




There is a degree of contradiction in the literature about the primary tumour that is most frequently associated with acrometastases, as well as their prognosis and treatment. The aim of this study is to determine the most frequent location of the acrometastases, the most frequent primary tumour according to its location, and to evaluate the surgical options according to the estimated survival.
MethodsA retrospective study on patients diagnosed with acrometastases. The primary tumour, as well as the number, location, symptoms and treatment of the acrometastases and survival rate were collected.
Results35 acrometastases in 21 patients were reviewed: 4 in the upper limbs and 31 in the lower limbs; the tibia was the most frequently affected bone (n=13). The primary tumour that most frequently produced acrometastases in the lower limb was hypernephroma (19%). In the upper limb lung tumour was more frequent (25%). Eleven patients died (52%); 10 of them had concomitant multiple metastases. The mean survival was 42 months from the diagnosis of acrometastases.
ConclusionAcrometastases are more frequently seen in the lower extremities and the most frequent tumour was hypernephroma followed by lung. The treatment of acrometastases depends on the prognosis of the primary tumour, so a multidisciplinary approach is essential. The mean survival in our series did not imply a poorer prognosis for acrometastases, so it is feasible to consider surgical options such as wide resection and reconstruction. A unique acrometastases is a good prognosis signal.
Existe cierta contradicción en la literatura acerca del tumor primario que se asocia con más frecuencia a las acrometástasis, así como acerca de su pronóstico y tratamiento. El objetivo de nuestro trabajo es determinar la localización más frecuente de las acrometástasis, el tumor primario más frecuente según su localización y evaluar las opciones quirúrgicas en función de la supervivencia estimada.
MétodosHemos realizado un estudio retrospectivo de los pacientes diagnosticados de acrometástasis en nuestra institución. Se recogieron variables epidemiológicas, así como información acerca de tumor primario y número, localización, síntomas y tratamiento de las acrometástasis.
ResultadosSe revisaron 35 acrometástasis en 21 pacientes: 4 en miembros superiores y 31 en miembros inferiores, siendo la tibia el hueso más frecuentemente afectado (n=13). El tumor primario que con más frecuencia produce acrometástasis en miembros inferiores es el hipernefroma (19%); en los miembros superiores, sin embargo, el pulmón fue más frecuente (25%). Once pacientes fallecieron (52%), de los cuales 10 tenían metástasis en múltiples localizaciones. La media de supervivencia fue de 42 meses desde el diagnóstico de las acrometástasis.
ConclusiónLas acrometástasis se observan con más frecuencia en las extremidades inferiores, y el tumor primario más frecuente es el hipernefroma, seguido del de pulmón. El tratamiento de las acrometástasis depende del pronóstico del paciente, por lo que es esencial un abordaje multidisciplinar. La media de supervivencia en nuestra serie no implica un peor pronóstico de las acrometástasis, especialmente si son únicas, por lo que es factible considerar opciones quirúrgicas como la resección amplia y reconstrucción.
Bone metastases are the most common oncological process affecting the bones. The axial skeleton is more frequently affected than the appendicular skeleton. In all long bone involvement, metastases distal to the elbow and knee, or acrometastases, are the least frequent; comprising barely .1% and 7% of all bone metastases.1–5 In general, the more distal the bone, the less red bone marrow it contains, and therefore its involvement is more rare.6
The term “acrometastasis” is used indiscriminately in the literature to refer to “bone metastases in the distal regions of the extremities”,7 or in some cases is only used for metastases affecting the wrist or the bones of the hands and feet.8–11 However, most articles define acrometastasis expressly as bone metastasis distal to the elbow and knee,2,4,5,12–14 as in our case.
A primary tumour of the lung has been described in the literature as most commonly causing acrometastasis.1,2,4,9,12–15 However, a primary in the kidney is the most common in some series on lower limb acrometastasis.6,7 The tibia is the bone most frequently affected by acrometastasis.1,5
Involvement of the distal bones is considered a factor of poor prognosis, since it implies wide disease spread. The described mean survival is from 3 to 9 months from diagnosis of distal metastasis,3,6,7,9,13,14 with poor results for patients with no known primary tumour.7
The objective of this study was to determine the most frequent location of acrometastases, the primary tumour most commonly associated with metastases distal to the elbow and the knee, and to assess the different surgical options for acrometastasis according to estimated patient survival.
