


Violence against women is widely recognized as a serious public health problem. The pregnancy is a risk factor for increasing the violence, especially when it is related to socio-economic conditions. The objective of this work is to ascertain the relation between violence against women during pregnancy in developed countries and in developing countries. It was performed a systematized review. It was proceeded a search of the literature through online databases MEDLINE and SciELO in December 2013, only with articles published between January 1, 2003 and November 30, 2013. The following descriptors were used for searching on the database “domestic violence” (Medical Subject Headings [MeSH]); “violence against women” (Health Sciences Descriptors [DeCS]); and “pregnancy” (Keyword). The Search strategies resulted in 71 studies. After analysis of the titles and abstracts of articles found for eligibility based on inclusion criteria, 43 articles were deleted and 28 articles were included in the final sample. The study revealed the predominance of researches developed about violence against women during pregnancy in developing countries, strengthening the strong socio-economic character related to victims and aggressors.
A violência contra a mulher é amplamente reconhecida como grave problema de saúde pública a gestação se configura em um incremento ao risco de violência, especialmente quando relacionada a condições sócio- econômicas. O objetivo desse trabalho é verificar a relação entre a violência contra a mulher na gestação em países desenvolvidos e países em desenvolvimento. Foi realizada uma revisão sistemática qualitativa. Procedeu-se busca na literatura através de bases de dados on line MEDLINE e SicELO em dezembro de 2013, limitando-se a artigos publicados entre 1 de janeiro de 2003 e 30 de novembro de 2013. Utilizaram-se os seguintes descritores para a busca na base “domestic violence” (descritor Medical Subject Headings [MeSH]); “violence against women” (descritor em Ciências da Saúde [DeCS]); e “gravidez” (palavra-chave). As estratégias de buscas resultaram em 71 estudos. Após análise dos títulos e dos resumos dos artigos encontrados para elegibilidade com base nos critérios de inclusão, 43 artigos foram excluídos e 28 artigos foram incluídos na amostra final. O estudo revelou a predominância de pesquisas desenvolvidas acerca da violência contra a mulher na gestação em países em desenvolvimento, fortalecendo o forte caráter sócio-econômico relacionado às vítimas e aos agressores.
Violence against women is widely recognized as a serious public health problem. In its various forms, it can be considered as every act of violence by reason of gender, able to generate physical, sexual, psychological damage and suffering, included, in this context, threat of such acts, coercion, and arbitrary deprivation of freedom, which may occur in instance of public or private life.1
Such injury can be considered multifactorial, once that is associated with the cultural and historical issues, especially with regard to gender issues, by understanding that these denote power relations between the sexes. We can understand, therefore, that genre is a set of relationships, attributes, roles, beliefs and attitudes that define what means to be a man or a woman.2 In that context, the violence against women exposes the vulnerability in domestic relations, perpetrating a financial or emotional dependency context, frequent and historically evidenced in the society.
The concept of domestic violence refers to all forms of violence committed in the family environment. However, it may also reflect the violence against women perpetrated by their intimate partner. In most cases, it is not recognized as violence, it is considered a cultural phenomenon, as a form of disciplinary action against wives and daughters.3 Studies conducted in developed and developing countries show that the prevalence of domestic violence against women varies from 10 to 70%.4
Multicenter study on domestic violence, coordinated by the World Health Organization (WHO), found that the prevalence of violence perpetrated by intimate partner at some point in life varies between 15% in Japan and 71% in Ethiopia, with prevalence of physical or sexual violence in the last year between 4% and 54%, respectively.5
Violence against women may occur at any stage of their lives, including pregnancy. The Pan-American Health Organization (PAHO) defines violence during pregnancy as violence or threat of physical, sexual or psychological (emotional) violence against pregnant women.6 In the literature review it was observed prevalence from 0.9% to 20.1%.7 Schraiber and D’Oliveira,8 highlight studies that consider pregnancy as an increment to the risk of violence against women, being able to change the pattern as to the frequency and severity during this period, or even be initiated at this stage of a woman's life.
The implications of this event have an impact not only in the life of the woman, but also in the life of the fetus and the future child, among them bleeding and termination of pregnancy.9 With regard to the health of the child, it had been evidenced increased risk of perinatal death, born with low birth weight and prematurity.10
Some women's life situations have been described as domestic violence related factors: low socioeconomic status, low level of social support, being of African descent and young.11 Highlighted the magnitude of the subject as a World damage, It is necessary to consider the Association of social determinants in the revelation incidence and prevalence indexes, the fact is ratified in the extension numbers when compared between developing countries and developed countries and the effects triggered by that phenomenon in the gravid-puerperal cycle.
