




Aeromedical evacuation missions to transport highly infectious critical COVID-19 patients involve multiple factors, therefore planning is essential in their preparation. The management of specialist nurses is cross-cutting, as they participate in the planning, organisation and implementation of aero-evacuation protocols, delivery of care and operational safety procedures throughout the operation, with an integrated aeromedical crew working as a team alongside the air crew.
ObjectiveTo study the management of nurses specialised in the aero-evacuation of highly infectious critical patients during the COVID-19 pandemic.
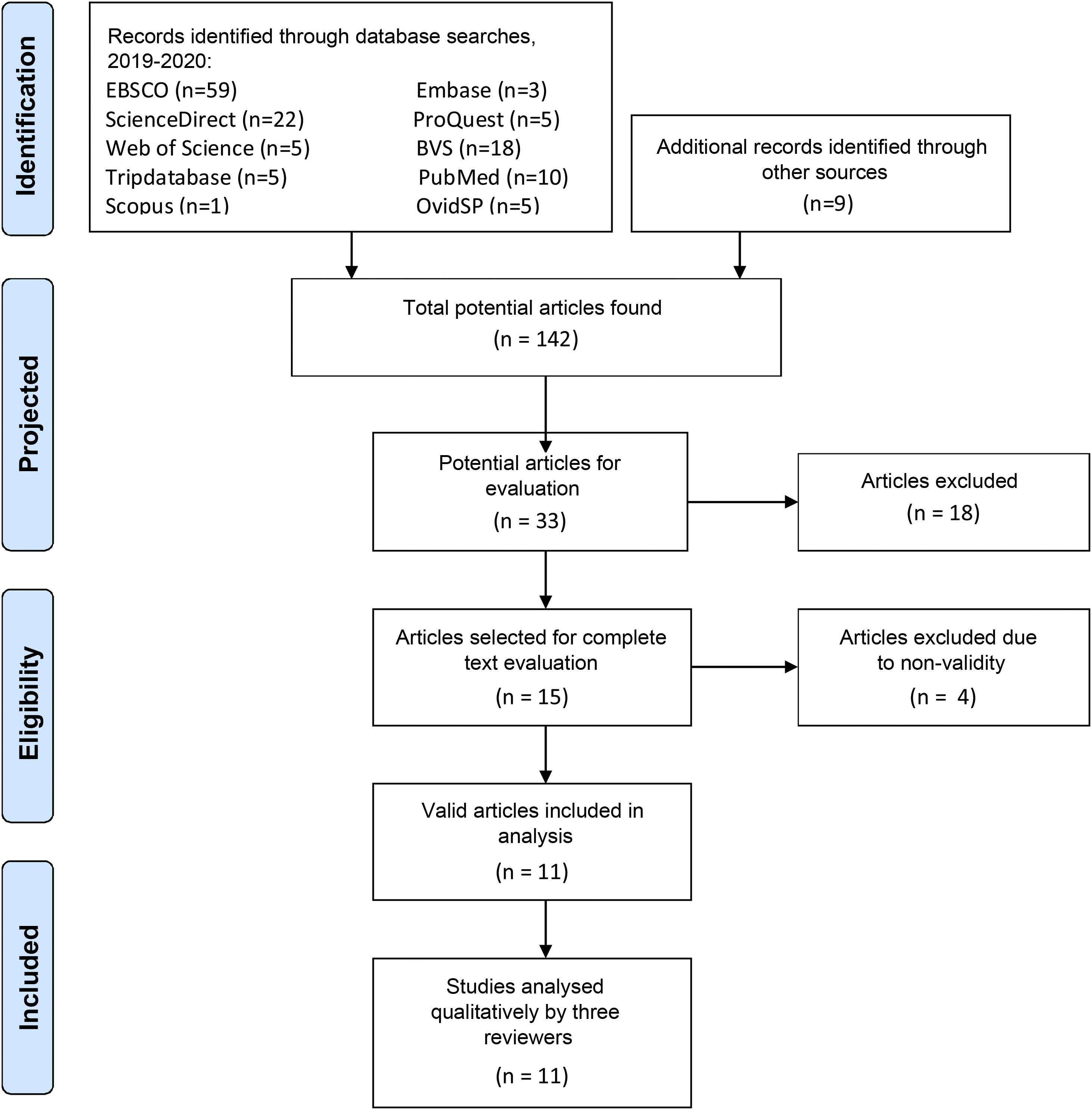
DesignThrough a systematic search of the biomedical literature, this study was conducted according to the standards of the Cochrane Handbook for Systematic Reviews of Interventions and PRISMA. The literature search included articles published from 2019 to August 2020 and meta-search engines, yielding a total of 142 articles, and a triangulation of information was performed. A total of 11 articles were eventually included in the review, and the validity of each article was determined according to the guidelines of the Joanna Briggs Institute level of evidence.
Results and discussionThe systematic review identified 11 studies that use different methodological considerations for conducting an aeromedical evacuation and covering key aspects for a successful operation.
ConclusionThe management of specialist nurses has a direct impact on the aeromedical evacuation of the critical patient. It covers planning, organisation, and operational safety, applied in the instruction, training, execution and strict monitoring of the work of the aeromedical crew as a solid team. This contributes to the success of the aero-evacuation mission and the infectious patient’s high likelihood of survival during the COVID-19 pandemic.
Las misiones de Evacuación Aeromédica de Paciente Crítico Altamente Infeccioso de paciente COVID-19, consideran múltiples factores, es por eso que la planificación, es la estructura fundamental de la preparación de la misión. La gestión de enfermeras/os especializados es transversal, ya que participa en gran parte en la planificación, organización y la aplicación de protocolos de aeroevacuación, ejecución de procedimientos asistenciales y de seguridad operacional durante toda la operación, con una Tripulación Aerosanitaria integrada trabajando en equipo junto a la tripulación aérea.
ObjetivoAnalizar la gestión de enfermeras/os especializados en la aeroevacuación de pacientes críticos altamente infecciosos, durante la pandemia por COVID-19.
DiseñoMediante una búsqueda sistemática de la literatura biomédica, este estudio se realiza según normas del manual Cochrane para las revisiones sistemáticas de las intervenciones y PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses). La búsqueda bibliográfica incluye artículos publicados desde el 2019 hasta agosto del 2020 y se utiliza metabuscadores, de lo cual se obtiene un total de 142 artículos, se realiza una triangulación de la información. Finalmente 11 artículos se incluyen en la revisión, y la validez de cada uno de ellos fue determinada de acuerdo con las directrices publicadas por el nivel de evidencia de Joanna Briggs.
