





Patients with major depressive disorder (MDD) have altered learning rates for rewards and losses in non-social learning paradigms. However, it is not well understood whether the ability to learn from social interactions is altered in MDD patients. Using reinforcement learning during the repeated Trust Game (rTG), we investigated how MDD patients learn to trust newly-met partners in MDD patients.
MethodSixty-eight MDD patients and fifty-four controls each played as ‘investor’ and interacted with ten different partners. We manipulated both the level of trustworthiness by varying the chance of reciprocity (10, 30, 50, 70 and 90%) and reputation disclosure, where partners’ reputation was either pre-disclosed or hidden.
ResultsOur reinforcement learning model revealed that MDD patients had significantly higher learning rates for losses than the controls in both the reputation disclosure and non-disclosure condition. The difference was larger when reputation was not disclosed than disclosed. We observed no difference in learning rates for gains in either condition.
ConclusionsOur findings highlight that abnormal learning for losses underlies the social learning process in MDD patients. This abnormality is higher when situational unpredictability is high versus low. Our findings provide novel insights into social rehabilitation of MDD.
Major depressive disorder (MDD) is one of the most serious mental disorders worldwide (Bueno-Notivol et al., 2021). MDD patients often suffer from impaired social functioning (Fernández-Theoduloz et al., 2019; Kupferberg et al., 2016). This is marked by decreased time and efforts engaging in social activities, and decreased quantity and quality of social interactions (Pagnini et al., 2019).
Successful social interactions require one to flexibly adjust behavioral strategies according to predictions of others’ attitudes and potential future responses (Van Overwalle et al., 2020). The role of learning is thus implicitly entailed in successful social interactions. While a large body of work has consistently found an altered learning pattern among MDD patients, including abnormalities in anticipation, prediction error coding and outcome feedback stages on the behavioral (Gradin et al., 2011; Kumar et al., 2008) and neurological level (Gradin et al., 2011; Lawson et al., 2017) in the non-social contexts, whether the ability to learn from social outcomes is altered among MDD patients remains unclear. A few studies have made groundbreaking steps to investigate the abnormalities in learning towards social stimuli among MDD patients (Frey, Frank, & McCabe, 2021; Frey & McCabe, 2020). However, a critical limitation in both studies is that they investigated patients’ altered learning pattern within a “stimuli-feedback” non-social interactional learning context, which essentially requires participants to learn the probabilistic connection between various stimuli and favorable versus non-favorable social feedbacks indicated by facial expressions. These paradigms lack real social interactions. Therefore, it is necessary to investigate patients’ abnormal social learning pattern within a social interactional context that represents real-life experience.
Economic games are increasingly used to study social learning abnormalities among patients with various psychiatric disorders and brain lesions (Brüne, von Hein, Claassen, Hoffmann, & Saft, 2021; Doppelhofer et al., 2021; Robson et al., 2020; Rosenberger et al., 2019; Serra, 2021). The current study introduces an economic game paradigm, the repeated Trust Game (rTG), to investigate abnormal social learning among MDD patients and how it relates to abnormal trust behaviors. Trust is an important aspect of social life, the foundation of corporation and a prerequisite for resource exchange (Weiss et al., 2021). MDD patients have diminished trust and poor help-seeking behavior towards others (Cobb-Clark, Dahmann, & Kettlewell, 2022). rTG quantifies the extent to which investors trust the partners in terms of the amount of investment in each round (Van Den Akker et al., 2020). Investors adjust their expected valuation of trust and distrust decisions based on their observations of the partners’ past reciprocity and betrayal behaviors (Attanasi et al., 2019). rTG is a paradigm with high ecological validity, which captures the social embeddedness of individuals whose decisions influence one another (Alós-Ferrer & Farolfi, 2019).
Reinforcement learning (RL) has been widely applied to describe how individuals learn from feedback of actions to plan future actions that maximize rewards (Olsson et al., 2020; Wagner & Rescorla, 1972). There is also a growing trend in social neuroscience to employ RL to depict the learning abnormalities of patients with brain lesion and psychiatric disorders in various contexts (Na et al., 2022; Rosenblau et al., 2021; Zhang et al., 2020). Due to the inherent consistency between trust learning in the rTG and the Rescorla-Wagner (R-W) RL process, the R-W RL model and its variations have been applied to quantify the trust learning process in the rTG among healthy individuals (Chang et al., 2010; Huys et al., 2011; Montague, 2018; Montague et al., 2012; Radell et al., 2016; Stephan & Mathys, 2014; van Honk et al., 2013)
Building upon this solid progress in healthy populations, the current study extends the RL modeling technique to clinical populations. We seek to compare the differences in the RL parameters in the rTG between the MDD patients and controls in different situations. We do so by manipulating two key situational characteristics: (1) whether information about trustees’ reputation is disclosed to participants before the game starts, and (2) trustees’ chance of reciprocity (10, 30, 50, 70 and 90%). No studies to date have made direct comparison on learning parameters between the MDD and healthy populations in a social context. However, past studies have found that MDD patients had a hyposensitivity to reward and hypersensitivity to punishment of both social and non-social stimuli in the Incentive Delay Task and Probabilistic Reward Task (Gradin et al., 2011; Kerestes et al., 2014; Kumar et al., 2008; Pizzagalli, 2014). These abnormalities were operationalized by a suboptimal learning rate for reward (Kunisato et al., 2012), enhanced learning rate for punishment (Byrne et al., 2016) and suboptimal exploration (Kunisato et al., 2012). Similarly, in the social interactional context, we hypothesize that MDD patients will have a generally lower level of trust placed on others (H1), impaired learning for gains (H2) and increased learning for losses (H3). Particularly, in our task design, we manipulated situational unpredictability, which is high when reputation information is not disclosed to participants (versus disclosed), and when partners’ behavior is random (versus consistent). A large body of studies have shown that there was a larger negative perceptual bias among MDD patients towards ambiguous stimuli (i.e. high situational unpredictability) as compared to positive or negative stimuli (i.e. low situational unpredictability) (Beevers et al., 2009; Münkler et al., 2015). Thus, we further predict that this altered pattern of learning would be more pronounced when situational unpredictability is high versus low (H4).