The most sensitive look that showed the gender violence as a public health problem permeated the policies of confrontation in various sectors of attention to vulnerable groups, especially the woman in the health, social and security fields. It is noticed empirically that from 2003 the identification, notification, and combating mechanisms of this damage, has been intensified as a result of extensive discussions in the various policy areas. In Brazil, the creation in 2006 of the Maria da Penha law represented an important role in combating domestic violence against women; however, its effectiveness finds the social barriers that keep women as hostages of intimate partners, following the example of other developing countries.
Based on these data, it is from 2003 that the data relates the violence against women specifically in gestational period were more clearly delineated and exposed on research, seeking to identify related factors, the indexes of incidence and prevalence as well as the confronting ways of that problem. Thus, the objective is to verify the relation between violence against women during pregnancy in developed countries and developing countries.
MethodIt was performed a systematized review of published articles about violence against women during pregnancy in electronic databases previously selected. The qualitative approach was elected whereas other methods as: meta-analysis (a) relevant information for the calculation and result of the sample cannot be measured by restricting the amount of studies; (b) the definition of “violence” has many different interpretations among the studies involved in the sample, it makes difficult to establish a statistical parameter among the various studies.
It was performed a research in the literature through online databases Medical Literature Analysis and Retrieval Systen Online (MEDLINE) and Scientific Eletronic Library Online (SciELO), limited to articles published between January 1, 2003 and November 30, 2013. The reason to limit this search to aforesaid interval was because during this period, It was noticed an intensification of studies about violence against women, and such fact passed to be the focus of attention in the Politics of Integral Attention to Women's Health. Initially, the following descriptors were used to search in the MEDLINE database: 1. “domestic violence” (Medical Subject Headings [MeSH]); 2. “violence against women” (Health Sciences Descriptors [DeCS]); and 3. “pregnancy” (key word).
The research conducted were 1 AND 2, 3. Beyond the MeSH descriptor, it was chosen to include the descriptor in health sciences “violence against women” and the keyword “pregnancy” on search strategy, since, they are not part of the list of MeSH descriptors, and they delineate better the subject of this review. The search strategy and the items obtained in the search were reviewed on two separate occasions to ensure proper sample selection.
A similar search strategy was held in the SciELO database, by using the descriptors related before and the equivalent descriptors in Portuguese language. In order to standardize the concepts about violence against women during pregnancy covered in this review, it was used a definition of the Pan-American Health Organization which consists of violence or threat of physical, sexual or psychological (emotional) violence against pregnant woman.
The analysis of the article followed previously determined eligibility criteria. It was adopted the following criteria for inclusion: (1) articles that had the title at least a combination of the terms described in search strategy; (2) publications written in english or in portuguese; (3) studies that address the theme of violence against women during pregnancy; (4) articles with full text accessible through the Capes Portal de Periódicos (Coordination for the Improvement of Higher Education Personnel), a library connected to the Brazilian Ministry of Education and with a content restricted to authorized users; and (5) prospective or retrospective observational studies (descriptive or analytical, except for studies of case), experimental or almost experimental. The exclusion criteria were: (1) other study designs, e.g. case reports, case series, literature reviews and comments; (2) non-original studies, including editorials, reviews, forewords, short communications and letters to the editor.
Then, each article of the sample was entirety read, and the information was inserted in a spreadsheet that included authors, year of publication, description of the sample of the study and the main findings. Some studies found were not only about pregnant women, but, in puerperal stage, and then such data were not recorded by the study because the focus of the study was the violence against women during pregnancy,
In order to perform a better data analysis, the next stage involved the comparison among the studies and their grouping by heuristics reasons, According to the results obtained from each study in 3 categories: Indexes of violence against pregnant women in developing countries; the relationship of violence with intimate partners, and the repercussions of violence against women during pregnancy.
