joelho) entre homens (n=14) e mulheres (n=14). Estas razões foram estudadas em duas velocidades diferentes de movimento (60°/s e 180°/s) e em cinco posições diferentes (por exemplo 40, 50, 60, 70, e 80 graus de flexão do joelho).
ResultadosOs resultados não mostraram diferenças significativas na relação H/Q entre os sexos. A relação da perna dominante mostrou valores médios de 9% mais elevados em relação a perna não dominante. As proporções foram, em média, 53,4% menor em posições próximas a flexão do que em posições perto da extensão.
ConclusõesPara ambos os sexos, os resultados mostram razões mais baixas no membro não dominante em comparação com a dominante. À velocidade mais elevadas, as relações de força foram superiores, enquanto que em maiores flexões de joelho as relações foram menores. Finalmente, não foram encontradas diferenças significativas nas proporções entre homens e mulheres.
The ratio between the strength of the hamstring (flexor muscles) and that of the quadriceps (extensor muscles), also known in the literature as the H/Q ratio, has been widely used in the fields of sports training and rehabilitation to describe the strength properties of muscles that affect the knee joint and to detect muscle imbalances.1 The conventional H/Q ratio is defined as the ratio between the peak torque of the hamstring and the quadriceps and is generally measured during a concentric contraction, while the functional H/Q ratio is defined as the ratio between the peak torque of the hamstring during an eccentric contraction and the peak torque of the quadriceps during a concentric contraction (Hecc/Qcon) (representative of knee extension).2,3 Low values of the H/Q strength ratio (<0.6 for 60°s−1) may increase the risk of injury to the lower limb, especially anterior cruciate ligament (ACL) injuries and hamstring strains.4,5 Female athletes are 4 times more likely to suffer an ACL injury than their male counterparts.6,7 In recent years, some authors have linked the higher incidence of ACL injury to a reduced H/Q strength ratio in women.8,9
Although some studies have found differences in the H/Q ratio between males and females,8 there is insufficient evidence to show that level-matched athletes performing the same sport and undergoing similar training programs show sex-related differences. In fact, studies that compared active men and women with similar activity levels did not find significant differences in the strength ratio between the anterior and posterior thigh muscles.10,11
On the other hand, some articles suggest that women may have a reduced H/Q ratio in some knee joint positions,12 however, as far as we know, no study has compared the strength ratios between level-matched athletes at different knee joint angles. We consider this comparison important because the realization of certain technical gestures required in specific sports involves the activation of different muscles throughout their range of movement; consequently, the risk of injury can vary.
Soccer players may display unequal development of the right and left limbs due to certain technical actions performed in the sport, and such unequal development can cause functional or even structural asymmetries. The dominance of one side of the body over the other produces a greater ability of the dominant side and may involve differences in the strength of various muscles that depend on the actions required in the sport. Some studies of soccer players have shown differences in strength and flexibility between the dominant and the non-dominant leg13 and even biomechanical asymmetries between them.14
In this study, our aims were (i) to compare the functional and conventional H/Q ratios between level-matched male and female soccer players at different knee angles and (ii) to determine whether differences in the H/Q ratio exist between the dominant and non-dominant leg in these players.
MethodExperimental approachThis study was designed as a cross-sectional group comparison. The participants were divided into two groups using sex (i.e., male or female) as the classification criterion. Body mass and height were measured for each subject. One week before the day of the test, the subjects attended a familiarization session in which the procedures of the study were explained and in which they learned how to execute the various protocols. In the test session, isometric and isokinetic torque (at 60°s−1, 180°s−1) were recorded. These data permit comparisons between groups to assess possible differences in the Hecc/Qcon functional ratio.
SubjectsTwenty-eight subjects voluntarily participated in the study. The subjects were divided into two groups, the female group (FG), composed of 14 women with a mean (standard error of measurement; SEM) age of 22.62 (4.69) years, height of 166.15 (4.06) cm and weight of 60.08 (6.23)kg, and the male group (MG) composed of 14 men with an age of 20.64 (1.63) years, height of 177.36 (3.56) cm and weight of 70.00 (4.65)kg. All of the subjects were level-matched soccer players who trained approximately 10h per week. To be included in the study, subjects were required to have regularly participated in official competitions. The exclusion criteria were (i) muscular lower limb injury, (ii) knee surgery or major ligament injury during the last two years, and (iii) the occurrence of any muscular or orthopedic problem during the test week.
All subjects were informed of the study protocols and gave written consent to participate in the study. The protocols complied with the requirements of the Helsinki Declaration of 1975 and its subsequent revision in 2008. The Institutional Review Board of the University of Valencia approved the study.