Material and methodsWe performed a retrospective study of patients with bone metastasis distal to the elbow and the knee, diagnosed or treated in our centre's department of orthopaedic and trauma surgery from 1988 to 2016, with a mean follow-up of 28 months (3–121 months). The treatment of each patient was individualised after the relevant multidisciplinary assessment.
Epidemiological variables and information were gathered about the primary tumour and the location of distal metastases, number of metastases, symptoms prior to diagnosis, time between diagnosis of primary tumour and diagnosis of distal metastasis, treatment of acrometastasis, and survival time from diagnosis of the distal metastasis.
Statistical analysis was performed using Fisher's exact test to compare proportions and Welch's test to compare means, with STATA 12.0 software, considering p<.05 as statistically significant.
ResultsOur series comprised 21 patients affected by bone metastases distal to the elbow and knee. Seven patients had unique metastases and 14 had multiple metastases, either bone or visceral. There were a total of 35 acrometastases: 4 in the upper limbs (2 in the radius, one in the ulna and one in the first metacarpal), and 31 in the lower limbs (13 in the tibia, 5 in the calcaneus, 5 in the wedges, 2 in the talus, one in the fibula, one in the scaphoid, and one in the cuboid).
The mean age of the patients was 48 (range 8–74 years), although the median was 55 years. The distribution by sex shows a clear male predominance: 14 men compared to 7 women.
The time between diagnosis of the primary tumour and diagnosis of acrometastasis was 41 months (range 0–150). Seven patients had no known primary tumour before diagnosis of acrometastasis; 6 of them had a unique metastasis (p=.001), i.e., we found a statistically significant relationship between the onset of disease with distal bone metastasis and it being a unique metastasis.
The main symptom reported by patients was pain (n=13, 62%); 3 of these patients had a pathological fracture (14%). Others consulted when they noticed a palpable mass (n=3, 14%). For the remainder (24%) diagnosis was by extension studies since, at the time of diagnosis, the patients were asymptomatic.
The most common primary tumours were of the kidney (n=3 patients; 4 of the 35 acrometastases) and the lung (n=3 patients; 3 of the 35 acrometastases). Prostate carcinoma, although only observed in 2 patients, was responsible for 12 of the 35 acrometastases. The other primary tumours are shown in Table 1. The primary that most frequently caused distal metastases in the lower limb was hypernephroma (19%), followed by adenocarcinoma of the lung (13%). In the upper limb, however, a lung primary was the most common (25%).
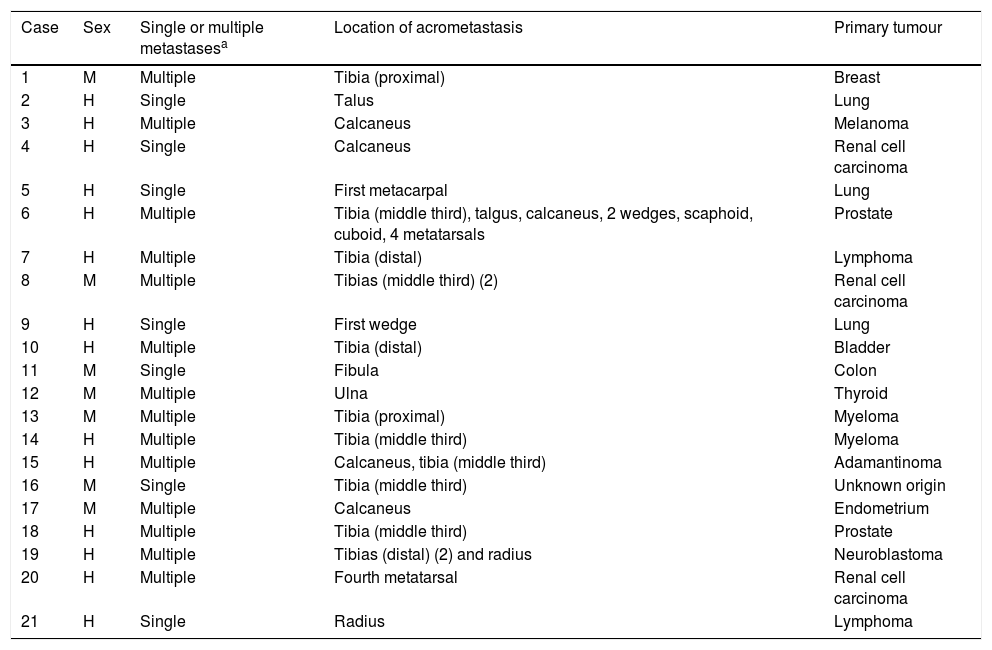
Patients with unique or multiple metastases, location of the acrometastases per case and primary tumours responsible for the acrometastases.