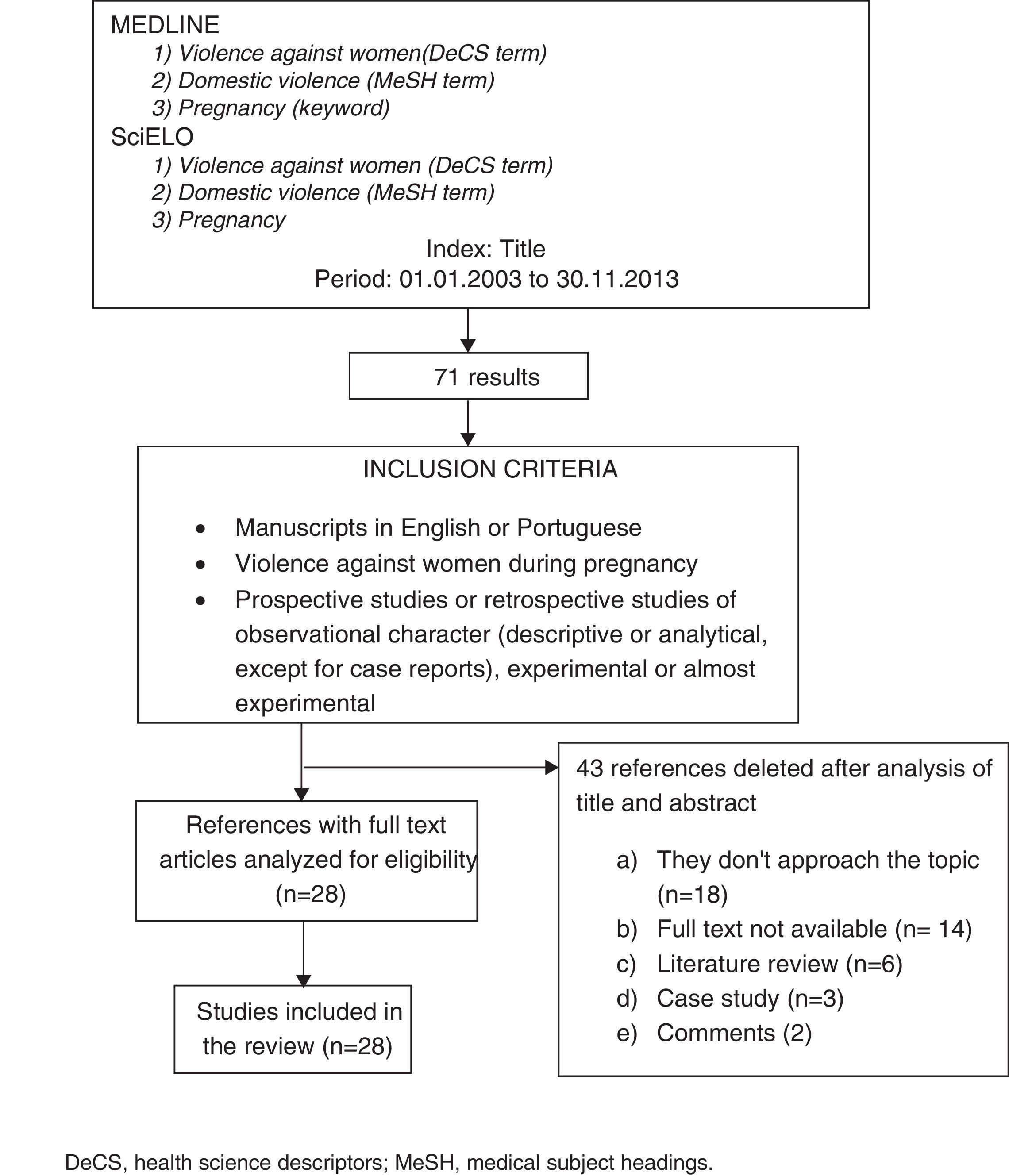
ResultsInitially, the research strategies resulted in 71 studies. After analysis of the titles and abstracts of articles found through eligibility on the basis of the criteria of inclusion, 43 articles were deleted and 28 articles were included in the final sample (Fig. 1).