Resultados y discusiónLa revisión sistemática evidencia 11 estudios que utilizan diferentes consideraciones metodológicas para la realización de una evacuación aeromédica considerando aspectos claves para una operación exitosa.
ConclusiónLa gestión de enfermeras/os especializados tiene un impacto directo en el proceso de Evacuación Aeromédica de Paciente Crítico Altamente Infeccioso, en diversos aspectos, como lo es la planificación, organización y seguridad operacional, aplicada en la instrucción, entrenamiento, ejecución y control estricto del quehacer de la Tripulación Aerosanitaria como equipo consolidado, contribuyendo en el éxito de la misión de aeroevacuación y a una alta probabilidad de sobrevida del paciente infeccioso en la pandemia por COVID-19.
The management of specialised nurses in aeromedical transport is an important factor in achieving patient success and survival considering clinical, operational, administrative and flight safety aspects, especially in highly infectious patients with COVID-19.
What it contributesThe analysis conducted in this systematic review provides aspects that are relevant and necessary to support the development of efficient and effective nurse management during the aeromedical transfer of highly infectious patients with COVID-19.
Study implicationsKnowledge of the key aspects of conducting an aeromedical evacuation enables the nurse practitioner to manage their care, ensuring quality and safety in the care of the highly infectious airborne COVID-19 patient.
In 1983, the Chilean Air Force (FACH) carried out its first aeromedical evacuation from Santiago – Punta Arenas – Santiago in a fixed-wing aircraft and the aerosanitary crew (ASC) at that time consisted of a cardiovascular surgeon and a nurse from the intensive care unit, whose mission was to stabilise a patient and transfer him, as he required emergency surgery due to a serious traumatic injury. Since that time, aero-evacuations have been consolidated and evolved over time in a number of areas, such as ASC training, medical equipment and care protocols.
In 2014, following the outbreak of the Ebola virus in Africa and in view of the imminent risk of a pandemic, the institution acquired specific equipment for the transfer of patients, consisting of isolation capsules, personal protective equipment (PPE) and protocols were created to address this problem. Training of the ASCs for this type of Highly Infectious Critical Patient Aeromedical Evacuation (HICPAE) of high or low complexity begins.
Following the declaration by the World Health Organisation (WHO) of the SARS-CoV-2 pandemic as a Public Health Emergency of International Importance (PHEII)1 and subsequently, in response to ministerial requirements, the Air Force began planning the logistics from the health point of view to form the HICPAE unit, which is made up of highly trained and specialised personnel, trained in the use of PPE and special equipment, all based on the lessons learned from the great powers in aviation medicine and aero-evacuation, such as the United States Air Force, the Spanish Air Force, the Brazilian Air Force and Italy. The above, with the aim of forming the aforementioned aero-evacuation unit with high standards of safety and quality for the care of infectious patients, with the indispensable support of the air crew, forming a consolidated nucleus in the aircraft. At the start of this process, various needs are reported, such as the training of CSAs, in this case institutional and extra-institutional, considering various governmental organisations, thus training the health crews of the Navy, Carabineros and members of the Emergency Medical Care Service, who learn a doctrine of long-haul en route care, far from their standard of pre-hospital care and urban transfer context. In this way, the human resources are amplified, taking into account the possible contagions among health personnel in the context of the pandemic and the contagions associated with the aero-evacuation procedure. Aviation medicine, flight physiology, care of the critical infectious patient during the entire aero-evacuation process and handling of specialised equipment in fixed and rotary wing aircraft are considered distinctive competencies.
Against this backdrop, a scenario of high transfer requirements was planned, considering the mobility of highly infectious critical patients using air travel throughout the national territory, depending on the existence of the resource in a territory with a constant geographical challenge and extensive areas to be covered of more than 5000 km.
In order to successfully carry out this type of operation, the following components are also required: configured aircraft, specific equipment, air crews, standardisation of protocols that guarantee clinical care and the role of specialised nurses, in compliance with established operational safety standards.2
In the aforementioned components, the role of Nursing Care Management becomes a key and transversal aspect of the whole process involving HICPAE. According to the Chilean Standard N.19 of the Ministry of Health, Nursing Care Management is defined as the application of professional judgement in planning, organising, motivating and controlling the provision of timely, safe and comprehensive care that ensures continuity of care and is based on the policies and strategic guidelines of the institution.3 These functions are performed by nurses specialised in the air transport of infectious patients during the COVID-19 pandemic.
The aim of this study is to analyse the management of nurses specialised in the aero-evacuation of highly infectious critical patients during the COVID-19 pandemic.
MethodologyA systematic review of the biomedical literature was conducted, this study is based on the standards of the Cochrane handbook for systematic reviews of interventions and PRISMA.4,5 The literature search included articles published from 2019 to August 2020, using meta-search engines such as OvidSP, EBSCO, Embase and Tripdatabase, in addition to the databases PubMed, ScienceDirect, ProQuest, Web of Science, Scopus and the Virtual Health Library (VHL); to avoid loss of information, a manual search for articles that could be relevant was included (Fig. 1). No limits were set for the searches, both in terms of language and type of study, but the search was defined for adult patients. The search strategies used were as follows:
- •
aeromedical transport AND nurse OR nurses OR nursing AND critical care
- •
air transport AND nurse OR nurses OR nursing AND critical care
- •
aeromedical evacuation AND nurse OR nurses OR nursing
- •
air transport AND COVID-19 AND nursing
- •
aeromedical evacuation AND COVID-19 AND nursing
- •
aeromedical evacuation AND COVID-19 AND nursing AND critical care
- •
aeromedical evacuation AND COVID-19 AND military nursing

After obtaining the references and abstracts, the articles related to air transport of critical patients with confirmed or suspected cases of SARS-CoV-2 virus were selected, resulting in a total of 142 articles that could be evaluated (Fig. 1), of which 33 were chosen because they were specifically related to the topic, while 18 of them were discarded because they were not related to the COVID-19 pathology or because they did not correspond to research studies, for example, because they were replicas of letters to the editor, protocols, etc.
To avoid the omission of relevant articles, a triangulation of the information was carried out, reviewing the articles related to the selected articles, as well as the review of the bibliography of each of the selected articles.
