



In non-valvular atrial fibrillation (NVAF) with embolic risk, the guidelines recommend oral anticoagulation (OAC), although not all patients receive it. In this study, an attempt is made to identify these patients, and to study factors related to non-anticoagulation.
Material and methodsNon-interventional, cross-sectional, multicentre study was performed on a population of patients ≥18 years with a NVAF diagnosis, moderate-high embolic risk (CHADS2 score≥2), not treated with OAC. Atrial fibrillation (AF) prevalence was also collected.
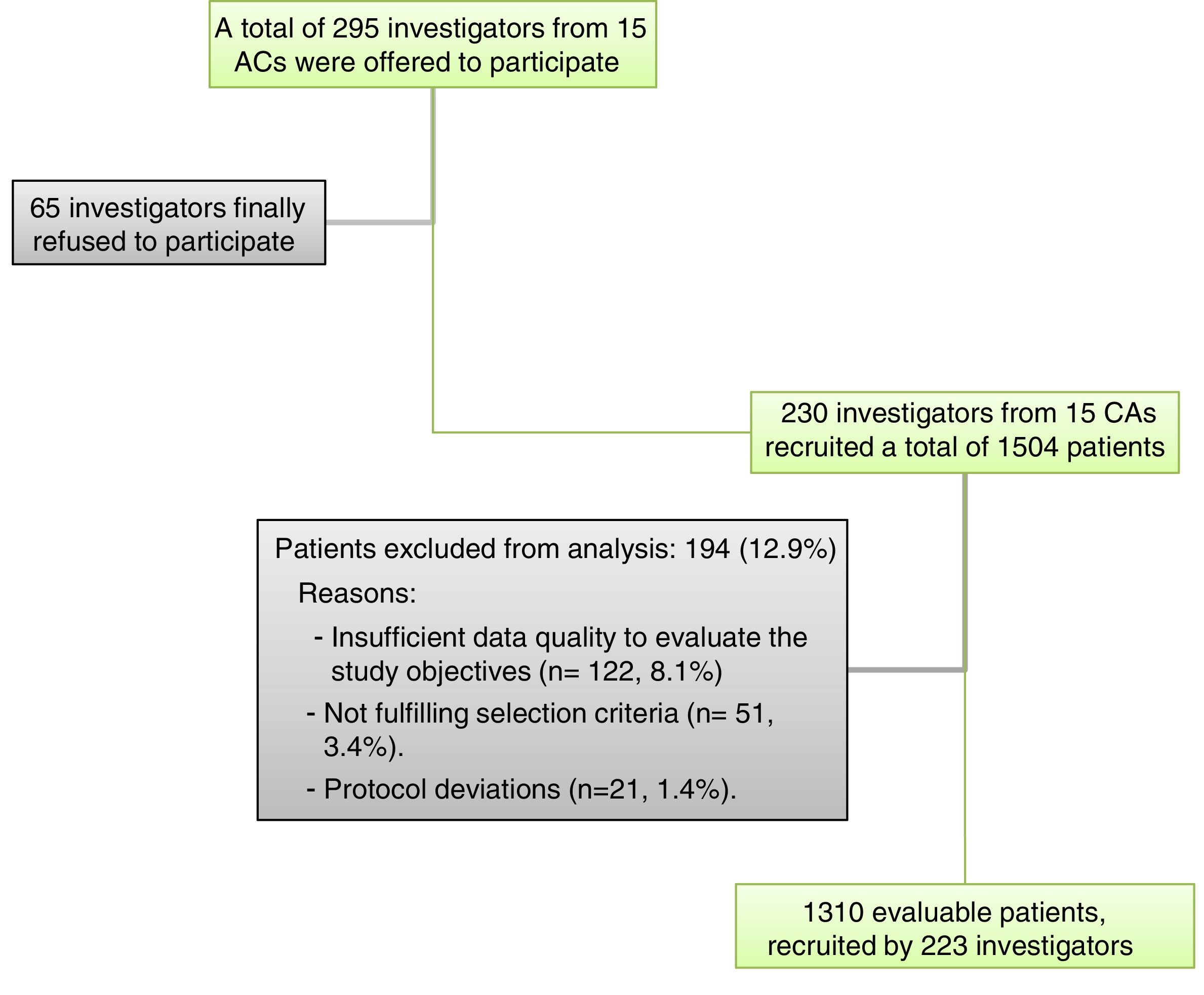
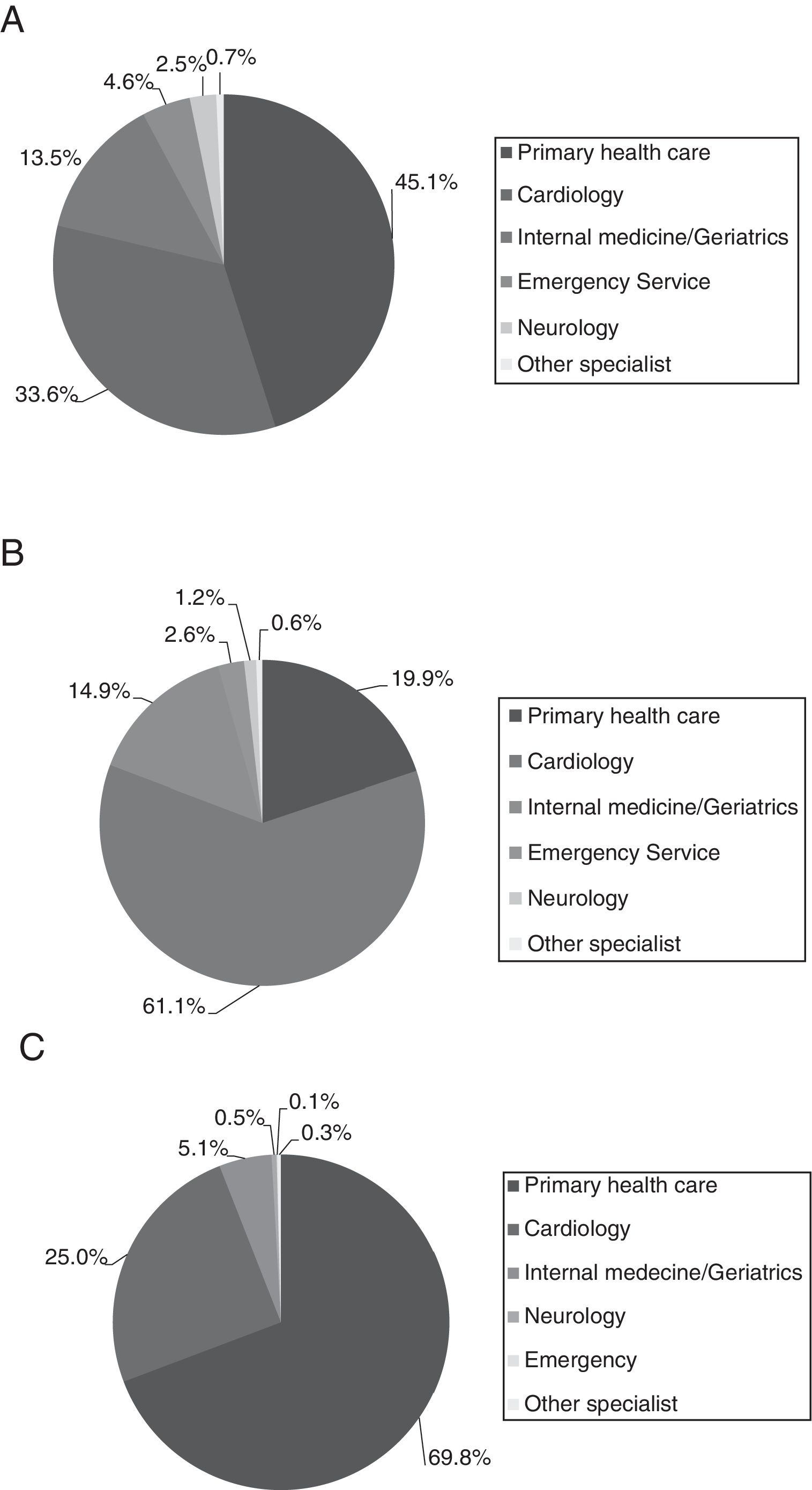