| Case | Sex | Single or multiple metastasesa | Location of acrometastasis | Primary tumour |
|---|---|---|---|---|
| 1 | M | Multiple | Tibia (proximal) | Breast |
| 2 | H | Single | Talus | Lung |
| 3 | H | Multiple | Calcaneus | Melanoma |
| 4 | H | Single | Calcaneus | Renal cell carcinoma |
| 5 | H | Single | First metacarpal | Lung |
| 6 | H | Multiple | Tibia (middle third), talgus, calcaneus, 2 wedges, scaphoid, cuboid, 4 metatarsals | Prostate |
| 7 | H | Multiple | Tibia (distal) | Lymphoma |
| 8 | M | Multiple | Tibias (middle third) (2) | Renal cell carcinoma |
| 9 | H | Single | First wedge | Lung |
| 10 | H | Multiple | Tibia (distal) | Bladder |
| 11 | M | Single | Fibula | Colon |
| 12 | M | Multiple | Ulna | Thyroid |
| 13 | M | Multiple | Tibia (proximal) | Myeloma |
| 14 | H | Multiple | Tibia (middle third) | Myeloma |
| 15 | H | Multiple | Calcaneus, tibia (middle third) | Adamantinoma |
| 16 | M | Single | Tibia (middle third) | Unknown origin |
| 17 | M | Multiple | Calcaneus | Endometrium |
| 18 | H | Multiple | Tibia (middle third) | Prostate |
| 19 | H | Multiple | Tibias (distal) (2) and radius | Neuroblastoma |
| 20 | H | Multiple | Fourth metatarsal | Renal cell carcinoma |
| 21 | H | Single | Radius | Lymphoma |
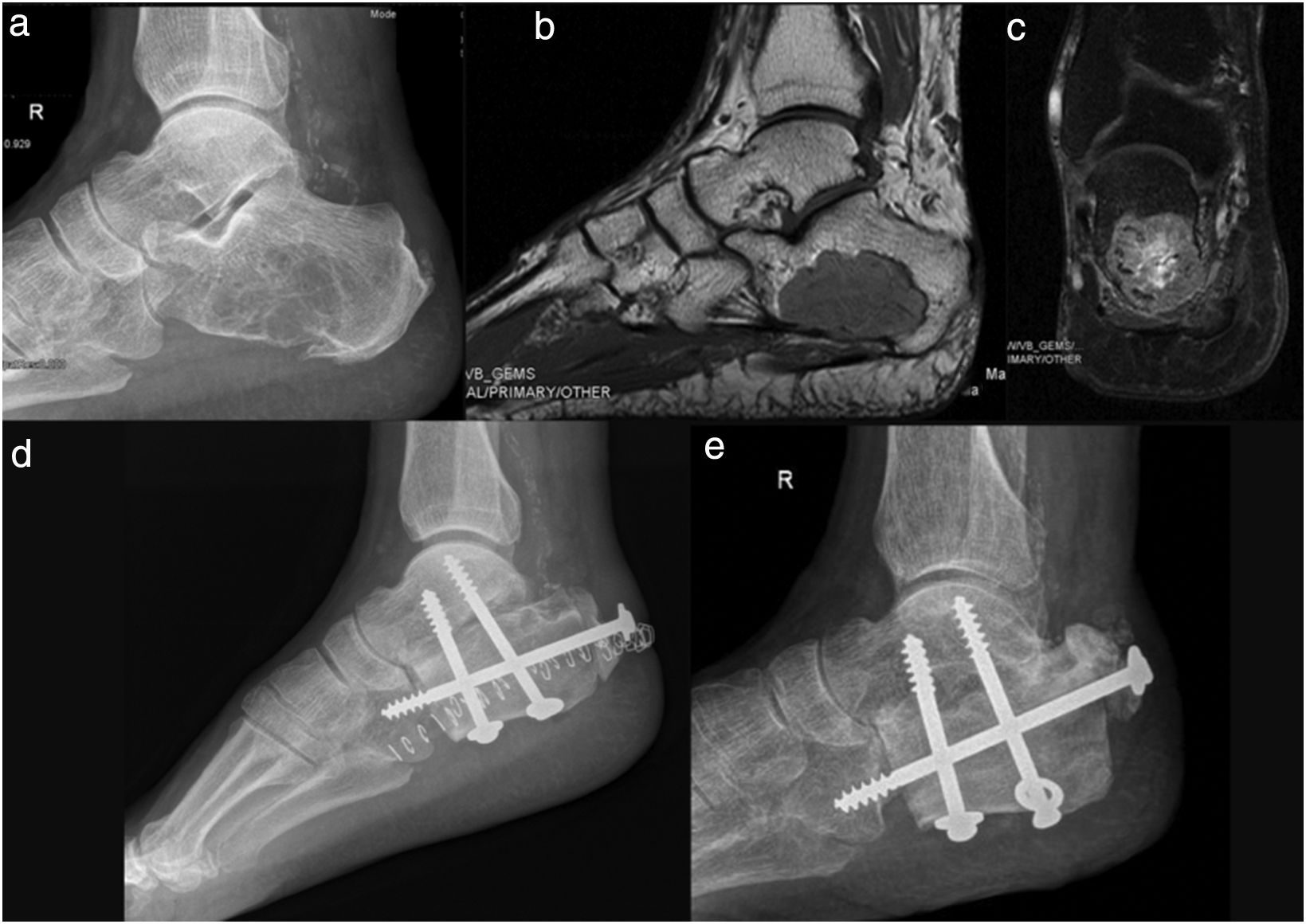
The treatment received by patients was individualised in each case according to the location of the metastasis and especially the prognosis of the primary tumour, the most frequent (n=10) being en bloc resection plus reconstruction with autologous or heterologous structural graft (Figs. 1 and 2). Other options were cryosurgery and cement fill (n=2) (Fig. 3), intramedullary nail fixation (n=1), amputation (n=1) and surgical abstention (n=7).