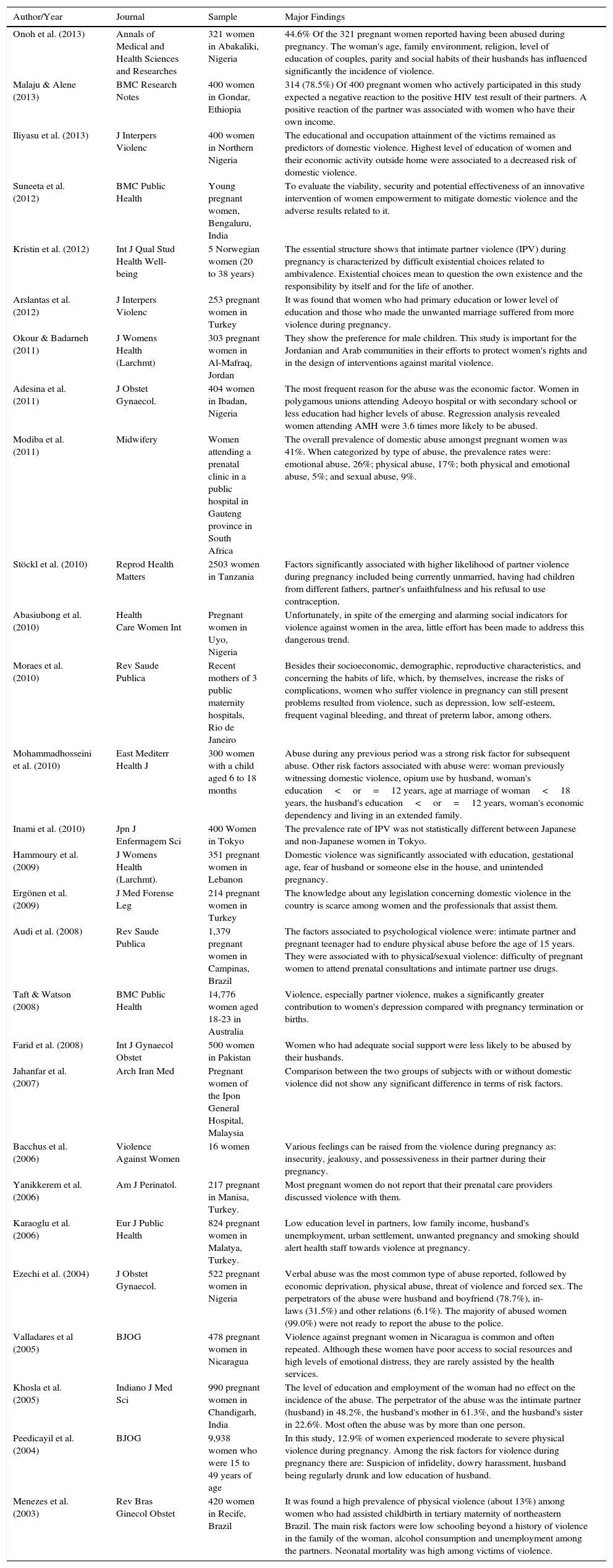
Table 1 provides an overview of all studies included in the final sample and all used in the process of analyzing the information. As for the design of study, it was concluded 22 cross-sectional studies, 1 case-control study, 1 randomized-study, 2 prospective cohort studies and 1 statistical regression analysis study. The 28 studies were distributed in three categories previously determined: Indexes of violence pregnant women in developing countries (13 studies); the relation of violence to intimate partners (8 studies) and Consequences of violence against women in pregnancy (7 studies).
Violence against women in pregnancy: studies and major findings.
| Author/Year | Journal | Sample | Major Findings |
|---|---|---|---|
| Onoh et al. (2013) | Annals of Medical and Health Sciences and Researches | 321 women in Abakaliki, Nigeria | 44.6% Of the 321 pregnant women reported having been abused during pregnancy. The woman's age, family environment, religion, level of education of couples, parity and social habits of their husbands has influenced significantly the incidence of violence. |
| Malaju & Alene (2013) | BMC Research Notes | 400 women in Gondar, Ethiopia | 314 (78.5%) Of 400 pregnant women who actively participated in this study expected a negative reaction to the positive HIV test result of their partners. A positive reaction of the partner was associated with women who have their own income. |
| Iliyasu et al. (2013) | J Interpers Violenc | 400 women in Northern Nigeria | The educational and occupation attainment of the victims remained as predictors of domestic violence. Highest level of education of women and their economic activity outside home were associated to a decreased risk of domestic violence. |
| Suneeta et al. (2012) | BMC Public Health | Young pregnant women, Bengaluru, India | To evaluate the viability, security and potential effectiveness of an innovative intervention of women empowerment to mitigate domestic violence and the adverse results related to it. |
| Kristin et al. (2012) | Int J Qual Stud Health Well-being | 5 Norwegian women (20 to 38 years) | The essential structure shows that intimate partner violence (IPV) during pregnancy is characterized by difficult existential choices related to ambivalence. Existential choices mean to question the own existence and the responsibility by itself and for the life of another. |
| Arslantas et al. (2012) | J Interpers Violenc | 253 pregnant women in Turkey | It was found that women who had primary education or lower level of education and those who made the unwanted marriage suffered from more violence during pregnancy. |
| Okour & Badarneh (2011) | J Womens Health (Larchmt) | 303 pregnant women in Al-Mafraq, Jordan | They show the preference for male children. This study is important for the Jordanian and Arab communities in their efforts to protect women's rights and in the design of interventions against marital violence. |
| Adesina et al. (2011) | J Obstet Gynaecol. | 404 women in Ibadan, Nigeria | The most frequent reason for the abuse was the economic factor. Women in polygamous unions attending Adeoyo hospital or with secondary school or less education had higher levels of abuse. Regression analysis revealed women attending AMH were 3.6 times more likely to be abused. |
| Modiba et al. (2011) | Midwifery | Women attending a prenatal clinic in a public hospital in Gauteng province in South Africa | The overall prevalence of domestic abuse amongst pregnant women was 41%. When categorized by type of abuse, the prevalence rates were: emotional abuse, 26%; physical abuse, 17%; both physical and emotional abuse, 5%; and sexual abuse, 9%. |
| Stöckl et al. (2010) | Reprod Health Matters | 2503 women in Tanzania | Factors significantly associated with higher likelihood of partner violence during pregnancy included being currently unmarried, having had children from different fathers, partner's unfaithfulness and his refusal to use contraception. |
| Abasiubong et al. (2010) | Health Care Women Int | Pregnant women in Uyo, Nigeria | Unfortunately, in spite of the emerging and alarming social indicators for violence against women in the area, little effort has been made to address this dangerous trend. |