Material and methodsParticipantsSeventy unmedicated major depressive disorder (MDD) patients were recruited from the Department of Psychiatry of the Beijing Anding Hospital, Capital Medical University. Two patients quitted in the midst, resulting in 68 MDD patients (mean age (SD) = 27.88 (6.44); 63% female). All patients were screened on established inclusion and exclusion criteria by trained psychiatrists. All participants (1) met the diagnosis criteria of major depressive episodes according to the Chinese version of the Mini-International Neuropsychiatric Interview (M.I.N.I.) 5.0.0 (Sheehan et al., 2006), a short structured clinical interview in accordance with DSM-IV, (2) did not take any antidepressant or other antipsychotic medication two weeks before the experiment, (3) between 18 and 45 years of age, (4) had at least 9 years of education, (5) right-handed, (6) mother language was mandarin. Patients who had any preexisting or concurrent co-morbid primary diagnosis that met the DSM-IV criteria for any Axis I disorder other than MDD (e.g. schizophrenia or schizoaffective disorders) were excluded from the study. The additional exclusion criteria were listed in the Supplementary Material S1.
Fifty-five controls were recruited by bulletin board postings in nearby communities and universities. Three participants were excluded due to drop-out in the midst of the experiment, resulting in fifty-two participants in the control group (mean age (SD) = 26.10 (5.10); 54% female). The controls did not have current psychopathology screened by the Chinese version of M.I.N.I. 5.0.0 (Sheehan et al., 2006) or self-reported histories of past psychopathologies. The controls met the same additional exclusion criteria as the MDD patients and no family history of major psychiatric or neurological illness in first-degree relatives.
All participants in the current study also completed an Ultimatum Game (UG), which is reported in another study (Jin et al., 2022). The demographic information, clinical and neurocognitive assessments were also reported in that study (Jin et al., 2022).
Clinical symptoms assessmentsWe administered the Chinese translated version of the 17-item Hamilton Rating Scale for Depression (HAMD-17) (Hamilton, 1960) and the Hamilton Rating Scale for Anxiety (HAMA) (Hamilton, 1959) to MDD patients to assess the severity of depression and anxiety. We also administered the Chinese translated version of two self-report measurements namely the Patient Health Questionnaire-9 (PHQ-9) (Spitzer et al., 1999) and the Generalized Anxiety Disorder-7 (GAD-7) (Spitzer et al., 2006) to both groups of participants. Reliability and validity of the translated scales were shown in the Supplementary Material S2.
Neurocognitive assessmentsTo exclude the potential influences of neurocognitive deficits on trust building behaviors in the rTG, we assessed basic aspects of neurocognition by subtests from WAIS-IV (Wechsler Adult Intelligence Test) (Wechsler, 2008): Digit Symbol Substitution Test (processing speed), Digit Span (working memory), Vocabulary (verbal comprehension), and Block Design (perceptual reasoning). In addition, executive functions such as fluency, control and problem solving were measured by a Verbal Fluency Test (Animals) and the Continuous Performance Test (CPT) (Lee et al., 2018).
The repeated trust gameWe revised the rTG (Fouragnan, 2013) by manipulating partners’ reputation disclosure and chance of reciprocity, where participants played as investors all the time. Participants were told that they would be matched with multiple anonymous real online players (trustees) and interacted with each of them for multiple repeated rounds. Behaviors of trustees were actually generated by the computer program. The experiment consisted of two blocks (order-randomized) in which the reputation information was disclosed versus not disclosed to participants in the partner matching phase before the game started. In each block, all participants were matched with 5 partners (order-randomized). In the reputation disclosure block, the reputation information of each partner was displayed to participants in the form of star-ratings in the partner-matching phase. 1, 3, 5, 7 and 9 star-rating denoted 10, 30, 50, 70 and 90% chance of reciprocation in terms of returning some money after receiving an investment, respectively. In the reputation non-disclosure block, the reputation information of the 5 partners was not disclosed such that participants had to infer the partners’ trustworthiness level only via interactions in the game. The actual chance of reciprocity for partners in the reputation non-disclosure block was 10, 30, 50, 70 or 90%. In this way, the actual behaviors of partners in the two conditions were identical.
Participants played 20 consecutive rounds with the same partner before matching to the next partner. At the beginning of each round, participants and their partner were each given 2 yuan. Participants were asked to choose between making a 2-yuan investment or keeping all the money to her/himself. If they made an investment, the amount would be multiplied by 3 and therefore their partner would receive 6 yuan. Their partner would choose between (1) returning 4 yuan such that each player got 4 yuan, or (2) keeping all 6 yuan to her/himself, such that the partner got all 8 yuan and the participant got nothing. The partners’ chance of reciprocity was manipulated as mentioned above. If participants did not make an investment, the round would end directly without any feedback about reciprocity, and participants and their partner would each get 2 yuan. The expected value (EV) for not making an investment is always 2, whereas the EV for investment is 4*p, where p is partners’ chance of reciprocity. The procedure is shown in the flow diagram (Fig. 1).

