



Dandy–Walker malformation (DWM) is an uncommon condition characterised by agenesis or hypoplasia of the cerebellar vermis, the cerebellar hemispheres, and cystic dilation of the fourth ventricle. There are very few records of asymptomatic adults with DWM. Hypotonia and motor and mental developmental delay, together with supratentorial hydrocephalus, malformation of the corpus callosum, and macrocephaly, appear in children.1,2 This case history describes arterial agenesis associated with abnormal brain embryogenesis.
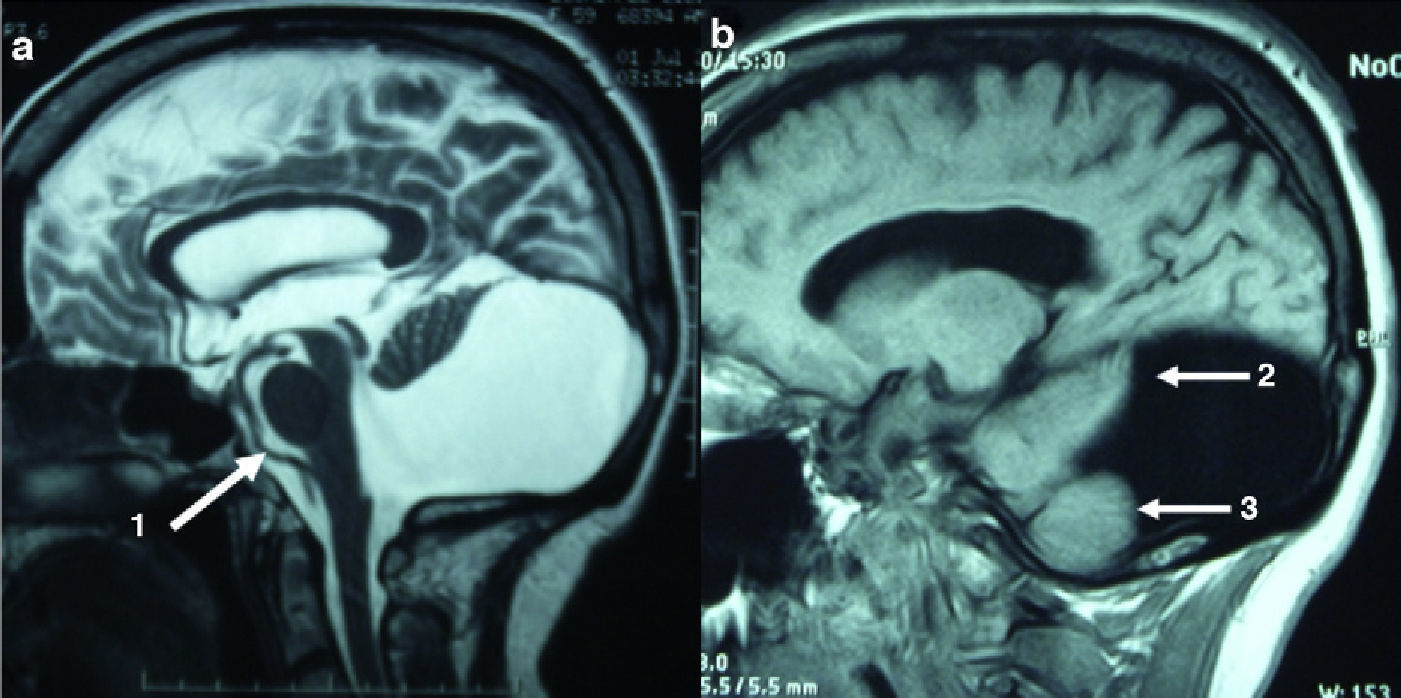
A 61-year-old female visited due to syncope. She had been taking medication for high blood pressure for 5years (25mg/day atenolol). Her medical history reported no motor or cognitive abnormalities. She was able to work and perform daily living activities normally. Blood tests, a 24-hour ECG, 24-hour blood pressure monitor test, a tilt test to measure response in terms of heart rate and blood pressure, and the EEG all delivered normal results. Findings from the neurological and cognitive tests were normal. Brain neuroimaging studies were performed. In Fig. 1, the sagittal brain MR image on the A side showed DWM. The supratentorial ventricles, cerebral cortex, corpus callosum, brainstem, and mesencephalic duct all appeared to be normal. On the medial slice of side A, Arrow 1 points to the entire length of the basilar artery. The cerebellar vermis is absent, and we see a small wing-shaped part of the upper cerebellum. In a paramedial slice on side B, arrows 2 and 3 indicate the anterior, superior, and inferior cerebellar parenchyma, respectively.
.")