 and MRI sequences T1 (b) and T2 (c), of a unique metastasis of hypernephroma in the calcaneus, in a 58-year-old male, treated by en bloc resection and reconstruction with structural allograft; (d) 5 years after surgery (e) the patient is able to walk several kilometres a day without needing crutches.")
Plain X-ray (a) and MRI sequences T1 (b) and T2 (c), of a unique metastasis of hypernephroma in the calcaneus, in a 58-year-old male, treated by en bloc resection and reconstruction with structural allograft; (d) 5 years after surgery (e) the patient is able to walk several kilometres a day without needing crutches.
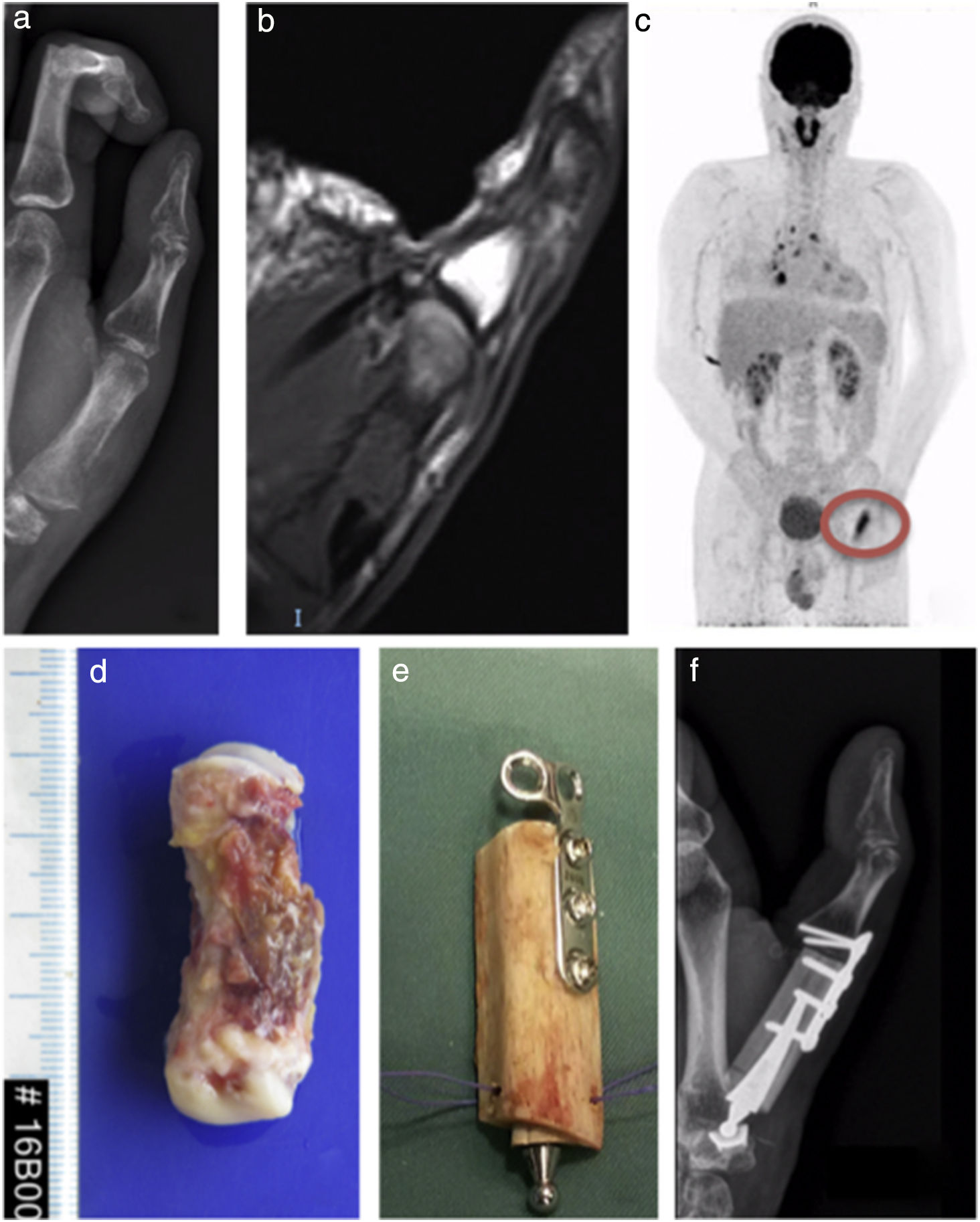
 and MRI (b) and PET (c) scans of a unique metastasis of lung adenocarcinoma in the first metacarpal, in a 35-year-old male, with no known primary prior to the diagnosis of metastasis, treated by en bloc resection (d) and reconstruction with autograft of the fibula (e and f). Two months afterwards the functionality of the hand is practically normal.")
Plain X-ray (a) and MRI (b) and PET (c) scans of a unique metastasis of lung adenocarcinoma in the first metacarpal, in a 35-year-old male, with no known primary prior to the diagnosis of metastasis, treated by en bloc resection (d) and reconstruction with autograft of the fibula (e and f). Two months afterwards the functionality of the hand is practically normal.