Fifteen articles were selected to be evaluated in full text, two published in Spanish and 13 in English, the latter being translated from their original language into Spanish in order to be able to carry out the analysis correctly.
After the first analysis of the articles, four articles were excluded as they corresponded to publications related to the topic, but did not reach 50% compliance in the analysis of evidence, according to guidelines corresponding to the type of study (AGREE Reporting Checklist [Appraisal of Guidelines Research & Evaluation], CARE Checklist [Case Report Guidelines], SANRA [Scale for the Assessment of Narrative Review Articles]).
Finally, 11 articles are included in the review,6–16 and the validity of each article was determined according to the guidelines published by Joanna Briggs’ level of evidence (Table 1).
Analysis of the quality of evidence in each article.
| Number | Author | Country | Year | Design | Analysis of evidence | Percentage of evidence | Level of evidence JBI |
|---|---|---|---|---|---|---|---|
| 1 | Gardiner et al. | Australia | 2020 | Cohort study | STROBE | 81.80% | 3b |
| 2 | Sammito et al. | Alemania | 2020 | Retrospectivd | STROBE | 75% | 3e |
| 3 | Bredmose et al. | Australia | 2020 | Systematic review | PRISMA | 56.60% | 4a |
| 4 | Osborn et al. | United States | 2020 | Narrative review | SANRA | 83% | 3b |
| 5 | HIQA | United Kingdom | 2020 | Clinical guide | AGREE | 78% | 5b |
| 6 | Tien et al. | Canada | 2020 | Narrative review | SANRA | 76% | 3b |
| 7 | Olsen et al. | United States | 2020 | Narrative review | SANRA | 50% | 3b |
| 8 | Mohrsen et al. | United Kingdom | 2020 | Case study | CARE | 100% | 4d |
| 9 | Borges et al. | Brazil | 2020 | Case study | CARE | 90% | 4d |
| 10 | Wanner et al. | Chile | 2020 | Case study | CARE | 76.60% | 4d |
| 11 | Martin | United States | 2020 | Letter to the editor | – | – | – |
The evidence of each study is assessed by means of a percentage, considering those with ≥50%, to which Joanna Briggs’ level of evidence is then applied (JBI, http://joannabriggs.org/assets/docs/approach/JBI-Levels-of-evidence), where: Level 3.b: systematic review of comparable cohort and other inferior study designs, Level 3.e. Observational study without control group, Level 4.a: systematic review of descriptive studies, Level 4.d: case study, Level 5.b: expert consensus; Level 5.c expert consensus.
Each article was analysed independently by three of the authors, the assessments were then compared. This analysis was concordant, so it was not necessary to involve a fourth author to act as, a mediator, reach agreement between the assessments.
After each article was validated, these were incorporated into the analysis of the criteria included as actions to be taken in the HICPAE (Table 2).
Main aero-assessment criteria used in each article.
| Number | Criteria/items | Articles | % | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |||
| 1 | Aero-evacuation nurse management | S | S | S | N | N | S | N | N | S | S | N | 54.5 |
| 2 | Planning | S | S | S | S | S | S | S | S | S | S | S | 100 |
| 3 | Process | S | S | S | S | N | S | S | S | S | S | N | 81.8 |
| 4 | Type of aircraft | FW | FW | RW | FW–RW | N | FW–RW | FW–RW | RW | FW | FW | FW | 90.9 |
| 5 | Level of patient severity | LMH | LMH | LMH | LMH | N | LMH | N | N | B | LMH | N | 63.6 |
| 6 | ASC condition | C | MX | C | M | N | C | C | C | M | M | N | 81.8 |
| 7 | ASC members | ME | MET | MT | ET | N | T | T | T | MET | MET | N | 81.8 |
| 8 | Transfer time (in hours) | 6 | N | N | N | N | 2 | N | N | 37 | 8 | N | 36.3 |
| 9 | National/international | NAT/INT | NAT/INT | N | NAC | N | NAC | NAC | NAC | INT | NAC | N | 72.7 |
| 10 | PPE use | N | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | 81.8 |
| 11 | Use of HCWM | N | N | Y | N | Y | N | N | Y | Y | N | N | 36.3 |
| 12 | Distribution of aircraft by areas | N | N | Y | N | N | Y | N | N | Y | Y | Y | 45.4 |
| 13 | Decontamination protocols | N | N | N | Y | Y | Y | Y | N | Y | Y | N | 54.5 |
| 14 | Administrative and care procedures | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100 |
| 15 | Preventative procedures | Y | N | Y | Y | N | Y | N | Y | Y | Y | Y | 72.7 |
| 16 | Restricted procedures | N | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | 81.8 |
| 17 | Use of capsules | N | N | Y | N | N | N | N | N | Y | Y | Y | 36.3 |
| 18 | Patient selection prior to embarkation | Y | Y | Y | Y | N | N | N | Y | N | Y | Y | 63.6 |
| 19 | Operational safety | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100 |
| Number | Criteria | Definition | Initial |
|---|---|---|---|
| 1 | Type of aircraft | Fixed wing/rotary wing | FW/RW |
| 2 | Patient severity | Low/medium/high | L/M/H |
| Low: ambulatory, non-life-threatening patient. | |||
| Medium: non-life-threatening patient, requires intermediate level of care. | |||
| High: life-threatening patient, intubated and VCDa | |||
| 3 | ASC condition | Military/civil/mixed | M/C/Mx |
| 4 | ASC members | Doctor/nurse/nursing assistant | D/N/A |
| 5 | Transfer time | In hours | In hours |
| 6 | National/international | Refers to aero-evacuations made inside and outside the country | NAT/INT |
| 7 | YES/NO | YES: criteria compliance. | Y/N |
| NO: criteria non-compliance |
Numbers 1–11 correspond to each selected article, if the criterion is present in the article it is symbolised with an “S”, if it is not present it is symbolised with an “N”, which finally gives a % of the total of each of the criteria present.
The results found for each criterion, included in the management of nurses specialised in aero-evacuation, in the actions to be carried out in the HICPAE, are presented below.
- 1.