| Moraes et al. (2010) | Rev Saude Publica | Recent mothers of 3 public maternity hospitals, Rio de Janeiro | Besides their socioeconomic, demographic, reproductive characteristics, and concerning the habits of life, which, by themselves, increase the risks of complications, women who suffer violence in pregnancy can still present problems resulted from violence, such as depression, low self-esteem, frequent vaginal bleeding, and threat of preterm labor, among others. |
| Mohammadhosseini et al. (2010) | East Mediterr Health J | 300 women with a child aged 6 to 18 months | Abuse during any previous period was a strong risk factor for subsequent abuse. Other risk factors associated with abuse were: woman previously witnessing domestic violence, opium use by husband, woman's education<or=12 years, age at marriage of woman<18 years, the husband's education<or=12 years, woman's economic dependency and living in an extended family. |
| Inami et al. (2010) | Jpn J Enfermagem Sci | 400 Women in Tokyo | The prevalence rate of IPV was not statistically different between Japanese and non-Japanese women in Tokyo. |
| Hammoury et al. (2009) | J Womens Health (Larchmt). | 351 pregnant women in Lebanon | Domestic violence was significantly associated with education, gestational age, fear of husband or someone else in the house, and unintended pregnancy. |
| Ergönen et al. (2009) | J Med Forense Leg | 214 pregnant women in Turkey | The knowledge about any legislation concerning domestic violence in the country is scarce among women and the professionals that assist them. |
| Audi et al. (2008) | Rev Saude Publica | 1,379 pregnant women in Campinas, Brazil | The factors associated to psychological violence were: intimate partner and pregnant teenager had to endure physical abuse before the age of 15 years. They were associated with to physical/sexual violence: difficulty of pregnant women to attend prenatal consultations and intimate partner use drugs. |
| Taft & Watson (2008) | BMC Public Health | 14,776 women aged 18-23 in Australia | Violence, especially partner violence, makes a significantly greater contribution to women's depression compared with pregnancy termination or births. |
| Farid et al. (2008) | Int J Gynaecol Obstet | 500 women in Pakistan | Women who had adequate social support were less likely to be abused by their husbands. |
| Jahanfar et al. (2007) | Arch Iran Med | Pregnant women of the Ipon General Hospital, Malaysia | Comparison between the two groups of subjects with or without domestic violence did not show any significant difference in terms of risk factors. |
| Bacchus et al. (2006) | Violence Against Women | 16 women | Various feelings can be raised from the violence during pregnancy as: insecurity, jealousy, and possessiveness in their partner during their pregnancy. |
| Yanikkerem et al. (2006) | Am J Perinatol. | 217 pregnant in Manisa, Turkey. | Most pregnant women do not report that their prenatal care providers discussed violence with them. |
| Karaoglu et al. (2006) | Eur J Public Health | 824 pregnant women in Malatya, Turkey. | Low education level in partners, low family income, husband's unemployment, urban settlement, unwanted pregnancy and smoking should alert health staff towards violence at pregnancy. |
| Ezechi et al. (2004) | J Obstet Gynaecol. | 522 pregnant women in Nigeria | Verbal abuse was the most common type of abuse reported, followed by economic deprivation, physical abuse, threat of violence and forced sex. The perpetrators of the abuse were husband and boyfriend (78.7%), in-laws (31.5%) and other relations (6.1%). The majority of abused women (99.0%) were not ready to report the abuse to the police. |
| Valladares et al (2005) | BJOG | 478 pregnant women in Nicaragua | Violence against pregnant women in Nicaragua is common and often repeated. Although these women have poor access to social resources and high levels of emotional distress, they are rarely assisted by the health services. |
| Khosla et al. (2005) | Indiano J Med Sci | 990 pregnant women in Chandigarh, India | The level of education and employment of the woman had no effect on the incidence of the abuse. The perpetrator of the abuse was the intimate partner (husband) in 48.2%, the husband's mother in 61.3%, and the husband's sister in 22.6%. Most often the abuse was by more than one person. |
