


The prevalence of allergic diseases is increasing. We evaluated temporal trends in the prevalence of asthma, rhinitis and eczema in adolescents (13–14 years) living in Taubaté, SP, Brazil (2005–2012) and assessed the relationship between these prevalences and the residential proximity to Presidente Dutra Highway (PDH, a heavily travelled highway).
MethodsThis cross-sectional study of adolescents (N=1039) from public and private schools was evaluated using the standard questionnaire of the International Study of Asthma and Allergies in Childhood (ISAAC) plus a question about their place of residence in relation to PDH. The data obtained were compared to the 2005 data using a chi-square test or Fisher's exact test. An analysis by groups consisting of two phases (two-step cluster) was used to evaluate the effect of living near PDH.
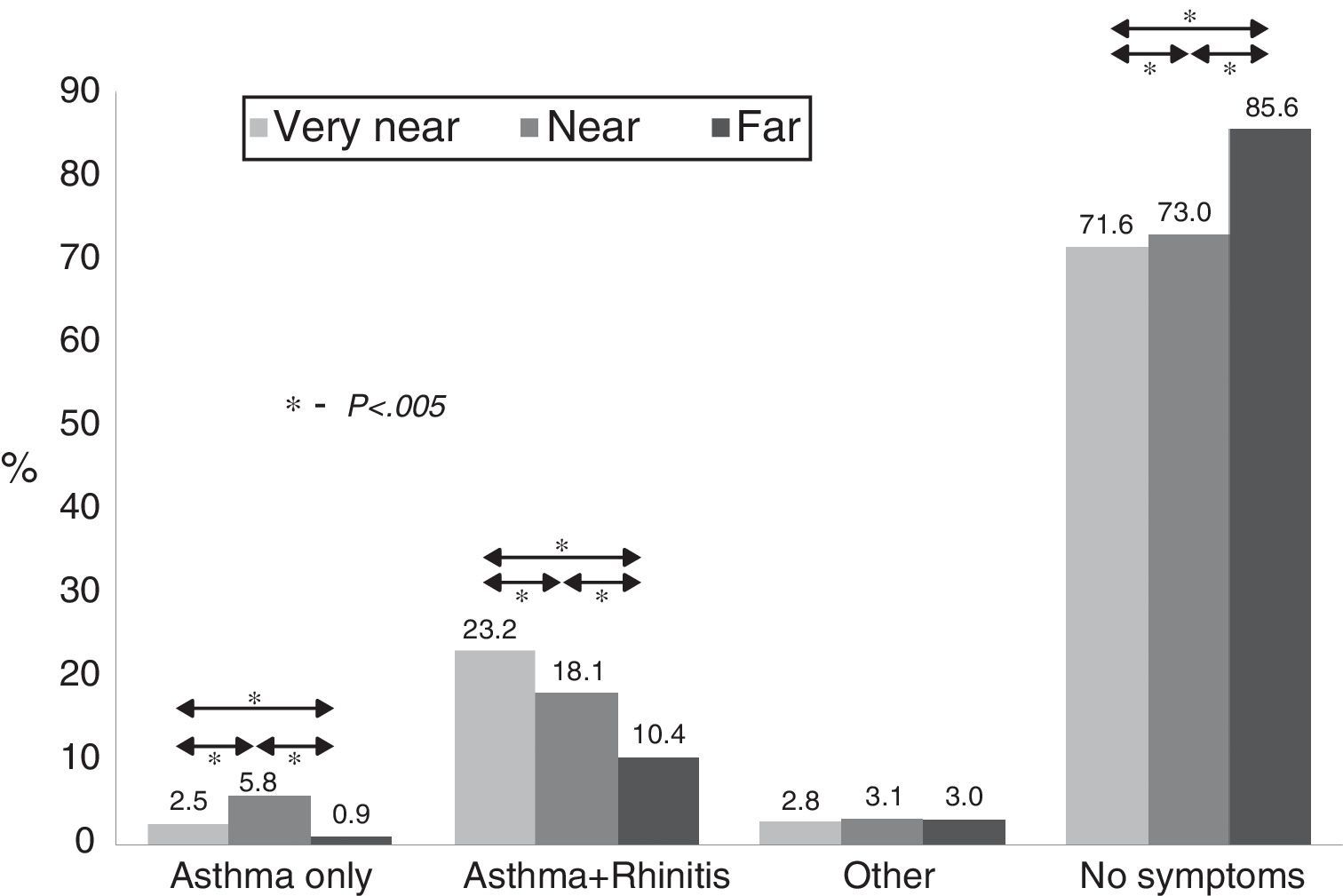
ResultsThere was a lifetime increase in the prevalence of active asthma (15.3% vs. 20.4%, p=0.005) and physician-diagnosed asthma (6.8% vs. 9.2%, p=0.06) and a decrease in the symptoms of active rhinitis (36.6% vs. 18.5%) between 2005 and 2012. A high frequency of asthma and rhinitis (18.1% vs. 23.2%, respectively) was observed among adolescents living close or very close to PDH; furthermore, 85.6% of the adolescents without symptoms of asthma or rhinitis lived far from PDH.
ConclusionAn increase in the prevalence of asthma and a decrease in the prevalence of rhinitis were observed during the studied period. Living near PDH was associated with higher rates of asthma, rhinitis, and eczema.