Management of nurses specialised in aero-evacuation
The description of the management of nurses specialised in aero-evacuation is included in 54.5% of the studies.6–8,11,14,15 Among the elements of care, 18.1% point out the importance of protocolising the transfer of critical patients7,15 and 18.1% point out the importance of carrying out clinical checks on take-off and landing.7,14 Of the articles, 63.6% describe the planning and organisation of human and physical resources for the successful execution of missions, guaranteeing operational safety aspects for the patient and the ASC.7–9,11,12,15,16 Contingency control in the event of an increase in demand for air transfers is set at 9%.6 Bredmose et al. and Borges et al. establish care management guidelines for pre-flight, in-flight and post-flight resource and action planning.8,14 Tien et al. and Wanner et al. highlight that the competencies of CSAs are of varying levels of criticality, which establishes motivation in them in the pre-pandemic period and during the pandemic.11,15 Wanner et al. in their institutional experience report the relevance of media planning prior to each mission and monitoring during patient preparation for transport with 9%.15 Infection control strategies are included as a care indicator.8
- 2.
Planning
Planning is one of the axes in the management of nursing care in aero-evacuation, this element is identified in 100% of the studies reviewed and its considerations are set out as follows: human resources (ASC and logistic personnel), was described in 90.9% of the articles,7–16 logistics referring to supplies and PPE, was described in 81.8% of the studies,7–15 development of technical guidelines and protocols for the care of infectious patients,7–14,16 was described in 81.8% of the publications.
Protocols for the transfer of infectious patients are specifically detailed: aircraft selection was described in 45.4% of the articles7,11,12,15,16; aircraft disinfection in 54.5%8,9,11,12,14,15 and coordination with secondary ground transport in 18.1%.10,16
Another element analysed is network planning,12 which includes: team meetings,13 team communication,16 mental health considerations and verification of general ASC conditions.16
Finally, planning considers the type of operation, levels of risk and safety, and this was identified in 54.5% of the studies analysed.9,11–13,15,16
- 3.
Processes
The processes established in aero-evacuation are detailed in 81.8% of the studies analysed. Gardiner et al. propose a model of care for patients with COVID-19 based on its responsiveness, preventive actions, patient classification and description of outcomes.6 Sammito et al. point out that the main components in the process are ASC conformation, aircraft type, patient selection, use of intensive care unit (ICU) protocols, use of PPE and patient evolution.7 Bredmose et al. describe their process from the development of clinical guidelines, mitigation strategies, and general procedures to mission completion.8 Several authors describe clinical and operational guidelines in the process.7,9,11 Tien et al. consider within the process the physical and mental preparation and protection of staff, the strategy of which is to maintain constant communication.11 Olsen et al. describe six strategic objectives to be developed during the aero-evacuation, based on the experience of other countries, by working online and sharing health intelligence information.12 Mohrsen et al. consolidate the processes by simulation modelling of general procedures to be performed.13
- 4.
Types of aircraft
The description of the type of aircraft used for evacuation of infectious patients is indicated in 90.9% of the studies.6–9,11–16 A total of 45.4% of aeromedical evacuations are performed in fixed-wing aircraft,6,7,14–16 18.1% in rotary-wing aircraft8,13 and 27.2% of articles report using both types of aircraft.9,11,12
- 5.
Assessment of patient severity
The evaluation of patients who are candidates for aero-evacuation includes their prioritisation and risk assessment, for which the measurement of physiological variables is considered. These parameters must indicate that the transfer does not increase the patient’s risk of mortality, for which scoring systems similar to those used in intensive care units are used, such as the Acute Physiology and Chronic Health Evaluation II (APACHE II).17,18
In the analysis of these articles, 9% describe the criteria for selecting patients for transfer,6 prioritising patients who require invasive ventilatory support, assistance from a specialised multidisciplinary team, and who are guaranteed safe care during the flight.
One of the methods used to assess the severity of the patients mentioned is the discrete event simulation (DES) classification,6 which allows the appropriate prioritisation and organisation of the transfer.
- 6.
Description and characteristics of the ASC
The status of the ASC is described in 81.8% of studies,6–9,11–15 which may be made up of health professionals, civilians or military. In this review, 45.4% are civilians,6,8,11–13 27.2% are military9,14,15 and 9% are mixed ASC made up of civilians and military.7 No advantages or disadvantages are indicated in relation to the composition of the CSA in the transfer of critical patients.
- 7.
ASC members
The CSA is usually made up of doctors, nurses and paramedics, and the participation of these professionals is described in 81.8% of the studies analysed.6–9,11–15 In 27.2% of the studies estudios7,14,15 the CSA is made up of a doctor, nurse and paramedic, in 9% it is made up of a doctor and nurse,6 in 9% it is made up of a doctor and paramedic,8 in 9% it is made up of nurses and technicians9 and in 27.2% it is only made up of paramedics.11–13
- 8.
Transfer time
This variable is described in 36.3% of the studies and forms part of the operational process in the planning of a transfer. It considers the assessment of risks, patient needs, crew safety and not exposing people unnecessarily. In studies describing transfer time, the variability ranged from two hours to 37 h.6,11,14,15
- 9.
National/international
The destination of the missions is described in 72.7% of the studies, and corresponds to the request, need for transfer or repatriation of patients.6,7,9,11–15 In 45.4% of the studies, transfers carried out at national level were described,9,11–13,15 9% of international missions14 and 18.1% of the studies refer to missions at national and international level.6,7
- 10.
PPE usage
Given that the SARS-CoV-2 virus disease is highly contagious and still unknown in some respects, there is a need to use PPE as a protective measure to prevent contagion in health professionals or ASCs caring for patients with respiratory symptoms. Such PPE, as recommended by the WHO, is contact and droplet protection on a routine basis, and airborne precautions for procedures that generate aerosols. This has been stipulated in most countries’ guidelines or consensus, although the US Center for Disease Control and Prevention (CDC) and Europe tend to take precautions against airborne transmission directly.19
Within the studies analysed, 81.8% specify each of the PPE used by the ASC in their transfers, these include: procedure gloves in 81.8%,7–9,11–16 eye protection with goggles or face shields in 81.8%,7–9,11–16 N95 respirator in 72.7%,7–9,11,12,14–16 N99 respirator in 27. 2%,8,13,16 coveralls or overalls in 45.4%,7,8,13–15 associated or not with the use of aprons or gowns in 63.6%.8,9,11–13,15,16 27.2% wore caps or helmets,8,11,13 36.3% wore surgical masks.8,12,13,16 In other words, the preventive measures used are related to protection by contact and airborne transmission.