The procedure of the rTG when participants were matched to a new partner. Participants were matched to a new partner whose name was represented by alphanumeric codes. In the reputation disclosure condition, the partner's star rating was presented at the bottom. In each round of the 20 consecutive rounds, participants were asked to choose between making an investment versus keeping the money. After the decision had been made and an additional random waiting period, feedback of whether the partner returned money would be shown. After the total of 20 rounds ended, participants rated on the perceived trustworthiness of their partner ranging from 1 = very untrustworthy to 10 = very trustworthy.
We measured interpersonal trust tendencies (Rotter, 1967), harm avoidance (Cloninger, 1987) and the Temporal Experience of Pleasure (TEPS) (Chan et al., 2012). The measurement details are shown in the Supplementary Material S2.
Analytic strategiesTrust decisionsWe used a generalized linear mixed effects model with random intercepts to investigate the main effects and interactions of subject type, partner's trustworthiness level and reputation disclosure on the binary outcome of investment or not. We did a supplementary linear mixed effects model (LME) to investigate the above predictors’ influence on the average rate of investment across trials (Supplementary Material S5).
Computational modelsWe used reinforcement learning models to capture the altered trust learning process in the patient group compared to the control group. We formalized the process into 4 candidate models: (1) Rescorla-Wagner (RW) model: the baseline Rescorla-Wagner (R-W) reinforcement learning model; (2) Gain-Loss (GL) model: an R-W reinforcement learning model with differentiation of learning rates for gains and losses; (3) Trustworthiness (TW) model: a model-based RL model with perception of trustworthiness level incorporated in the learning process; (4) Trustworthiness Gain-Loss (TW-GL) model: a model-based RL model with perception of trustworthiness level incorporated in the learning process and with differentiation of learning rates for gains and losses. Details of model formalism and parameter specification are shown in the Supplementary Material S3.
Model comparison and selectionModel selection was based on minimizing the Akaike Information Criterion (AIC) (Akaike, 1983). Nonparametric Wilcoxon signed-rank tests on AIC were conducted to select the optimal model for the patient and the controls group, respectively. As models vary on the number of parameters, we also conducted model selection on Bayesian Information Criterion (BIC) which is more stringent on correcting for the number of parameters (Lorah & Womack, 2019).
Parameter estimationParameter estimation was performed for each participant in the reputation non-disclosure and reputation disclosure condition respectively within the optimal model. Parameters were estimated by maximizing the total log likelihood of the observed choices made by the investor on a trial-to-trial basis using the fmincon function in Matlab. To avoid model convergence on local minima, we selected 100 random start locations with the rmsearch function (Fareri et al., 2015).
Parameter recoveryTo test the reliability of parameter estimation for each participant, we performed parameter recovery (Fareri et al., 2015). The detailed procedures were shown in the Supplementary Material S4.
Between-group comparison of parametersWe conducted mixed ANOVAs to examine the main effect and interaction of reputation disclosure and subject type on each parameter in the optimal candidate model.
Cross validation using the hierarchical Bayesian approachWe conducted cross-validation of results using the Hierarchical Bayesian estimator in Rstan. The Hierarchical Bayesian approach simultaneously estimates group-level and individual-level parameters, thus enables us to compare posterior distributions of group-level parameters (Tso et al., 2021). Detailed modeling procedure is introduced in Supplementary Material S8.
Comparison of goodness of fit with the Bayesian model classTo compare the goodness of fit between the RL and the Bayesian model class, we built two candidate models from the Bayesian class, namely the Bayesian Inference model adapted from Kreis et al. (2022) and the Bayesian Observer Model adapted from Rupprechter et al. (2018). Modeling details are presented in Supplementary Material S9.
External validity of parametersWe calculated correlations between external criteria (e.g. PHQ-9, GAD-7, harm avoidance, and TEPS) and parameters in the optimal candidate model to examine the external validity of parameters.
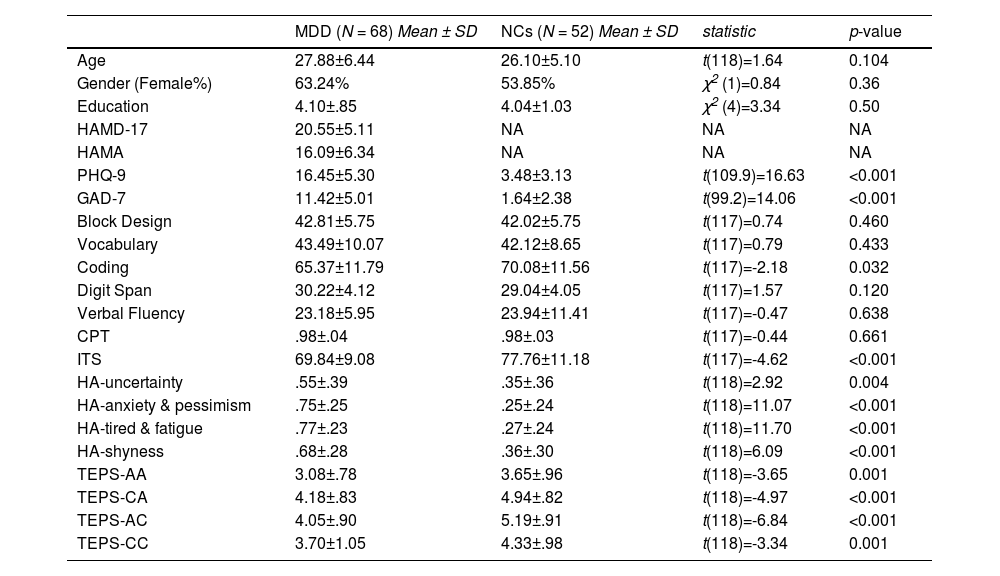
ResultsDemographics, clinical characteristics, neurocognitive and psychological assessmentsThere were no significant differences in gender composition, age, and educational level between the patient group and the control group (Table 1). The self-rated depression and anxiety symptoms (i.e. PHQ-9 and GAD-7) were significantly higher for the MDD patients than the controls. The two groups had no significant differences in neurocognitive measures except for the coding task, where MDD patients were slower than controls. The MDD patients scored significantly lower than the controls on interpersonal trust and all four dimensions of TEPS, whereas the MDD patients scored significantly higher than the controls on all four dimensions of harm avoidance.