 and MRI (c) of a bone metastasis in the tibia, in a women of 45 years with breast cancer with multiple bone metastasis, treated with curettage, cryosurgery, cement fill and plate stabilisation (d); (e) 10 years after surgery the patient is able to undertake all her daily activities without outside help.")
Plain anteroposterior and lateral X-ray (a and b) and MRI (c) of a bone metastasis in the tibia, in a women of 45 years with breast cancer with multiple bone metastasis, treated with curettage, cryosurgery, cement fill and plate stabilisation (d); (e) 10 years after surgery the patient is able to undertake all her daily activities without outside help.
Of the 21 patients, 11 died (52.4%), 7 are alive with progressive disease, and 3 with disease in remission. Of the 11 patients who died, 10 had multiple metastases. The mean patient survival was 42 months (1–121 months), with no statistically significant differences between patients with unique metastases and those with multiple metastases (p=.9), although this might be due to the small sample size and the variety of patients included in the study.
DiscussionA diagnosis of metastasis distal to the elbow and knee poses a major challenge since, because it is so rare is often not considered, particularly when there is no known primary tumour.1,8,10,16 Acrometastases can be the first manifestation of an oncological process in up to 10% of cases.12,14 In our series this percentage was higher (33%), probably because we only included cases that had been diagnosed or treated in the orthopaedic and trauma surgery department, without considering cases that had not been referred to us because surgical treatment had not been advised for them.