Regarding the use of surgical masks in spontaneous breathing patients, 27.2% of studies use this measure8,9,14 Cook et al. report an estimated risk reduction of at least 80%, which provides a form of prevention and protection for the crew or healthcare personnel.19
Kang et al. report that increased training in the use of PPE certainly improves its use.20 In the analysis, it is observed that 54.5% of the articles studied refer to training in the use of PPE8,11,12,14–16 and only 36.3% consider the application of supervision guidelines.8,9,14,15
- 11.
Health care waste management (HCWM)
Each aeroevacuation generates waste or residues that represent a risk to health. Eighty per cent is solid waste assimilable to household waste and the remaining 20% is waste that poses a risk to public health and/or the environment.21 The analysis of this review shows that only three of the selected studies, 36.3%, describe healthcare waste management.8,10,13,14 However, they do not report on post-flight handling measures after the end of the flight with these wastes.
- 12.
Aircraft configuration
The configuration of the aircraft is described in 45.4% of the studies analysed8,11,14–16 and is distributed as follows: contaminated area; patient location; intermediate area; disinfection procedures and PPE change and decontaminated or clean area. Some studies describe the same areas as: hot (patient location), warm (intermediate area for PPE change) and cold (safety area).14,15 According to Bredmose et al. the use of a physical divider between cabins is implemented according to aircraft configuration.8
- 13.
Decontamination protocols
The decontamination protocols are included in 54.5%8,9,11,12,14,15 with 45.4% specifying that cleaning or decontamination should be carried out with PPE and by the ASC.8,9,11,12,14 27.2% agree that cleaning or decontamination of the aircraft should be carried out after the aero-evacuation has been completed.8,12,14 Once decontamination has been completed, 18.1% stated that the aircraft should be ventilated for 1 h8,9 and 36.3% stated that the ambulance transporting the patient to or from the hospital should be decontaminated.9,11,12,14 Regarding the agent to be used, it is mentioned that disinfection should be carried out in accordance with the manufacturer’s instructions,8,9 hydrogen peroxide,11,12 quaternary ammonium,15 sodium hypochlorite9 or the use of ultraviolet light.9 Regarding the disinfection of equipment and isolation capsule, only 9% of the studies mention the procedure.15.
- 14.
Administrative and care procedures
Administrative and care procedures made in the HICPAE are present in 100% of the analysed studies (Table 3).
- 15.
Preventative procedures
Administrative and care procedures for each item, performed during the preparation and flight stages in the aero-evacuation of a highly infectious patient.
| Procedures | Articles | % | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | ||
| Access to the clinical file to obtain patient data | S | S | S | S | 36.3 | |||||||
| Early intubation. | S | S | S | S | S | S | S | S | 72.7 | |||
| Sedation and deep relaxation prior to the flight. | S | S | S | S | S | S | S | 63.6 | ||||
| Necessary personnel and use of medical equipment. | S | S | S | S | S | S | S | 63.6 | ||||
| Medical care, assessment of parameters before, during and after the flight. | S | S | S | S | S | 45.4 | ||||||
| Use of orotracheal tube (OTT), central venous catheter (CVC), arterial line, urinary catheter, nasogastric tube (NGT), peripheral venous line (PVL). | S | S | S | S | S | S | S | S | S | 81.8 | ||
| Use of viral filters in transferred patients. | S | S | S | S | S | 45.5 | ||||||
| Closed circuit aspiration of secretions. | S | S | S | S | 36.3 | |||||||
| Use of portable isolation units with negative pressure environment. | S | S | S | S | S | 45.4 | ||||||
This table presents the most important Administrative and Care Procedures to be included in the whole aero-evacuation process. The numbers 1–11 correspond to each selected item, if the procedure is present in the item it is symbolised with an “S”, which finally gives a % of the total number of procedures present.
Preventive procedures are present in 72.7% of the studies analysed (Table 4).
- 16.
Restricted procedures
Preventative procedures made during preparation stages and flight in the aero-evacuation of the highly infectious patient found in each article.
| Preventative procedures | Articles | %a | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 1 | 3 | 4 | 6 | 8 | 9 | 10 | 11 | ||
| Border closure | S | S | 18.1 | ||||||
| Non-essential service closure | S | 9.0 | |||||||
| Difference between patients with respiratory diseases and patients with other pathologies | S | S | S | S | 36.3 | ||||
| Health survey, respiratory symptoms, fever or contact with cases of COVID-19 (+) | S | S | S | S | 36.3 | ||||
| Quarantine for 14 days of persons in contact with confirmed case or travelling to areas with COVID-19. | S | S | S | 27.2 | |||||
| COVID-19 testing in the presence of respiratory symptoms or fever | S | S | S | 27.2 | |||||
| Traceability of COVID-19 confirmed cases and their contacts. | S | S | S | S | 36.3 | ||||
| During aeromedical transport, change masks every four hours | S | 9.0 | |||||||
| Crew should practice hand hygiene and social isolation outside working hours | S | S | 18.1 | ||||||
| Pre-selection of route to referral hospital, minimising risk of cross-contamination | S | 9.0 | |||||||
| Segregation of areas | S | S | S | 27.2 | |||||
| Limit access to work, meal and rest areas for health teams. | S | 9.0 | |||||||
| Cleaning of surfaces and equipment before and after aero-evacuation. | S | 9.0 | |||||||
This table presents the recommended Preventive Procedures to be carried out throughout the aero-evacuation process. Numbers 1–11 correspond to each selected item, if the procedure is present in the item it is symbolised with an “S”, which finally provides a % of the total procedures present. Articles 2, 5, 7 are not considered as they do not present preventive procedures.
Restricted procedures are described in 81.8% of the studies analysed (Table 5).
- 17.
Use of individual isolation capsules
Restricted procedures for each item, used during the preparation and flight stages of the aero-evacuation process of a highly infectious patient.
| Restricted procedures | Articles | %a | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 2 | 3 | 4 | 5 | 6 | 7 | 8 | 10 | 11 | ||
| Physical contact | S | 9.09 | ||||||||
| Aerosol generating procedures: Non-Invasive Mechanical Ventilation (NIV), High Flow Nasal Cannula (HFNC), nebulisations, bag-ambu ventilation. | S | S | S | S | S | S | S | 63.6 | ||
| Suctioning of secretions with open system | S | S | S | S | 36.3 | |||||
| Disconnection of invasive mechanic ventilator | S | S | S | S | S | 45.4 | ||||
| Aero-evacuation with fuel limit, power consumption greater than aircraft support, night flight with use of night visors or day flight only, complex landing zone, cabin height limit. | S | S | S | S | 36.3 | |||||
| Use of gaseous oxygen balloons without hydrostatic certification. | S | 9.09 | ||||||||
This table presents the Restricted Procedures to be considered during the aero-evacuation process. The numbers 2–11 correspond to each selected article, if the procedure is present in the article it is symbolised with an “S”, which finally contributes a % of the total procedures present, Articles 1 and 9 are not considered because they do not present restricted procedures.