Demographic, clinical symptoms, neurocognition and psychological assessments.
Abbreviations: ITS, Interpersonal trust scale; HA-uncertainty, Harm avoidance-afraid of uncertainty; HA-anxiety & pessimism, Harm avoidance-expected anxiety and pessimism; HA-tired & fatigue, Harm avoidance-easily getting tired and fatigue; HA-shyness, Harm avoidance-afraid of strangers; TEPS, temporal experience of pleasure; AA, Abstract anticipatory; CA, Contextual anticipatory; AC, Abstract consummatory; CC, Contextual consummatory.
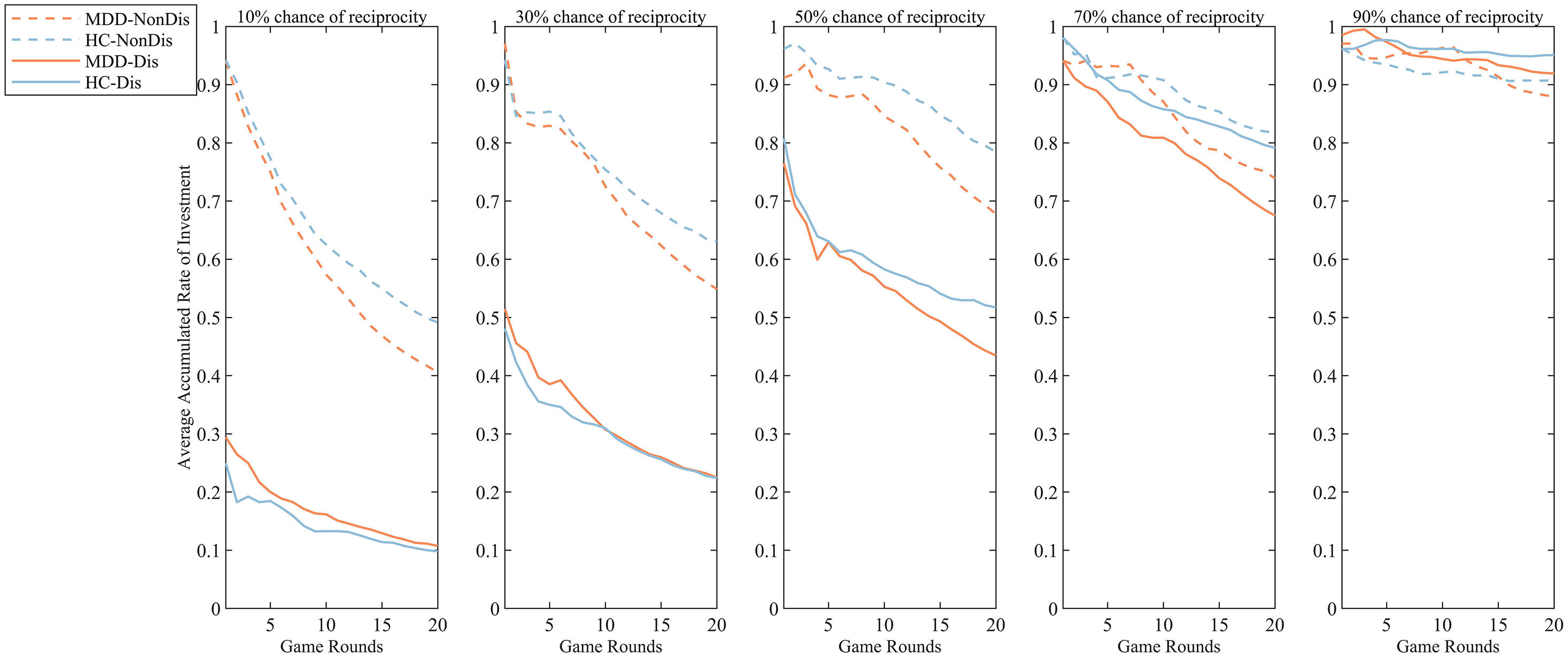
Fig 2 shows the average cumulative rate of investment in the 20 rounds, when participants were matched with trustees exhibiting various chances of reciprocity in the reputation disclosure and non-disclosure condition.
 and reputation disclosure condition (Dis).")