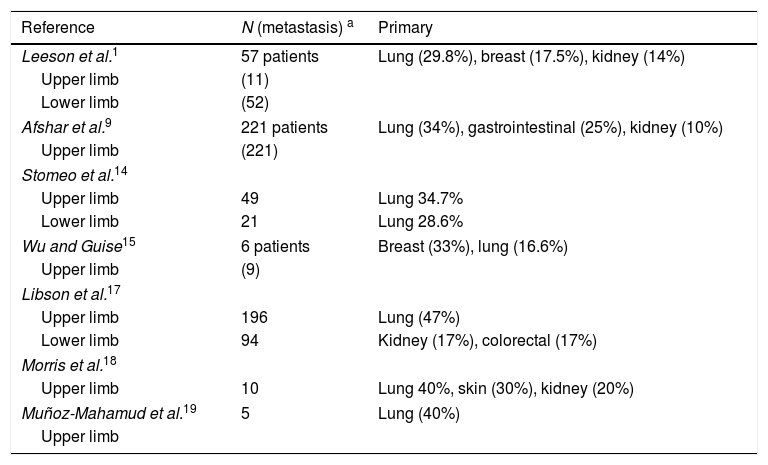
In our series, as in other published series, such as those of Baran,6 Lamarca,7 Mavrogenis12 and Libson,17 a location distal to the knee is more frequently associated with infradiaphragmatic tumours. Specifically, in our series, hypernephroma was responsible for 19% of the acrometastases of the lower limbs. However, metastases distal to the elbow are more often associated with supradiaphragmatic tumours, such as the lung or thyroid. Some publications that do not specify whether the acrometastasis affected an upper or a lower limb, assert that the primary tumour most often associated with acrometastasis is that of the lung (Table 2).
Literature references about primary tumours responsible for acrometastases.
| Reference | N (metastasis) a | Primary |
|---|---|---|
| Leeson et al.1 | 57 patients | Lung (29.8%), breast (17.5%), kidney (14%) |
| Upper limb | (11) | |
| Lower limb | (52) | |
| Afshar et al.9 | 221 patients | Lung (34%), gastrointestinal (25%), kidney (10%) |
| Upper limb | (221) | |
| Stomeo et al.14 | ||
| Upper limb | 49 | Lung 34.7% |
| Lower limb | 21 | Lung 28.6% |
| Wu and Guise15 | 6 patients | Breast (33%), lung (16.6%) |
| Upper limb | (9) | |
| Libson et al.17 | ||
| Upper limb | 196 | Lung (47%) |
| Lower limb | 94 | Kidney (17%), colorectal (17%) |
| Morris et al.18 | ||
| Upper limb | 10 | Lung 40%, skin (30%), kidney (20%) |
| Muñoz-Mahamud et al.19 | 5 | Lung (40%) |
| Upper limb | ||
The treatment of distal metastases depends on the prognosis of the primary tumour; therefore a multidisciplinary approach is essential. Surgical treatment has a place beyond prophylactic osteosynthesis or amputation. Although the literature refers to a poor prognosis, we chose en bloc resection plus reconstruction with graft for most of our patients thanks to the multidisciplinary approach taken. It is important to assess each case individually, according to the number and location of the metastasis, the response of the primary tumour to systemic treatments, the patient's general condition and the functionality that might be achieved with surgery. In short, in the case of unique metastases from hypernephroma, en bloc resection followed by reconstruction increases survival.20 Similarly, in the case of breast cancer, treatments should be planned that help not only to relieve pain, but also to reduce tumour load and preserve limb function, because these patients now have long survival.
Despite the fact that amputation is one of the most recommended surgical techniques in some series on bone metastases in the hands and feet,3,11,21 it is not the only surgical option. Although reasonable in the case of metastatic involvement of the phalanges, it can cause great functional alteration if there is more proximal involvement. Therefore, and bearing in mind the survival observed in our series, we do not consider amputation the technique of choice; more conservative surgical treatment could be justified, as long as they did not compromise the patient's prognosis, although studies are required with a greater number of cases to confirm this.
Bone metastases distal to the elbow and knee do not necessary mean a poor prognosis, especially when they are unique metastases. In our series, although 11 (52%) of the patients died, their mean survival was 42 months from diagnosis of the distal metastasis, and this is 6 times higher than that described in the literature. This is explained by the high number of unique metastases observed in our series, which indicates less disease spread.
Given that these metastases are so rare compared to axial bone metastases, the series we present is small, and therefore the evidence provided is limited. Furthermore, our series includes 2 cases with bone metastasis in the proximal tibia, which cannot be considered strictly acrometastases. Another limitation of the study to consider is that only cases diagnosed or treated in the orthopaedic and trauma surgery department were included, without considering the cases that the oncologist did not refer to our department, and therefore there might be a bias in estimating the survival.
Level of evidenceLevel of evidence IV.
Conflicts of interestThe authors have no conflict of interests to declare.
We would like to thank Dr Blanca Vázquez.
Please cite this article as: Machado V, San-Julian M. Pronóstico y tratamiento de las acrometástasis: estudio observacional de 35 casos tratados en un único centro. Rev Esp Cir Ortop Traumatol. 2019;63:49–55.