| Peedicayil et al. (2004) | BJOG | 9,938 women who were 15 to 49 years of age | In this study, 12.9% of women experienced moderate to severe physical violence during pregnancy. Among the risk factors for violence during pregnancy there are: Suspicion of infidelity, dowry harassment, husband being regularly drunk and low education of husband. |
| Menezes et al. (2003) | Rev Bras Ginecol Obstet | 420 women in Recife, Brazil | It was found a high prevalence of physical violence (about 13%) among women who had assisted childbirth in tertiary maternity of northeastern Brazil. The main risk factors were low schooling beyond a history of violence in the family of the woman, alcohol consumption and unemployment among the partners. Neonatal mortality was high among victims of violence. |
Violence against women according to the studies is related directly to low socio-economic level of the women and their Intimate partner,12–14 their main aggressor.5 Considering these aspects, it was found a greater number of studies set in developing countries (23 studies), with different approaches, in contrast, only 3 studies were developed in developed countries.
The finding of these studies reinforce the risk factors listed by the multicenter study conducted by OMS,5 in which, among the countries included in the study, large variations of prevalence of physical and sexual violence were recorded. The lowest rate was observed in Japan (8%), followed by Servia and Montenegro (13%), Thailand (11%) and the highest rates were recorded in Brazil, in the cities of Zona da Mata [Forrest Region] in Pernambuco (32%), and in a province in Peru (44%).15
African countries have developed a significant number of studies about the issue of violence against women, especially during pregnancy, and important scientific studies with relevant samples were developed by deepening the discussion on the need for more effective social policies for this population. In total, 9 studies had the backdrop of African countries, in different regions of the continent, with emphasis on the studies carried out in Nigeria (5 studies).
The studies conducted in Nigeria revealed a variation of prevalence of violence in pregnancy of 17%16 to 58,6%,13 however, the samples were variables, as well as the data collection instruments, representing a research bias, which makes the establishment of a uniform parameter difficult to measure.
With regard to the profile of victims and aggressors, the results of the Nigerian research were uniforms. The victims were monogamous women, with low level of education and financial dependence of their respective partners.12,13,16 The aggressors, most of them were intimate partners,12,13,16,17 the low level education is repeated.
In the remaining countries of the African continent, other factors emerge as aggravating to the risk factors for violence as the infidelity of a partner, the fact of the woman being single in current pregnancy and have children from different fathers, besides, the refusal of the woman to use contraceptive methods.18 This last event will result in significant repercussions on women's health and the future child, since it will increase the number of unwanted pregnancies, such fact, will focus on women's mental health, shaping up as a risk factor for depression and the abortion practice.19
When categorized the types of violence, there is a prevalence of violence defined as verbal and emocional.17,20,21 However, the physical and sexual violence, and the economic abuse practiced by intimate partners were recorded at high rates, the physical abuse, for example, reaches 17%.20,22
In the countries of the Asian continent, studies that underscore the religiosity and culture as predictors in the phenomenon of violence against women were found. A study conducted in Iran showed that the abuse during any previous period was a strong risk factor for subsequent abuse. Other risk factors associated to abuse were: woman testifying previously domestic violence, the use of opium by her husband, the woman education<or=12 years, the age of marriage of the woman<18 years, the husband's education<or=12 years, the economic dependence of the woman.23 It is noteworthy in this context the emergence of a psychoactive substance popular in that country (opium), and the early age of marriages, common in the culture of Islamic countries.