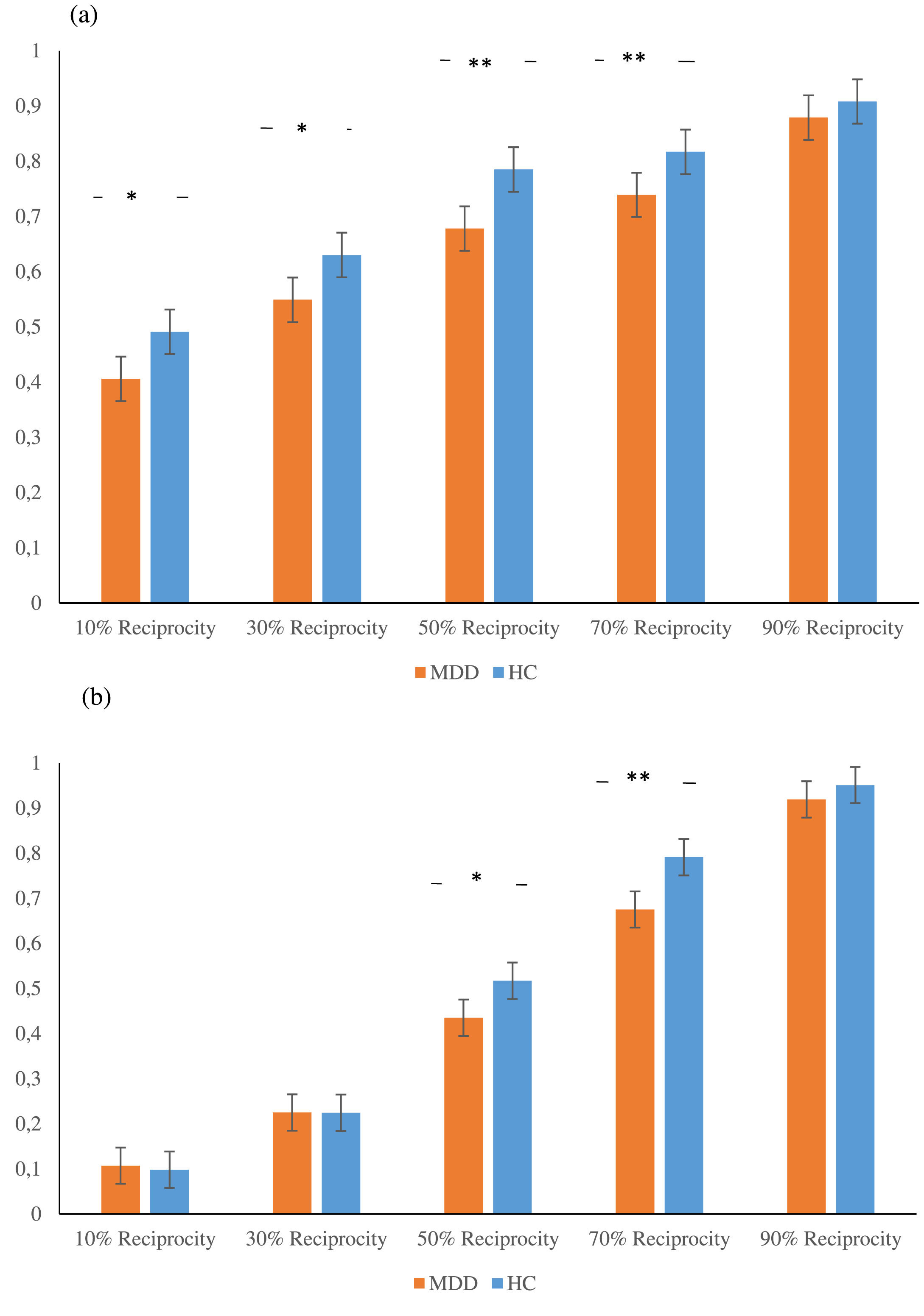
We used the generalized linear mixed effects model to examine the effect of subject type, partners’ level of reciprocity and reputation disclosure on the binary investment outcome in each trial. We found that MDD patients generally made fewer investments than the controls (χ2(1) = 5.52, p = .019). We found a larger between-group difference in trust behaviors when situational unpredictability was high versus low, backed up by several findings. Specifically, there was a significant difference in trust behaviors between the two groups in the reputation non-disclosure condition (exp (B) = 1.59, SE = 0.17, z = 2.81, p = .005), whereas the difference was not significant in the reputation disclosure condition (exp (B) = 1.35, SE = 0.17, z = 1.77, p = .076). Having a close look on the three-way interaction, we found that in the reputation non-disclosure condition, the two groups differed in the average rate of investment when they interacted with trustees with 10% (exp (B) = 1.50, SE = 0.18, z = 2.22, p = .026), 30% (exp (B) = 1.49, SE = 0.18, z = 2.20, p = .028), 50% (exp (B) = 1.89, SE = 0.19, z = 3.39, p < .001) and 70% (exp (B) = 1.70, SE = 0.19, z = 2.79, p = .005) chance of reciprocity; in the reputation disclosure condition, the two groups differed in the average rate of investment when they interacted with trustees with 50% (exp (B) = 1.48, SE = 0.18, z = 2.15, p = 0.032) and 70% (exp (B) = 2.01, SE = 0.19, z = 3.70, p < .001) chance of reciprocity (Fig. 3). We did a supplementary LME model which specified the average rate of investment across trials as the dependent variable to prove the robustness of our generalized linear mixed effects results. Detailed statistics are shown in the Supplementary Material S5.
 In the reputation non-disclosure condition, the two-way interaction between trustees’ chance of reciprocity and subject type on the average rate of investment. (b) In the reputation disclosure condition, the two-way interaction between trustees’ chance of reciprocity and subject type on the average rate of investment.")
The three-way interaction plot of the average rate of investment. (a) In the reputation non-disclosure condition, the two-way interaction between trustees’ chance of reciprocity and subject type on the average rate of investment. (b) In the reputation disclosure condition, the two-way interaction between trustees’ chance of reciprocity and subject type on the average rate of investment.