The use of individual patient isolation capsules is described in 36.3% of the analysed studies. The authors include the use of negative pressure capsules, among their models are the IsoArk, IsoPod and Epishuttle.8,14–16
- 18.
Patient selection prior to embarkation
Patient selection was included in 63.6% of the studies reviewed.6–9,13,15,16 Some authors establish guidelines for selecting patients for aero-evacuation as a mitigation measure to promote stable aero-evacuation.7,8,15 Martin establishes the selection of patients according to risk type, in this case using variable risk and high-risk algorithms.16 Mohrsen et al., for their part, establish as a requirement a negative polymerase chain reaction (PCR) test prior to transfer13 and finally Osborn et al. describe that patients should be selected by prioritising severity.9
- 19.
Operational safety
Operational safety in aero-evacuation is established in 100% of the selected studies. Gardiner et al. report that, as the number of requests for airlifts increases, the exposure of specialist healthcare personnel increases, leading to a massive drop in the number of such personnel, and therefore propose to increase the ASC to include medical students, nurses and Australian defence forces.6 Sammito et al. mention that due to the operational limitation of aircraft, the German Air Force performed five airlifts at a flight altitude between 6000 and 20,000 feet, thereby increasing the safety of patients and crew.7 Bredmose et al. reinforce safety in the operation and selection of PPE according to the aircraft to be used, recommending apron over full coverall.8 Osborn et al. report that there is greater operational safety in fixed-wing aircraft,9 as the compartment allows the pilot to be isolated from the patient, a risk that is reduced by using portable isolation units with the respective training in their use for healthcare personnel. Tien et al. note that cabin separation reduces operational risk.11 In the Health Information and Quality Authority (HIQA) review, it is mentioned that the most important thing is PPE.10 Olsen et al. emphasise a safety approach before, during and after the air mission, considering the patient in an uncontrolled situational state scenario.12 Mohrsen et al. state that patients suspected of COVID-19 are airlifted only if they have a negative PCR test.13 Borges et al. established circulation areas to increase operational safety.14 Wanner et al. mention the importance of using gaseous oxygen balloons with flight certification.15 Martin points out that certain safety-related questions need to be answered operacional16: is the aircraft suitable for transporting infectious patients, is there comprehensive communication, and is the centre of gravity of the aircraft affected by the location or weight of the equipment?
DiscussionIn the FACH experience, these four axes (planning, organisation, motivation and control) are included, with emphasis on planning and organisation, due to the fact that the arrival of the pandemic required the preparation of equipment and personnel, with emphasis on the training of the ASCs, in the execution of the different procedures and the use of specialised equipment.
Of the aspects included in the aero-evacuation process, the planning of a HICPAE considers various elements, which are mentioned in most of the articles analysed, such as: assessment of human resources, verification of the general and mental health conditions of the ASCs, which is fundamental for the execution of these missions as it is essential for the safety of the personnel and their performance during the aero-evacuations. Logistics, selection of the type of aircraft, provision of supplies and PPE must be considered on the basis of a projection according to the number of patients and number of flights to be carried out. In terms of operations and care, the information analysed includes and develops the review of pre-flight procedures, operational safety aspects, network planning, work meetings, development of technical guidelines, protocols for infectious patient care, disinfection and management of HCWM. The aim is to have strategies to mitigate risks associated with the aviation environment and possible complications that may arise for the patient or crew. In FACH’s institutional experience, planning becomes the fundamental axis for initiating the aerovacuation process, which must be carried out in a methodical and structured manner in order to achieve the proposed objectives.
The types of aircraft used for aeromedical evacuations can be fixed-wing or rotary-wing, but there is a greater use of fixed-wing aircraft in aero-evacuations, due to the flight time, the space that allows separation of areas and autonomy, the pressurisation that reduces physiological effects on patients and the air crew. In rotary wing, there is no energy supply for the equipment and the reduced space of the aircraft limits its movements when carrying out procedures, but it can land and take off on any runway. The FACH institutional experience for HICPAE was in both types of aircraft, with a higher percentage of fixed-wing aircraft, as the dimensions of these allow a greater number of patients to be transported.
There are different methods of severity classification that allow for the selection, prioritisation or organisation of transfers, an example of which, according to the study, is: classification by discreet event simulation (DES). Regardless of the type of criteria or scale used to measure severity, this should be protocolised in order to minimise risks.
The condition of the ASC refers to the composition of the crews, be they military, civilian or mixed, and it is vital that it is made up of a trained team with competencies in critical medicine, emergency medicine and aviation medicine, who are familiar with the processes and act with defined standards. The members of the ASC are doctors, nurses and paramedics, and depending on the complexity of the patient being transferred, a complete team is optimal, given that the functions or roles in the task are different, however, they complement each other in their execution.
The transfer time, an important link when planning the mission, must guarantee the safety of the patient and the crew. The longest institutional experience in national territory was eight hours.
The use of PPE is considered a vitally important measure for prevention, reducing the spread of the disease, which has a high mortality rate for those who contract it, without excluding the ASC and air crew. The application of guidelines for the supervision of the correct use of PPE during installation and removal favours the prevention of contagion during the aerosanitary transfer.
With regard to the institutional experience of aeromedical transfers during the SARS-CoV-2 pandemic, the ASC protects itself from airborne and contact transmission, as do the studies indicated in this review using: clinical clothing, hooded coveralls, long and short nitrile gloves, full-face mask and boot covers. In the case of rotary wing aero-evacuation, only a one-piece biosafety coverall should be considered to reduce the risk of accidents due to the detachment of individual PPE. Training is carried out prior to transfers and guidelines are applied to supervise the correct use of PPE.
Both in the review of the articles and in the institutional experience, there is no record of contagion of ASC, which could be considered as an indicator of compliance with preventive measures.
The handling of HCWM is a critical point during flight planning and must be carried out under strict safety rules and with adequate protection for their handling, in order to avoid exposing the crew to unnecessary risks during aero-evacuation. From the selected studies, there is a low percentage of background information related to this measure.