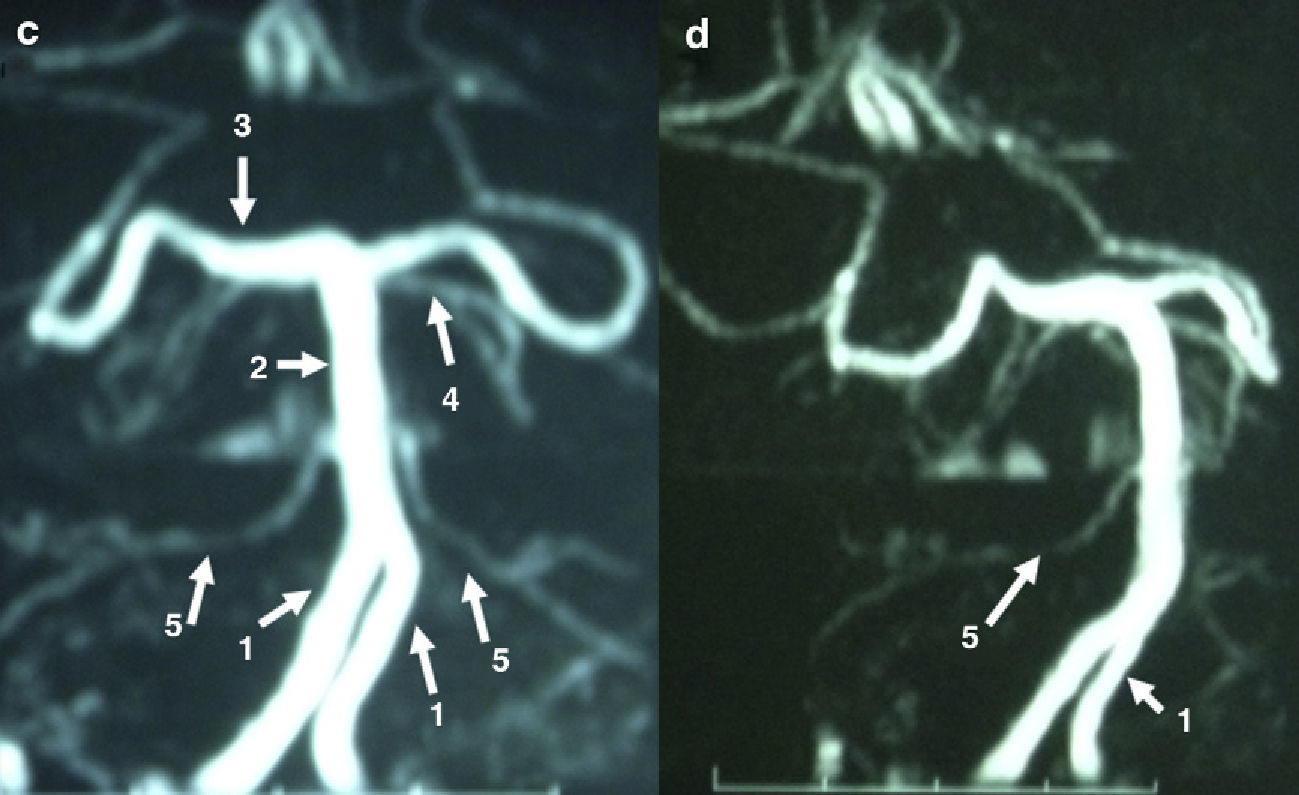
Angio-RM revealed that neck and supratentorial arteries were normal. Side C of Fig. 2 shows a frontal view, and side D, an oblique view, of the arteries of the posterior fossa. Arrow 1, along the final segment of the vertebral arteries, shows the lack of posterior inferior cerebellar arteries (PICA). Arrow 2 indicates the basilar trunk; Arrow 3 shows the posterior cerebral terminal branches; Arrow 4 shows the superior cerebellar colateral branches; and Arrow 5, the anterior inferior cerebellar arteries (AICA).
.")
One year after the syncopic episode, the patient had not experienced symptom recurrence, and was able to carry out daily activities normally.
Descriptions of DWM state that children hardly ever reach adulthood without clinical neurological signs of the syndrome. There are fewer than a dozen published accounts of asymptomatic adults, most of which describe females.
One article provides a case history of a woman with asymptomatic DWM who died of breast cancer at the age of 52. This was the first published anatomical pathology study in asymptomatic DWM. Macroscopic examination revealed hypoplasia of the vermis and both cerebellar hemispheres, cystic dilation of the fourth ventricle, and no supratentorial hydrocephalus. The external and medial walls of the cyst were formed by arachnoidal cells and internal ependymal cells. The cerebellar cortex had only 2 small areas with dysplasia. The cerebral cortex showed no neural losses, ectopias, vascular lesions, or degenerative lesions.3 In our case, the lack of other structural brain lesions concomitant with DWM could explain the patient's lack of symptoms in adulthood.
Other published articles on DWM present 4 women and 1 man aged 30–65years with a normal ability to engage in activities of daily life who rapidly developed symptoms compatible with vascular lesions, including headache, nausea, vomiting, ataxic gait, diplopia, and reduced awareness.4–8
As we are well aware that stroke complications may arise in DWM, we ordered an MR angiography study to assess large cervical and intracranial arteries. The most relevant finding was agenesis in both PICAs, and this coincided with the absence of the bilateral posterior and inferior areas of the cerebellum. Cerebellar parenchyma was present in the AICA and superior cerebellar arterial territories. Pascual-Castroviejo's study on cutaneous vascular malformations and hemangiomas with other concomitant abnormalities mentions DWM in the context of variations in the arteries of the brain.9
We wished to highlight the well-illustrated PICA agenesis in our patient. No published articles report bilateral absence of these arteries, but the abnormality may be linked to the same embryogenic defect found in regions of the cerebellum. It is very surprising that the patient has reached an advanced age without displaying specific symptoms.
Please cite this article as: Domínguez RO, et al. Agenesia de arterias cerebelosas postero-inferiores en adulto asintomático con malformación de Dandy Walker. Neurología. 2012; 27:445–6.