The AIC, BIC and the parsimony principle all favored the GL model in all experimental condition for each group of participants. Model recovery suggested that simulations from the GL model can capture key features of the original investment behavior. Parameter recovery supported a reliable estimation of parameters in all conditions for each group of participants. Detailed model selection, model recovery and parameter recovery procedures are shown in Supplementary Material S6.
Parameter estimationMean and standard deviation of parameter estimations for the patients and the controls in the reputation disclosure and non-disclosure conditions in the best model are presented in the Table 2.
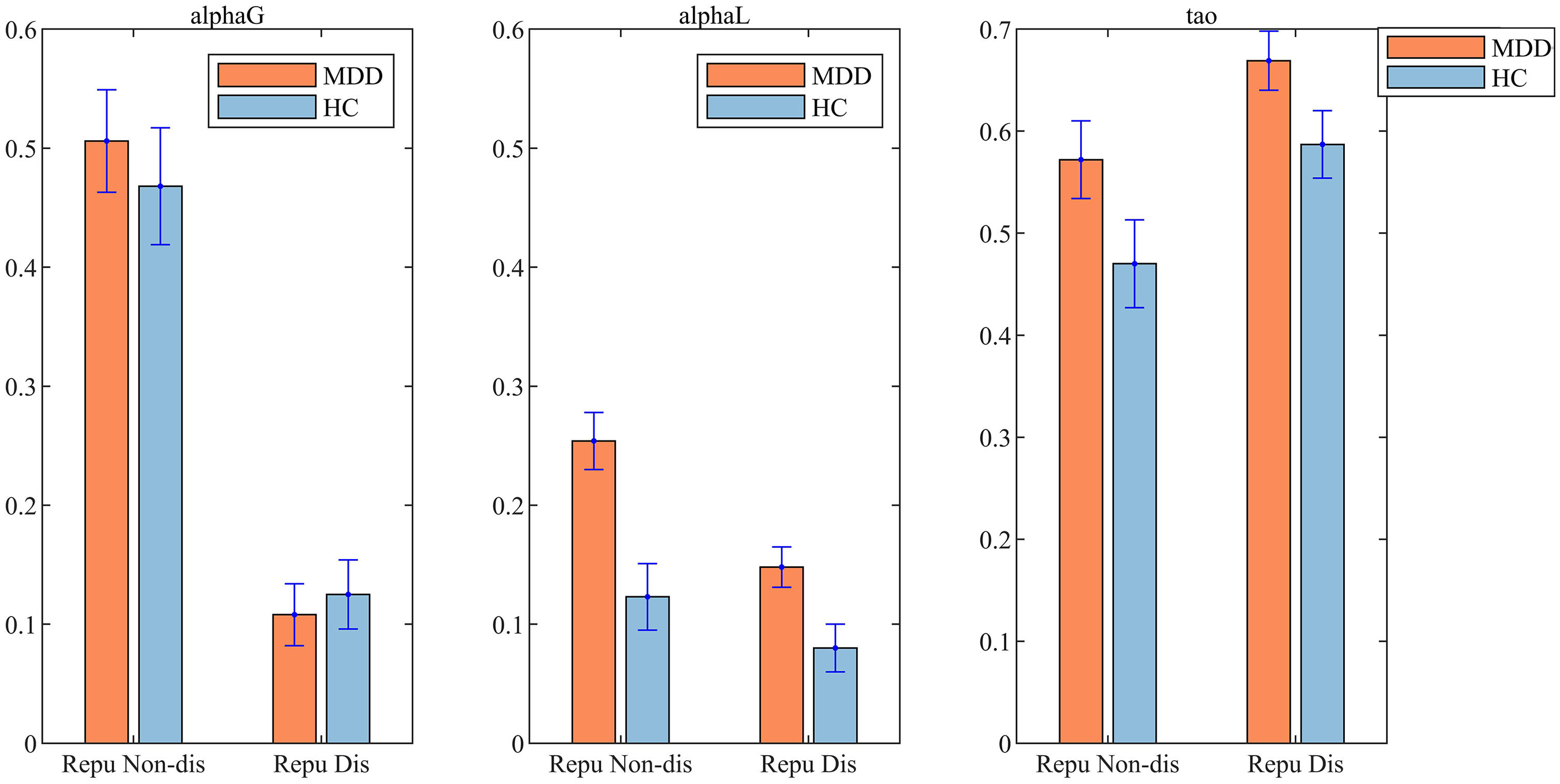
A mixed ANOVA on αG revealed a significant main effect of reputation disclosure (F(1,118) =116.22, p < 0.001, partial η2=0.50). Post-hoc analysis suggested that αG in the reputation non-disclosure condition was significantly higher than in the reputation disclosure condition (mean (SE) =0.37 (0.04), t (118) =10.88, p < 0.001, Cohen's d = 0.99) (Fig. 4). No other effects were significant.