Other relevant data with regard to risk factors is related to the fact that women who witnessed domestic violence are more likely to be victims of this abuse, for a cultural issue. Thus, it is not recognized as a form of violence, often being accepted as a cultural phenomenon,1 it is part of the customs and norms of the society who understand and accept violence against women as a form of disciplinary action exercised on wives and daughters.5
Another study brought a cultural particularity, in which, the emotional/verbal physical abuse is not only by intimate partner, but also by the mother-in-law and sisters-in-law. In this Indian study, the author of abuse was the intimate partner (husband) in 48.2%, the husband's mother in 61.3%, and husband's sister in 22.6%. In most cases the abuse amounted to more than one person.24
Indian studies also have excelled in this theme. The discrepancy is typical of developing countries as social disparities between the very rich and the very poor, which emphasize public health problems such as gender violence. The same study22 disagrees with those who make up this review. The level of women's education and employment had no effect on the incidence of the abuse, underscoring the financial dependence and education for submission, as hypothesis that reflect this reality.
Other Indian research with a sample ten times greater than the previous one, revealed a similar context to other countries studied in this review. In this study, 12.9% of women have experienced moderate to severe physical violence during pregnancy. Among the risk factors for violence during pregnancy there are: suspicion of infidelity, harassment, her husband's low educational level and his alcoholism.25
The Asian continent by its vast territorial extension, and cultural, ethnic, and economic differences showed distinct traces in the polls that address violence against women during pregnancy. A study conducted in Japan, in a maternity ward in Tokyo, revealed that there is no statistical difference between Japanese women and non-Japanese women assisted in that service. But, it was agreed with the other studies conducted in developing countries, in which, the history of violence in previous pregnancy has direct influence on acceptance of violence in the current pregnancy.26
Considering the cultural, religious, and ethnic differences of Asia, brings attention, the study conducted in Jordan, predominantly Muslim country that shows a preference for male children. So, the woman according to religious precepts has a lower value in society, such idea is perpetrated among families, based on the rules of the Quran, the Holy Book for Muslims. Violence against women deemed disobedient is a right of the man for such precepts. This study was important to the Jordanian and Arab communities in their efforts to protect the rights of women in the design and in the speeches against marital violence.
The risk factors for violence against women during pregnancy are repeated among developing countries, with peculiarities related to religion and culture, but in general are the same. However, one of the studies, revealed that there is no difference among these risk factors among women who suffer and those who do not suffer violence in pregnancy.27
In the American continent were registered in the parameters of the search 3 studies, 2 in Brasil15,28 and 1 in Nicaragua.29 The results corroborate with the other world's findings, highlighting that the association of aggressors to the use of alcohol and other drugs, the performance of partners, and low adhesion to prenatal.15,28 Other important content that deserve to be highlighted is on the aggravation in that the women who witnessed domestic violence before 15 years old age present higher risk of violence during pregnancy.28
However, a study involving different social and ethnic groups did not show the association among the prevalence, the abuse pattern, and the sociodemographic characteristics.17 Although, the numbers of prevalence among countries of different economic models show the reality found in the studies of this review.
Relation of violence to intimate partnersPresent in most of societies, the violence caused by the intimate partner is the most endemic violence against the woman, the damages to women's health who suffer intimate partner violence (IPV) of a psychological, physic, and sexual type are globally recognized. According to estimates of the World Bank, a Woman has a higher probability of being hit, assaulted and murdered by her actual or previous partner than by a stranger.28
As mentioned previously, the profile of the aggressors, mostly intimate partners is the same worldwide. They have low education, low income or they are unemployed and present vulnerability to abuse of licit and illicit drugs.15,21,25 The implications of IPV arouse fear, insecurity in pregnant women, who suffer the partners feelings of jealousy and possessivity,30 adding to this delicate period in the life of the woman is a risk factor for the situations of violence.
The aggressions caused by intimate partner are predominantly verbal aggressions, emotional and psychological abuse, and financial violence,17,20 also they also reveal themselves in sexual assaults, forced sex, exposing pregnant women to sexually transmitted infections. The woman's economic dependence of the partner adds to other aggravating in the violence during pregnancy, even in anticipation of the results of serological tests for sexually transmitted infections such as HIV, conducted routinely in prenatal care.