During the aero-evacuations carried out by the institution, an intermediate area is identified in the aircraft where a HCWM container is located, the disposal of which is carried out at the hospital of destination. There is also an agreement with a company accredited by the local health authority for the removal of HCWM, in the case of remnants collected on the aircraft.
The aircraft is made up of areas: contaminated zone where patients go; intermediate zone where disinfection and PPE replacement procedures are carried out; and decontaminated zone. In the different studies, these three areas are defined for fixed-wing aircraft; in the case of rotary-wing aircraft, these three areas cannot be differentiated; only the crew area is kept isolated from the aircraft, with a physical divider. This configuration is in line with the operational experience of the Chilean Air Force.
Decontamination, a critical procedure associated with preventive and strategic infection control measures, should be carried out with PPE by the ASC at the end of the aero-evacuation, considering the aircraft, equipment, capsule and ambulance transporting the patient.
In relation to the agent used, there are several alternatives: hydrogen peroxide, quaternary ammonium, sodium hypochlorite and the use of UV light; however, no study specifies the scientific evidence for each agent. Only 16.6% of the studies mention these measures, which is a low percentage of description, considering the criticality of the procedure in this type of transfer. In the FACH experience, decontamination is a critical procedure and is carried out in accordance with protocols emphasising safety pauses in the decontamination of capsules and equipment, mainly on boarding the aircraft.
The administrative and assistance procedures in aero-evacuation of critical and highly infectious patients require a high level of specialisation of the personnel and adequate equipment, which are feasible to perform considering the efficiency and safety in their execution, such as early intubation, sedation and deep relaxation, medical care and control of vital signs pre-flight, during and post-flight, use of invasive monitoring, use of viral filter, closed circuit aspiration of secretions, correct use of PPE and isolation units, as well as prior access to all patient documentation.
Restricted procedures in the execution of a flight may be subject to different factors, such as cabin altitude, adverse weather conditions, fuel restriction, problems in the landing zone or only daytime flights. There are patient-specific factors to consider in patient care protocols that restrict flight, such as PAFI less than 150, FiO2 greater than 90%, patient pronated or weight greater than 120 kg. At the care level, avoid aerosol-generating procedures and/or unnecessary disconnections of the mechanical ventilator.
Preventive procedures are essential to reduce operational risks that may affect the aero-evacuation mission, protect the patient, air crews and the ASCs, and are divided into pre-flight, establishing the difference between respiratory and non-respiratory patients, execution of the health survey, traceability actions for confirmed patients and their contacts, screening for COVID-19 with symptomatology, quarantine if close contact or travel to areas of high transmissibility, promotion of self-care measures for aircrews and HCWs, route selection from the referral hospital to reduce the risk of cross-contamination.
The use of negative pressure capsules can be IsoArk, IsoPod and Epishuttle. Only a few of the studies reviewed include the use of individual isolation capsules, and there is no evidence that refers to the operational safety of using or not using this type of device.
The selection of patients is established as a mitigation measure and favours stable aero-evacuation. Its requirements are according to risk, by means of algorithms for risk definition, examination prior to transfer and prioritisation according to the severity of the patient. In relation to FACH’s institutional experience, patients are selected the day before, with evaluation of haemodynamic parameters, examinations and control of these on the day of the aero-evacuation.
Operational safety in aero-evacuations involves a series of components from the operational side of the aircraft, considering a flight altitude between 6000 and 20,000 feet, choice of the aircraft according to the type of patient, taking into account that it does not affect the aircraft’s centre of gravity, which is directly related to the defined safety and circulation areas, establishing greater safety in fixed-wing flight equipment, as the isolation of the air crew from the patients is achieved. In addition, the preparation of a controlled scenario, with adequate PPE according to the aircraft and sufficient equipment to ensure that care during the flight is smooth. In addition to the above, the level of safety is increased by the use of individual isolation units, the oxygen cylinders have aeronautical certification and communication is integral to the ASC, which is critical if in-flight procedures are to be carried out.
Scientific limitations of the studySeveral structured methods are used for triangulation of the information obtained, and no restrictions are used in the search for information to ensure that the results are robust. However, it is likely that despite this the results have a publication bias, as given the severity of the pandemic many critical patient transfer teams in this period have not published their transfer methods in sources that are accessible worldwide, this information may not be published, and if published in the future should be contrasted with the findings of this study to assess whether or not they reinforce these conclusions.
RecommendationsBased on the items addressed in the various articles included in this systematic review, a checklist has been drawn up for the flight nurse to apply each time a HICPAE is performed, including all the dimensions to be considered when performing this type of aero-evacuation (Table 6).
Highly infectious critical patient aeromedical evacuation checklist.