ProceduresThe maximum hamstring and quadriceps torque was assessed isokinetically. A dynamometer (Biodex multi-joint system V.4X, Biodex Medical Systems Inc., Shirley, New York, USA) was used to obtain these measurements. Before measurements were taken, each individual performed a warm-up consisting of quadriceps and hamstring stretching and 3 submaximal repetitions of isokinetic quadriceps and hamstring strength for each speed (i.e., 60°s−1, 180°s−1). In both measurements, the axis of rotation of the dynamometer lever was visually aligned with the lateral malleolus, and the trunk, hips, thighs, and ankles were strapped to the dynamometer. During isometric testing, individuals were asked to sit with their lower limbs positioned 60° from the anatomical position of knee extension. Three repetitions, each five seconds in duration, were recorded with one-minute rest periods in between.
Following the recommendations of Brown and Weir,15 the subjects were asked to sit with 90° hip flexion and an initial knee flexion of 100° during the isokinetic measurements. Four repetitions were recorded at each of the two speeds listed above, and the maximal torque during the repetitions was measured. The tests performed were (i) knee extension and flexion for registering the concentric and eccentric actions, respectively, of the quadriceps; and (ii) knee flexion and extension for exploring the eccentric and concentric actions, respectively, of the hamstring. The first three repetitions were performed at an angular velocity of 60°s−1 and the subsequent repetitions at 180°s−1. Higher angular velocities were avoided to minimize the risk of injury due to excessively powerful movements. For each measurement, a gravity correction was performed following the device manufacturer's instructions. The rest period between velocities and movements was 90s. The range of motion was fixed between 100 and 20° knee flexion.
The testing procedures were identical for both legs; the order of assessment of the two legs was counterbalanced.
Signal processingMatlab 7.0 (Mathworks Inc., Natick, USA) was used to process the strength signals. For isometric signals, the average value of the central second period was established. The mean value for the three repetitions was set as the maximum isometric torque for flexion and extension movements. The H/Q isometric ratio was calculated by dividing the flexor maximum isometric torque by the extensor maximum isometric torque.
For isokinetic signals, the torque at 40°, 50°, 60°, 70° and 80° of knee flexion was established using two repetitions of the movement at each velocity. The mean value of the two repetitions was set as the torque for each joint angle. Moreover, the peak torque for the same two repetitions was found, and the mean value was taken as the isokinetic peak torque. Conventional (i.e., Hcon/Qcon) and functional (i.e., Hecc/Qcon) H/Q ratios were calculated for each joint angle and for isokinetic peak torque.
Statistical analysesSPSS 17 for Windows (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Basic statistical methods were applied to obtain the mean as descriptive of the central tendency and the standard error of the mean as descriptive of the statistical dispersion.
The assumptions of normality (Kolmogorov–Smirnov test), homoscedasticity (Levene test) and sphericity (Mauchly's test) were tested before performing differential statistical analysis. For the isometric measurements, a mixed model [Group (2)×Leg (2)] ANOVA was applied to establish the effects of ‘group’ and ‘leg’ tested on the dependent variables. A mixed model [Group (2)×Leg (2)×Velocity (2)×Joint angle (6)×type of ratio] ANOVA was applied to establish the effects on the isokinetic variables. Follow-up of the multivariate contrast was performed through univariate contrast. Post hoc analysis with Bonferroni correction was performed in the case of significant main or interaction effects. The significance level for all tests was set at p<0.05.
ResultsIsometric measurementsThere were no main or interaction effects of the H/Q isometric ratio. Women showed a mean (SEM) isometric ratio of 0.48 (0.01), while men showed a mean value of 0.49 (0.02). For both men and women, the average values of dominant leg showed an isometric ratio of 0.51 (0.01), while the non-dominant leg showed an isometric ratio of 0.47 (0.01).
Isokinetic H/Q ratioFor the H/Q isokinetic ratio, univariate contrast showed significant effects of velocity (F1,312=69.17; p<0.001; η2p=0.18),angle of the ratio (F5,312=26.42; p<0.001; η2p=0.3), leg (F1,312=4.27; p=0.04; η2p=0.14) and type of ratio (F1,312=603.9; p<0.001; η2p=0.66). In addition, the interactions type of ratio×angle of the ratio (F5,312=16.27; p<0.001; η2p=0.21), velocity×type of ratio (F1.312=175.42; p<0.001; η2p=0.36) and velocity×type of ratio×angle of the ratio (F5.312=5.02; p<0.001; η2p=0.07) were significant in the dependent variable.
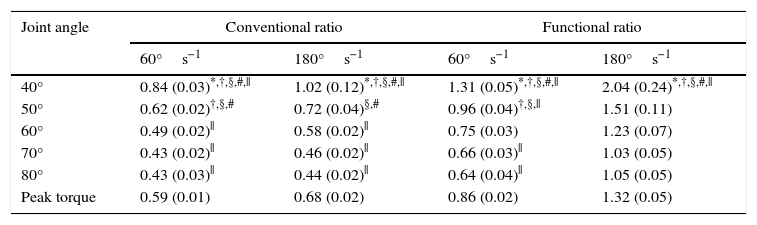
The H/Q isokinetic ratio was higher at 180°s−1 (mean=1.0; SEM=0.03) than at 60°s−1 (mean=0.73; SEM=0.01). Moreover, the conventional ratio (mean=0.63; SEM=0.01) showed a lower value than the functional ratio (mean=1.09; SEM=0.03). The H/Q ratio showed higher values in the dominant leg (mean=0.9; SEM=0.03) than in the non-dominant leg (mean=0.82; SEM=0.02). There were differences in the H/Q ratio values depending on the knee angle; these differences are shown in Table 1.