A study conducted in Ethiopia showed such relationship. Most participants in this study expect their partner to react negatively to the positive HIV test result. Of 400 pregnant women who actively participated in this study, 314 (78.5%) expected a negative reaction to the positive HIV test result of their partners. A positive reaction of the partner was associated to women who have their own income. Such fact took place because most part of the population studied described to as an occupation being a housewife (59%), thus confirming the financial dependency.31
A qualitative study in Norway recorded the experiences of women who have suffered violence during pregnancy by intimate partner, such research characterized the phenomenon by the view of victims that have associated to violent acts the unpredictability, or something belonging to the partner's own body, stuck to his essence.32
In the same study the participants described the phenomenon as an explosive and uncontrolled anger, which can be expressed by slamming doors, punching the wall, breaking Windows, destroying furniture and throwing food on the walls. The uncertainty of not knowing what cause the anger makes the situation a dramatic and threatening experience.32
As already mentioned is frequent the use of alcoholic beverages by intimate partner and the abuse of other drugs, which dictate or precipitate the violence during pregnancy. Some authors believe that the use of alcohol facilitates the acts of violence, since it modifies the behavior patterns, creating conditions for discussions, insults, name-calling, insults and threats which may culminate in sexual and physical assaults.11,12,15
A study conducted in Campinas, Brazil, proved that the consumption of alcohol and illicit drugs by intimate partner represents a greater likelihood of violence against pregnant women. Such situation can lead to delays in seeking help and, consequently, interventions that would minimize the effects of violence or discontinue these acts.1,11,15
Analyzing the factors that precipitate the IPV during pregnancy, it is possible to affirm that violence is a factor that causes illness not only the victim but also the partner, in this case, the pregnant woman, and the aggressor suffer possible behavioral disorders and/or mental disorders. The mental health care, therefore, should extend the victim and the aggressor.
Repercussions of violence against women during pregnancyThe impact of violence against women during pregnancy involves physical and psychological damage to the woman and to her child. The damage extends to the gynecological and sexual complaints, and several obstetric consequences as unwanted pregnancies,15 start prenatal retardation,15,18,19 abortion and natimortality,20 low birthweigh,19 preterm labor and fetal loss.23,24 May also be present chronic pelvic pain, headache, spastic colons’ disease,25 depression, attempted suicide and posttraumatic stress disorder, anxiety and use of drugs.28
Violence during pregnancy can have serious consequences for women's health, including bleeding and the interruption of pregnancy.18 As for the health of the child, there is an increased risk of perinatal mortality and for newborns with low birth weight or prematurity.15
Violence, especially practiced by the partner, has a major contribution to the development of depression in women, being also responsible for the increase in the number of abortions.19 Such a study was conducted in Australia, a country in which abortion is allowed legally. In this cohort study, it was proven that 43% of women who reported partner violence in 1996, definite themselves as depressed and 45% who suffered violence by partner in 2000. Thirty-eight per cent of women in 1996 and 41% in 2000, who reported “other types of violence,” also reported depression, underlining the strong association between intimate partner violence and depression.
Study in India also recorded the impact on mental health of pregnant women victims of IPV. The total number revealed that the abuse was practiced by more than one person. The emotional effect of this abuse showed depression and anxiety, other reported desire to escape those ceded to such appeal came back after some time, and a smaller number have expressed suicidal thoughts.24
Many studies have reported an association between violence and worse results during pregnancy. Abused women are more likely to register late prenatal care, premature labor or suffer miscarriage or give birth to low-weight babies.33 In addition to the intrinsic physical trauma injury by assault, caused by punches, jostling among other violent acts, like the placental expulsion, another consequence is associated with exposure to continuous stress. The continuous stress seems to affect the perinatal outcome through changes in the behavior of individuals or changing physiological responses. The individual behavior can be engaged in different forms, as interfering on the ability of the individual to maintain its satisfactory nutritional status, rest and healthcare.28
Another result bound to pregnant women victims of violence during pregnancy is associated to the quality of prenatal care, these presented a higher chance of having a prenatal assistance unsatisfactory in relation to the standards set by the institutions linked to the health of the woman and the child. To be a victim of at least one act of physical violence perpetrated by the partner during pregnancy more than doubles the chance of a prenatal of worst quality.34
ConclusionIt is evident the strong relation between violence against women during pregnancy and socio-economic factors, because of the predominance of studies set in developing countries, in which is highlighted the intrinsic factors in the profile of the aggressors, conducted mostly by intimate partner. Such data ratifies gender inequalities reinforced by cultural, social, and religious factors as important links between power relations and violence as a reflection of these associated factors. However, the development predominance of the studies concentrated in developing countries do not underline this phenomenon as a minor relevant problem in developed countries, considering that the violence against women also affects the populations of these countries, with similar characteristics, although in a few number.
Conflicts of interestThe authors declare no conflicts of interest.
Research conduced at Faculdade de Medicina do ABC, Laboratório de Delineamento de Estudos e Escrita Científica, Santo André, SP, Brazil.