| Criteria/items | Check | Definition | Observation | |
|---|---|---|---|---|
| Planning | a. ASC role | ○ | ||
| b. Logistics | ○ | |||
| c. Care protocols | ○ | |||
| d. Aircraft selection | ○ | |||
| e. Type of aircraft | ○ | AF–AR | ||
| f. Patient severity | ○ | B – M – A | ||
| g. ASC condition | ○ | M – C – MX | ||
| h. ASC members | ○ | M – E – T | ||
| i. National/international | ○ | N – I | ||
| j. Transfer time | ○ | ____ Hrs | ||
| Management of nurses specialised in aero-evacuation | a. Patient control register. | ○ | ||
| b. Organisation of care pre-flight, during flight and post-flight. | ○ | |||
| c. Checklist control of equipment and supplies for the mission. | ○ | |||
| d. Recording of incidents during the mission. | ○ | |||
| e. HCWM protocols | ○ | |||
| f. Decontamination protocol of equipment and isolation capsules | ○ | |||
| g. Supervision of aircraft decontamination | ○ | |||
| h. Use of PPE according to type of isolation | ○ | A – G – C | ||
| Distribution of aircraft into areas. | a. Clean area | ○ | ||
| b. Intermediate area | ○ | |||
| c. Contaminated area | ○ | |||
| Procedures to be taken | a. Access the pre-hospital record. | ○ | ||
| b. Deep sedation and relaxation prior to the flight. | ○ | |||
| c. Early intubation. | ○ | |||
| d. Use of minimum necessary medical equipment and personnel. | ○ | |||
| e. Take medical equipment and back-up batteries in case of failure | ○ | |||
| f. Medical care and vital sign monitoring before, during and after the flight. | ○ | |||
| g. Use of TOT, CVC, arterial line, permanent urinary catheter (PUC) or SNG. | ○ | |||
| h. Fixation and management of TOT, CVC, arterial line, PUC, SNG and/or drains. | ○ | |||
| i. Aspiration of secretions with closed-circuit suction. | ○ | |||
| j. Emptying of drains and catheters. | ○ | |||
| Restricted procedures | a. Aerosol-generating procedures: VMNI, CNAF, NBZ, abu-bag ventilation. | ○ | ||
| b. Aspiration of secretions with open system. | ○ | |||
| c. Frequent disconnection of invasive mechanical ventilators. | ○ | |||
| d. Transfers of patient with PAFI under 150, FiO2 over 90%, prone position or heavier than 120 kg. | ○ | |||
| e. Aero-evacuation with fuel limit, power consumption greater than aircraft support, night flight using NVG or day flight only, complex landing area, cabin height limit. | ○ | |||
| Preventative procedures | a. Difference between patients with respiratory disease and other diagnoses. | ○ | ||
| b. Health survey on respiratory symptoms, fever or contact with COVID-19 (+) cases. | ○ | |||
| c. Quarantine for 14 days of persons in contact with confirmed case or travelling to areas with COVID-19. | ○ | |||
| d. COVID-19 testing in the presence of symptoms such as fever or respiratory failure. | ○ | |||
| e. Conduct traceability of confirmed cases with COVID-19 and their contacts. | ○ | |||
| f. During aeromedical transport, change masks every four hours. | ○ | |||
| g. Crew must practice hand hygiene and social isolation outside of working hours. | ○ | |||
| h. Segregation of areas. | ○ | |||
| i. Cleaning of medical surfaces and equipment. | ○ | |||
| j. At the referral hospital, pre-screening of the route. | ○ | |||
| k. Use of individual isolation capsules with negative pressure environment. | ○ | |||
| l. Pre-screening of patients prior to boarding. | ○ | |||
| Operational safety | a. Permissible flight altitude according to aircraft. | ○ | ||
| b. Selection of PPE according to type of aircraft. | ○ | |||
| c. Use of isolation chamber according to the anthropometric measurements of the patient. | ○ | |||
| d. Strict compliance with area configuration. | ○ | |||
| e. Location of patients in aircraft according to severity. | ○ | |||
| f. Use of flight-certified oxygen balloons or use of NPTLOX. | ○ | |||
| g. Use of power inverter ad hoc to the aircraft. | ○ | |||
| h. Supervise aircraft boarding and disembarking safety areas. | ○ | |||
| i. Supervise areas of crew’s internal circulation areas. | ○ | |||
| j. Control HCWM elimination process. | ○ | |||
| k. Know emergency procedures in the event of: ASC contamination, forced landing, imminent crash, splashdown, aircraft fire, aircraft depressurisation and emergency descent. | ○ | |||
| l. Disembarkation of patients according to severity and evolution during the flight. | ○ | |||
| m. Handling of protocols in case of with sharp item or contact with organic material | ○ | |||
| n. Supervision of disembarkation of aircraft. | ○ |
| Definitions | |||
|---|---|---|---|
| No | Criteria/items | Definition | Nomenclature |
| 1 | Type of aircraft | Fixed wing/rotary wing | FW/RW |
| 2 | Patient severity | Low: low: ambulatory, non-life-threatening patient. | B/M/A |
| Medium: non-life-threatening patient, requires intermediate level of care | |||
| High: life-threatening patient, intubated with VAD, ECMO, EVD and/or plural drain. | |||
| 3 | ASC condition | Military/civil/mixed | M/C/Mx |
| 4 | ASC members | Doctor/nurse/nursing assistant | D/N/A |
| 5 | Transfer time | ---------------------------------------------------------------- | In hours |
| 6 | National/international | ---------------------------------------------------------------- | N/I |
| 7 | Type of isolation | Aerial/droplets/contact | A/G/C |
| 8 | Aircraft configuration | Clean area (ASC rest area), intermediate area (PPE change area) and contaminated area (Patient area) | |
CVC: central venous catheter; ECMO: extracorporeal membrane oxygenation; EVD: external ventricular drainage; HCWN: healthcare waste management; HFNAC: high-flow nasal cannula; NBZ: nebulisers; NGT: nasogastric tube; NIV: non-invasive mechanical ventilation; NPTLOX: new generation portable therapeutic liquid oxygen system; NVG: night vision goggles; OTT: orotracheal tube; PPE: personal protective equipment; VAD: vasoactive drugs. OBSERVATIONS/INCIDENTS:
____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________.
The HICPAE aero-evacuation missions of COVID-19 patients consider multiple factors, which is why the management carried out by nurses specialised in aero-evacuation is one of the components established in the planning, which is the fundamental structure of the preparation of the mission, and is related to the execution of the process in a sequential manner, with established guidelines so that all the areas that comprise it, from the strategic to the operational, are under strict quality standards. Operationally, the use of fixed and rotary wing flight equipment is used according to the number and complexity of the patients, within which an optimal configuration must be executed, to establish and condition the isolation systems, with their respective safety areas, operated by aerosanitary crews with a high degree of experience at both strategic and operational level in the management of the patient unit in flight, highlighting that they have a role as a team and also with responsibilities according to their specialty, regardless of the origin of these crews, whether civilian or military. It is essential that they are familiar with the aircraft and the procedures within it, the transfer times, which allows them to plan various aspects of aero-evacuation such as oxygen levels, supplies, drugs, which can be carried out in a national and international context.
The selection and assessment of the severity of the patient are key aspects to consider, on which the decision to airlift depends. In terms of care, the management carried out by nurses specialised in the air transport of infectious patients during the COVID-19 pandemic resulted in the planning, organisation, application of aero-evacuation protocols and pre-flight, flight and post-flight care procedures. On the other hand, it considers aspects of care and operational safety such as training and use of PPE for the ASC, patients and air crew, highlighting the importance of the application of decontamination protocols and handling of REAS.
It can be concluded from the above that the functions of nurses specialised in air transport cover the various areas of air evacuation, from its four main axes, adding aspects of operational safety, applied in the instruction, training, execution and strict control of the work of the ASC as a consolidated team, contributing to the success of the air evacuation mission and to a high probability of survival of the infectious patient in the COVID-19 pandemic.
FundingThis study did not receive any type of funding.
Conflict of interestsThe authors have no conflict of interests to declare.