Differences in conventional and functional ratios by extension angle.
| Joint angle | Conventional ratio | Functional ratio | ||
|---|---|---|---|---|
| 60°s−1 | 180°s−1 | 60°s−1 | 180°s−1 | |
| 40° | 0.84 (0.03)*,†,§,#,|| | 1.02 (0.12)*,†,§,#,|| | 1.31 (0.05)*,†,§,#,|| | 2.04 (0.24)*,†,§,#,|| |
| 50° | 0.62 (0.02)†,§,# | 0.72 (0.04)§,# | 0.96 (0.04)†,§,|| | 1.51 (0.11) |
| 60° | 0.49 (0.02)|| | 0.58 (0.02)|| | 0.75 (0.03) | 1.23 (0.07) |
| 70° | 0.43 (0.02)|| | 0.46 (0.02)|| | 0.66 (0.03)|| | 1.03 (0.05) |
| 80° | 0.43 (0.03)|| | 0.44 (0.02)|| | 0.64 (0.04)|| | 1.05 (0.05) |
| Peak torque | 0.59 (0.01) | 0.68 (0.02) | 0.86 (0.02) | 1.32 (0.05) |
Data are expressed as the mean (SEM).
The major findings of our study were the detection of increased strength at angles closer to knee extension compared to more flexed positions and a lack of a difference in the H/Q ratios between men and women.
In the first part of the study, H/Q ratios were compared between male and female players. The results showed no differences in any of the ratios between the sexes. Some authors who compared the H/Q ratios of male and female level-matched athletes with similar activity levels10,11 have reported results similar to those found in our study. In these studies, it was suggested that the lower H/Q ratios reported by others may have been due to the lack of control of extraneous variables such as age or training background. Thus, in our work, we were very careful to control variables that may affect the detection of muscle imbalance differences (e.g., hours of training, level of training and training type). Therefore, the main conclusion that may be drawn from these results is that, despite some anatomical and physiological disadvantages that may predispose them to injury,16 women soccer players training at the same level as men do not show differences in the prognosis of injury based on force ratios.
Another controversial issue is the comparison between the dominant and the non-dominant leg. In our study, the dominant leg showed significantly higher H/Q ratios than the non-dominant leg. There is a specific reason that may explain the differences between legs. Soccer is a sport that involves some actions in which only the dominant leg is required or in which the two legs perform different movements (e.g., long pass, shooting goal); thus, the dominant leg may perform more varied actions. In addition, some of the movements performed by the dominant leg place greater strength demands on the hamstring that those performed by the non-dominant leg. This fact may explain the differences found in our work.
Concerning the limb angle at which the ratio was calculated, we found significant differences (i.e., angles closer to extension show higher ratios than more flexed angles). The actions typically performed while shooting at a soccer goal have the following dynamic. At the beginning of the action, the hamstring performs a slightly eccentric contraction,17,18 while at the end of the action the eccentric contraction of the hamstring provides braking essential for knee protection; therefore, the magnitude of the force is very high. This action, which is repeated many times in a match and over many matches, strengthens the hamstrings involved when the knee is close to extension. However, far from reassuring therapists who care for soccer players, this fact should warn them of the risk to the knee in flexed positions. Although some experts think that shooting actions are the most important, other actions such as braking or direction changes require hamstring eccentric force in knee-flexed positions. The hamstring strength in eccentric contraction may be increased at these angles to avoid anterior tibial translation.2
Because the force application time is different for each speed of motion, the flexo-extension velocity should also be considered. Thus, we found higher forces at lower velocities (60°s−1), and this may influence the relationship between the quadriceps and the hamstring. The eccentric contraction is not as greatly influenced by varying the speed as is the concentric contraction.2 In our study, the concentric contraction was performed by the quadriceps. Thus, comparing speeds of 180°s−1 and 60°s−1, quadriceps strength was greater than hamstring strength at the lower speed. This may explain the higher ratios found at higher velocities (180°s−1). In addition, there is greater knee stabilization in situations in which greater joint stress is expected, such as high-velocity movements or actions in which the knee is close to full extension.17,19,20
The primary limitation of our study is related to the lack of nervous system activity measurement (EMG). Future research should attempt to deepen our understanding of the motor patterns that underlie agonist–antagonist coordination.
In conclusion, our results show lower H/Q ratios in the non-dominant leg compared to the dominant leg. With respect to velocity, our results confirm that the force ratios are higher at higher velocities, while in the more knee-flexed position, lower deficient ratios were found. Finally, we found no differences in H/Q ratios between men and women.
Conflict of interestThe authors have no conflicts of interest to declare.
The authors would like to thank Dr. Xavier García-Massó (University of Valencia, Valencia, Spain) for his contribution to this study.