A mixed ANOVA on αL revealed a non-significant interaction between subject type and reputation disclosure (F(1,118) =2.31, p = 0.132, partial η2=0.02), a significant main effect of subject type (F(1,118) =17.38, p < 0.001, partial η2=0.13), and a significant main effect of reputation disclosure (F(1,118) =12.32, p = 0.001, partial η2=0.10). Driven by our hypothesis that a larger discrepancy of learning rate should exist between MDD and NC when reputation was not disclosed, we conducted a simple effect analysis. Simple effect analysis suggested that in the reputation non-disclosure condition, the αL for MDD patients was significantly higher than for controls (mean (SE) =0.13 (0.04), t (118) =3.57, p < 0.001, Cohen's d = 0.66). In the reputation disclosure condition, the αL of MDD patients was significantly higher than for controls (mean (SE) =0.07 (0.03), t (118) =2.58, p = 0.012, Cohen's d = 0.48). Post-hoc analysis suggested that αL in the reputation non-disclosure condition was significantly higher than in the reputation disclosure condition (mean (SE) =0.08 (0.02), t (118) =3.57, p = 0.001, Cohen's d = 0.33). The αL for the patient group was significantly higher than for the controls (mean (SE) =0.10 (0.02), t (118) =4.13, p < 0.001, Cohen's d = 0.76) (Fig. 4).
A mixed ANOVA on τ revealed a significant main effect of subject type (F(1,118) =4.57, p = 0.035, partial η2=0.04), and a significant main effect of reputation disclosure (F(1,118) =11.28, p = 0.001, partial η2=0.09). Post-hoc analysis suggested that τ among the MDD patients was significantly higher than among the controls (mean (SE) =0.09 (0.04), t (118) =2.15, p = 0.035, Cohen's d = 0.40). τ in the reputation disclosure condition was significantly higher than in the reputation non-disclosure condition (mean (SE) =0.10 (0.03), t (118) =3.40, p = 0.001, Cohen's d = 0.31) (Fig. 4).
Cross validation using the hierarchical Bayesian approachTo test the robustness of our results, we conducted cross validation using the Hierarchical Bayesian approach. Consistent with the above mixed ANOVA analyses, we found MDD and HC credibly differed in the learning rate for losses in both experimental conditions when reputation was given v.s. not given. We also found a credibly larger difference between MDD and HC when reputation was not given than given in the learning rate for losses in both the TWGL and the GL model (Supplementary Material S8). We did not find stable between-group differences in the learning rate for gains.
Comparison of goodness of fit with the Bayesian model classThe Bayesian model class did not provide better goodness of fit than the RL class (Supplementary Material S9), indicating that the RL models might be more suitable for depicting the social learning process in the rTG.
External validityWe computed the Pearson correlation between self-rated questionnaires and estimated parameters across participants using a Bonferroni correction (p < .05) for multiple comparisons (uncorrected p < .005). In the reputation non-disclosure condition, αL was positively correlated with PHQ-9 (r = 0.34, uncorrected p < .001), three dimensions of harm avoidance (for expected anxiety and pessimism: r = 0.32, uncorrected p < .001; for easily getting tired or fatigue: r = 0.31, uncorrected p=.001; for fear of strangers: r = 0.28, uncorrected p=.002), and TEPS-consummatory contextual (r=-0.26, uncorrected p=.004). No other correlations passed the multiple comparisons correction threshold. Among of them, αL in the reputation non-disclosure condition was also positively correlated with GAD-7, and αL in the reputation disclosure condition was both positively correlated with PHQ-9 (r = 0.22, uncorrected p=.016) and GAD-7 (r = 0.20, uncorrected p=.033) but did not pass the multiple comparisons correction threshold.
DiscussionThe current study found that MDD patients generally made fewer investments than controls in the rTG, which proves our hypothesis H1 and is consistent with a large body of studies demonstrating generally lower levels of trust towards others among MDD patients (Clark et al., 2013). More importantly, we found altered social learning process underlying trust building in MDD patients using the reinforcement learning modeling technique. More importantly, we found higher learning rate for losses among MDD patients, which supports hypothesis H3. Such between-group discrepancy was larger in the reputation non-disclosure condition than reputation disclosure condition, which supports hypothesis H4.
Optimal model selectionModel comparison within the MLE estimator favored the model-free GL model over the other candidate models. Our optimal model is consistent with recent studies (Fareri et al., 2012; Radell et al., 2016), which also favored the GL model. However, our optimal model was inconsistent with some other studies (Chang et al., 2010; Fareri et al., 2015), which favors model-based models. This inconsistency could partially be attributed to differences in experimental design. Participants interacting with close others in Fareri et al. (2015) might involve stronger appraisal of social value (i.e. trustworthiness) and hence, behaviors might be better fitted by model-based social value models. Chang et al. (2010) manipulated partners’ level of trustworthiness by facial trustworthiness shown in photos as opposed to star ratings in our study, which might elicit different psychological processes.
Parameter comparisonComparison of parameter estimates shows a higher learning rate for losses, but not gains, in the patient group in both the reputation non-disclosure and the reputation disclosure condition. These results were cross-validated with the Hierarchical Bayesian approach. Our findings support hypothesis H3 but does not support H2. We detected an abnormal punishment learning but did not detect an abnormal reward learning among MDD patients. The higher learning rate for losses in our study is consistent with a vast body of studies which found hypersensitivity to punishment feedback among MDD patients in various social and non-social reinforcement learning paradigms (Dombrovski et al., 2013; Kumar et al., 2008). We did not find differences in the learning rate for gains in the reputation non-disclosure condition between MDD patients and HC, which is consistent with some previous studies. Huys et al. (2013) found no difference in the rate for learning of reward prediction signals among depressive individuals in the probablistic reward learning task, although dopamine manipulation among healthy individuals affected the learning rate. However, some other studies show an impaired learning rate for reward (Kunisato et al., 2012). Kumar et al. (2008) found reduced reward prediction error signals in the ventral striatum and hippocmpus among MDD patients using a non-social probablistic learning paradigm. A possible explanation is that hypersensitized punishment learning is the driving force behind interpersonal trust learning towards a stranger. Another possibility is that the moderate correlation between original and recovered learning rates for gains in the parameter recovery might potentially lead to the occurrence of Type-II error, i.e. failing to detect the between-group difference in the learning rate for gains between MDD patients and HC. To our knowledge, our study is the first to compute and compare the learning rate for gains and losses among MDD patients and healthy individuals in a social learning context. Although we did not find statistically significant differences in the learning rate for gains between the MDD patients and controls in the reputation disclosure condition, descriptive statistics on means revealed a lower average learning rate for gains among the MDD patients than the controls. Future studies could enhance parameter recovery by enlarging the number of valid trials, and furthermore investigate how the altered learning rate for gains impedes trust learning in MDD patients.