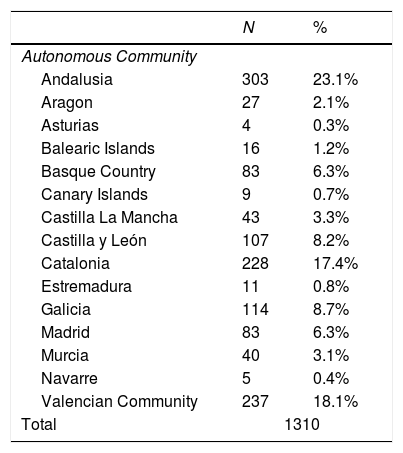
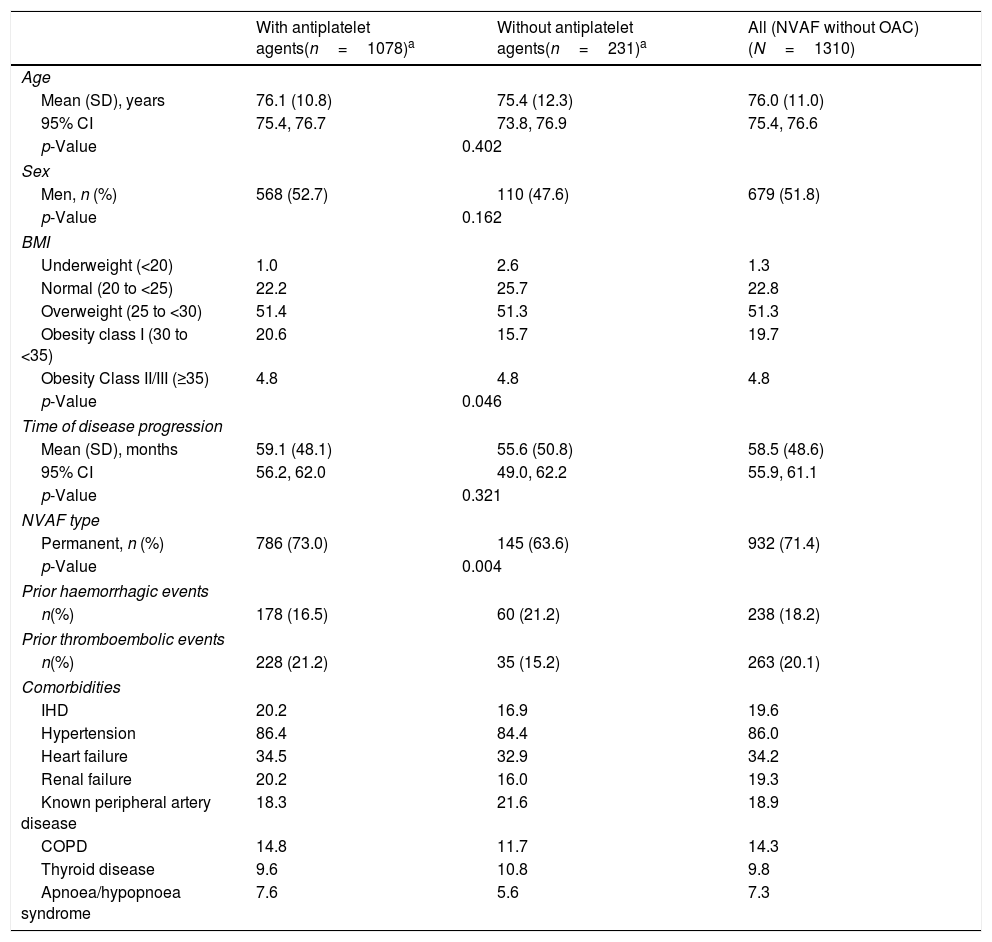
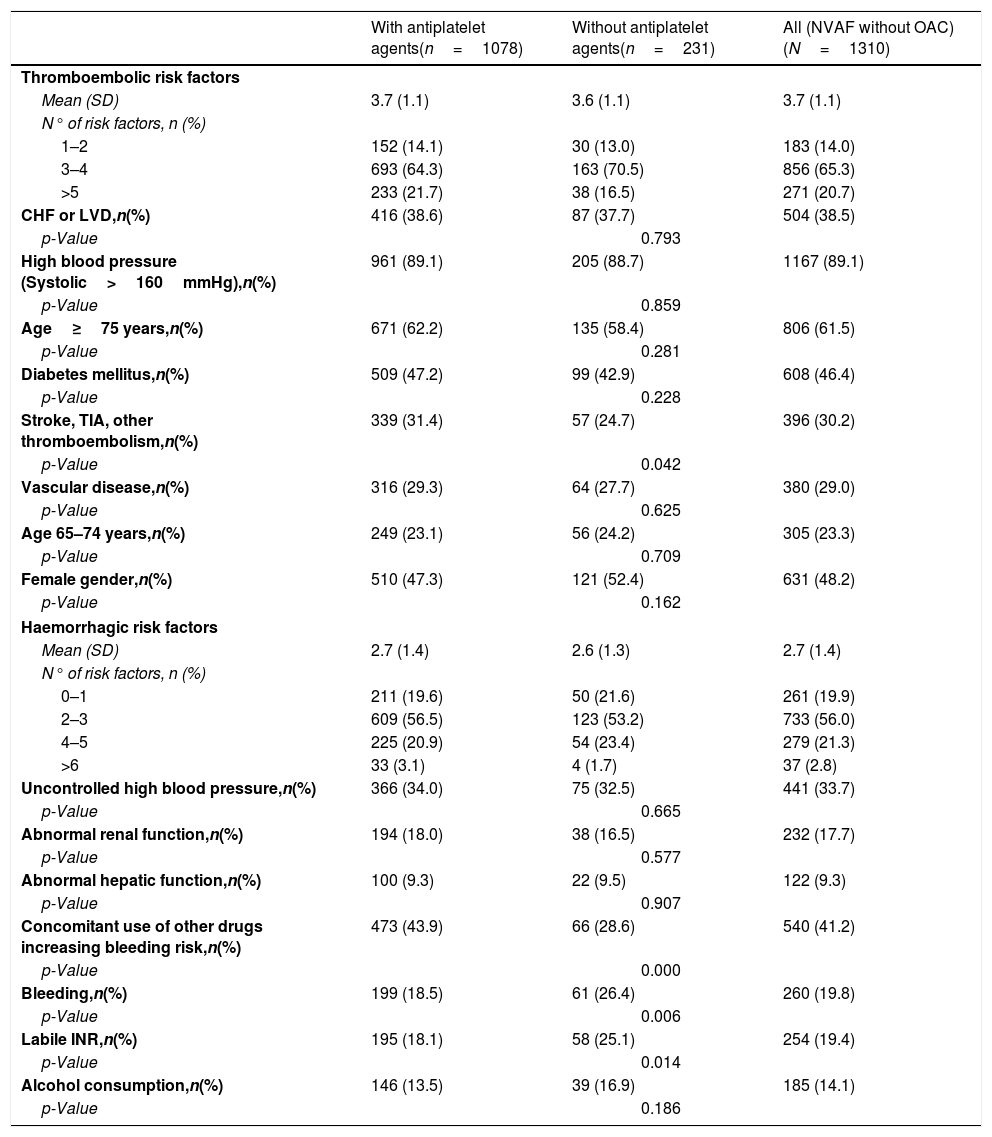
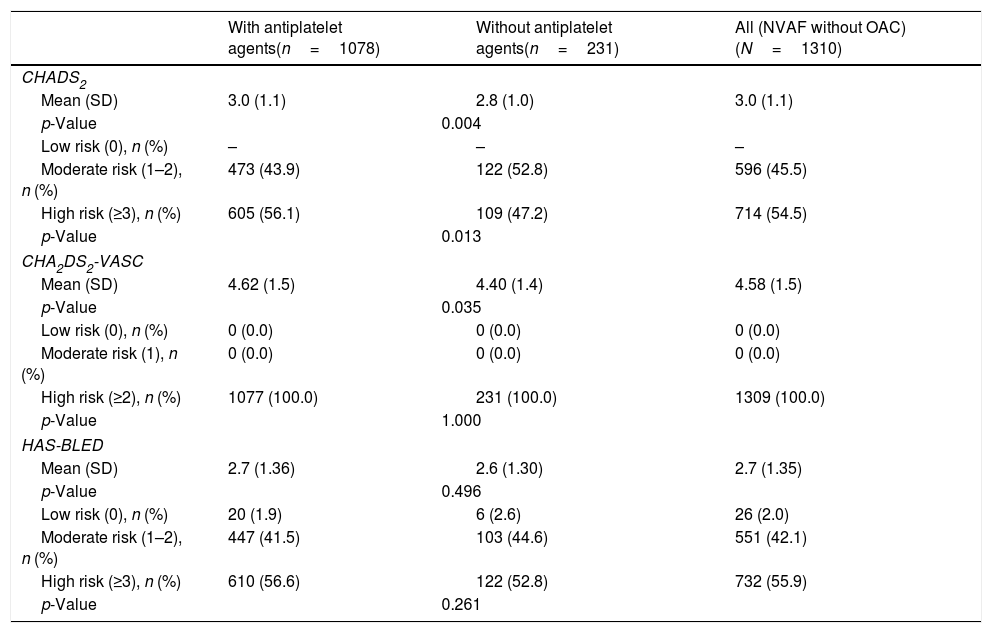
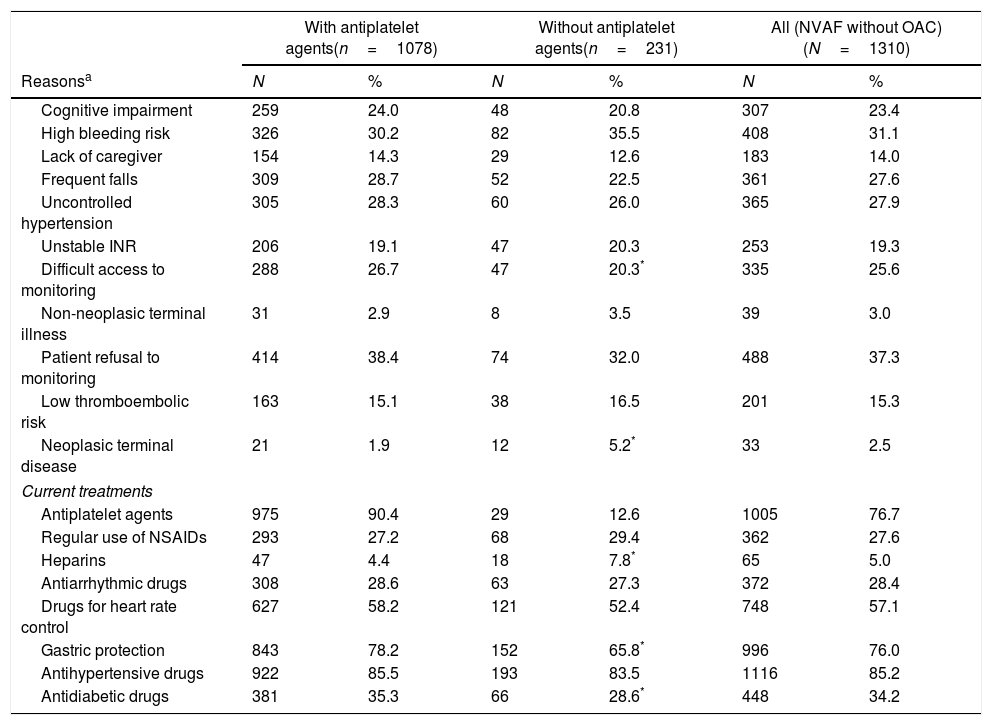
ResultsAF prevalence was 4.5%, and 80.7% of the patients had NVAF (20.0% did not receive OAC). A total of 1310 non-OAC-treated patients were included (51.8% male, mean age: 76.0 years). The mean time since AF diagnosis was 58.4 months. The main therapeutic decision for stroke prevention was prescription of antiplatelet agents (82.4%, n=1078), and the main reasons were: patient refusal to monitoring (37.3%), high bleeding risk (31.1%), uncontrolled