Our study showed differences in exploration versus exploitation tendency between patients and controls. There was a higher τ in the patient group than the control group. This implies the decision behavior of MDD patients was less associated with utility estimation compared to the controls. The attenuated association between perceived value of behavioral outcomes and actual behaviors among MDD patients was consistent with our previous finding (Jin et al., 2022) that MDD patients display an attenuated association between fairness perception and acceptance behavior in the Ultimatum Game.
External validity analyzesThe learning rate for losses in the reputation non-disclosure condition was correlated with depressive symptoms measured by PHQ-9, harm avoidance, and anhedonia indicated by temporal experience of pleasure. This implied that the hypersensitivity to losses might be associated with depressive symptoms, harm avoidance, and anhedonia.
Our findings also suggest that only in the reputation non-disclosure condition where situational unpredictability was high, the learning rate for losses was positively related to depression-related symptoms or personality traits. This implies that these depressive symptoms or personality traits are more pronounced risk factors for mal-adaptive social learning in environments with high situational unpredictability. Future studies can further investigate the causal link between changes in learning rates for losses and various depressive symptoms or personality traits among MDD patients especially in highly unpredictable environments.
Situational unpredictabilityMultiple findings in our study convergently show that the MDD patients had more serious impairments in reinforcement learning and more mal-adaptive trust behaviors when the level of situational unpredictability was high versus low. These findings support hypothesis H4. High situational ambiguity is characterized by (1) not knowing reputation information of partners, and (2) partners’ chance of reciprocity approximates chance level. Our supportive findings thus include (1) there was a smaller difference between patients and controls in the learning rate for losses and the average rate of investment in the reputation disclosure condition than the reputation non-disclosure condition; (2) patients showed a lower rate of investment when they interacted with trustees with 50% and 70% chance of reciprocity in the reputation disclosure condition. Our findings are consistent with past studies which found a larger negative perceptual bias among MDD patients towards ambiguous stimuli as compared to non-ambiguous (i.e. either positive or negative) stimuli (Beevers et al., 2009; Münkler et al., 2015). Our findings may highlight that decreasing situational unpredictability may be beneficial for enhancing social adaptability in MDD patients.
LimitationsOur study has several limitations. First, parameter recovery tests suggested moderate level of correlation between original and recovered parameters. This could be attributed to the limited number of valid trials that involve learning from feedback. As feedback was delivered only after an investment was made, non-investment trials did not involve learning since no feedback was delivered. The average valid trials was 68 (65 for MDD; 73 for HC) in the reputation non-disclosure condition, and 49 (47 for MDD; 52 for HC) in the reputation disclosure condition. Second, the limited number of valid trials (See Supplementary Material Table S7–1) also prevents us from performing reliable parameter estimation for candidate models which specify different learning rates for partners with different levels of repay. Future studies could enlarge the number of valid trials to model the potential difference of learning rate by partner types. Third, partners in the rTG are not real persons. However, we did not collect information about the extent to which participants believe that they were playing with real persons in real time. Future studies should include a manipulation check about whether participants believed they played with real persons in real time.
Clinical implicationsOur findings highlight that the abnormal learning for losses underlies the social learning process among MDD patients and thus provide novel insights into learning process in the social interactional context in people with MDD. Our findings also open avenues for a new treatment target for social rehabilitation of MDD patients. Therapists could focus on ways to mitigate patients’ excessive learning for losses via altering patients’ cognitive processing about social losses. In addition, our findings suggest that reducing situational unpredictability might be a critical aspect underlying promoting a socially supportive environment for MDD patients.
ConclusionMDD patients exhibited lower levels of trust behavior towards trustees with low and moderate level of trustworthiness when they were naïve to the reputation of their partners, and exhibited lower levels of trust behavior towards trustees with moderate level of trustworthiness when the reputation of their partners was known. Parameter estimation further implies that the above lower level of trust behaviors was associated with increased learning rate for losses, while we did not find associations with learning rate for gains. MDD patients exhibited a higher discrepancy in trust behaviors and learning rate for losses compared to controls when the trustworthiness of their partners was not pre-disclosed.
Data availability statementData for this research project will be available upon reasonable request to the corresponding author.
Funding statementThis work was supported by the Natural Science Foundation of China (Grant Nos. 81771473, 82171535 and 72033006), and the Scientific Foundation of Institute of Psychology, Chinese Academy of Sciences, No. E2CX3815CX.
Ethics approval statementThe study was approved by the Ethics Committee of Beijing Anding Hospital and the Institutional Review Board of the Institute of Psychology, Chinese Academy of Sciences.
Patient consent statementAll participants viewed and signed the informed consent before the experiment.
We would like to thank all the participants who participated in this study. We are also grateful towards the supports from Qun Chen, Guofu Zhang and other staff in the Beijing Anding Hospital. We appreciate the suggestions from Junyi Dai in Zhejiang University to the early version of this study.