hypertension (27.9%), and frequent falls (27.6%). The mean CHA2DS2-VASc score was 4.6, and the HAS-BLED was 2.7 (55.9% of patients scoring HAS-BLED≥3). The most common thromboembolic risk factors were: hypertension (89.1%), age≥75 years (61.5%); the haemorrhagic factors: use of drugs increasing the bleeding risk (41.2%), uncontrolled blood pressure (33.7%).
ConclusionsAbout 20% of Spanish NVAF patients do not receive OAC in the clinical practice and are treated with antiplatelet agents, which do not reduce haemorrhagic risk. Most patients do not clearly show a contraindication to OACs, particularly considering that there are other available options (direct oral anticoagulant drugs [DOACs]).
En la fibrilación auricular no-valvular (FANV) con riesgo embólico las guías recomiendan la anticoagulación oral (ACO), aunque no todos los pacientes la reciben. En este estudio, tratamos de identificar estos pacientes y estudiar los factores relacionados con la no-anticoagulación.
Material y métodosEstudio observacional, transversal y multicéntrico. Población de estudio: pacientes ≥18 años con FANV, riesgo embólico moderado-alto (puntuación CHADS2≥2), no tratados con ACO. También se recogió la prevalencia de fibrilación auricular (FA).
ResultadosLa prevalencia de FA fue del 4,5% y del 80,7% de los pacientes presentaban FANV (20,0% no recibía ACO). Se incluyeron 1.310 pacientes no tratados con ACO (51,8% varones, edad media: 76,0 años). El tiempo medio desde el diagnóstico de FA fue de 58,4 meses. La estrategia terapéutica principal para la prevención tromboembólica fue la antiagregación (82,4%; n=1.078) y las principales razones: negativa del paciente a la monitorización (37,3%), alto riesgo de sangrado (31,1%), hipertensión no controlada (27,9%) y caídas frecuentes (27,6%). La puntuación CHA2DS2-VASc media fue 4,6 y HAS-BLED 2,7 (55,9% HAS-BLED≥3). Los factores de riesgo tromboembólico más frecuentes fueron: hipertensión (89,1%) y edad ≥75 años (61,5%); los factores de riesgo hemorrágico fueron: uso de fármacos que aumentan el riesgo de sangrado (41,2%) y presión arterial no controlada (33,7%).
ConclusionesEn la práctica clínica en España, un 20% de los pacientes con FANV no recibe ACO, y son tratados con antiagregantes, lo que no reduce el riesgo hemorrágico. La mayoría de los pacientes no presenta una clara contraindicación para ACO, más aún considerando otras opciones disponibles (anticoagulantes orales directos [ACOD]).
Artículo
Comprando el artículo el PDF del mismo podrá ser descargado
Precio 19,34 €
Comprar ahora