The lack of specific diagnostic tests for asthma, rhinitis, and eczema and the use of different assessment methods have prevented the gathering of information about the prevalence of these diseases in epidemiological studies. The International Study of Asthma and Allergies (ISAAC) was a turning point in the epidemiological study of asthma, rhinitis and eczema in the paediatric population.1,2
The ISAAC enabled temporal comparisons of the prevalence of asthma and allergic diseases in different regions and among regions within a country.2,3 It allowed the identification of annual increases in the prevalence of asthma among adolescents in several parts of the world, including Africa (+0.16%), Latin America (+0.32%), Northern Europe (+0.26%), Eastern Europe (+0.26%) and India (+0.02%). In contrast, in other regions, such as Oceania (−0.76%), the disease prevalence remained stable or even decreased.3 ISAAC also reported an increase in the prevalence of rhinitis and eczema, especially in Asia-Pacific countries and in India.3
Solé et al.4 assessed seven Brazilian cities over a 9-year period and found that in 2012, the prevalence of active asthma (wheezing in the last 12 months) among adolescents was highest in São Paulo, in the state of São Paulo (SP) (21.3%), and lowest in Aracaju, in the state of Sergipe (SE) (12.8%). The prevalence of rhinitis was also highest in São Paulo (SP) (47.4%) and lowest in Recife, in the state of Pernambuco (PE) (26.3%), while the prevalence of eczema was highest in Belém, in the state of Pará (PA) (7.9%) and lowest in Aracaju (SE) (3.4%).
Although genetic factors are involved in the occurrence of asthma, their interaction with environmental factors may explain the international variation in the prevalence of this disease.5
Several studies identified air pollution as one of the key risk factors for developing or triggering asthma.6,7,8,9,10 The exposure of asthmatic patients to air pollutants causes oxidative stress over time, which results in damage to the bronchial epithelium, increased airway inflammation, increased bronchial responsiveness and allergic sensitisation.11,12
A study conducted in the city of São José dos Campos, Paraíba Valley (SP) demonstrated a significant relationship between air pollutants and an increased number of asthma-related hospitalisations among children up to 10 years of age.13
The city of Taubaté (SP) is crossed by the President Dutra Highway (PDH), which is considered the most important Brazilian highway because it links the two main national metropolises (Rio de Janeiro and São Paulo) and passes through one of the richest areas in the country, the Paraíba Valley. The cities located at the margins of the PDH have undergone rapid expansion, conurbation, and industrialisation in recent years.14
The lack of studies investigating the effects of pollutants on the respiratory health of adolescents with asthma and other allergic diseases in Taubaté (SP) prompted our interest in studying these effects and assessing temporal trends in the prevalence of asthma, rhinitis, and eczema in this municipality.
Materials and methodsThis epidemiological cross-sectional study was conducted in the city of Taubaté (SP), which is located 142km from São Paulo, the state capital. The study included adolescents aged from 13 to 14 years old attending randomly selected public and private schools. The students were asked to answer the ISAAC written questionnaire (ISAAC-WQ) plus one question about the location of their residences in relation to PDH. The participants and their parents/guardians signed informed assent and consent forms, respectively, before their inclusion in the study. The sample size was calculated based on a prevalence of active asthma of 15.3%,15 80% power, 5% alpha error and a 4% confidence interval, which resulted in an initial sample size of 500 adolescents. However, considering possible losses of 25% and the stratification of the study population into groups and subgroups, N was increased to a minimum of 1000 participants. This present study included only adolescent population in order to make comparisons easier once we used the same age group in a previous study.15
According to the answers to the ISAAC-WQ, adolescents were classified as having: active asthma (i.e., those who answered “yes” to the question “Have you had wheezing or whistling in the chest in the last 12 months?”), active rhinitis (those who answered “yes” to the question “In the past 12 months, have you had a problem with sneezing or a runny nose or a blocked nose when you did not have a cold or the flu?”) or eczema (those who answered “yes” to the question “Have you had an itchy rash at any time in your life?”).3
The severity of asthma was assessed based on the frequency and severity of symptoms.16
Based on the symptoms exhibited, adolescents were divided into various subgroups: no allergy symptoms; asthma only; asthma+rhinitis, and other (asthma, rhinitis, and atopic dermatitis). According to their place of residence (proximity to PDH), the participants were divided into the following groups: residing near PDH (N, 200m to 1km), very near PDH (VN, less than 200m) or far from PDH (F, more than 1km away). These distances were mainly established based on data provided by the “Departamento Nacional de Infraestrutura de Transportes” (DNIT), which recommends a minimum distance of 1km between residential areas and two-lane highways17 and in another study that establishes similar distances from the residences to the highways.10 Data were collected from January to December 2012. The data were entered in a standard spreadsheet (Excel) and then transferred to SPSS 20.0 software for statistical analysis.
Statistical analysisThe data were expressed as simple percentages and were compared with the 2005 data15 using a chi-square test or Fisher's exact test. Cluster analysis was performed to identify homogeneous groups according to the presence of asthma, rhinitis and eczema (based on reported symptoms in the last 12 months) and place of residence. Two-step cluster analysis and the Schwarz–Bayes Information Criterion (SBIC) were used to investigate the similarities and differences among the investigated variables.18,19 The level of significance was set to 5%. The study was approved by the Ethics and Research Committees of Hospital São Paulo, Escola Paulista de Medicina – Federal University of São Paulo and University of Taubaté (UNITAU).
ResultsA total of 1039 adolescents (51.9% males) participated in the study. Of these, 60.1% were enrolled in public schools, and 39.9% were enrolled in private schools.
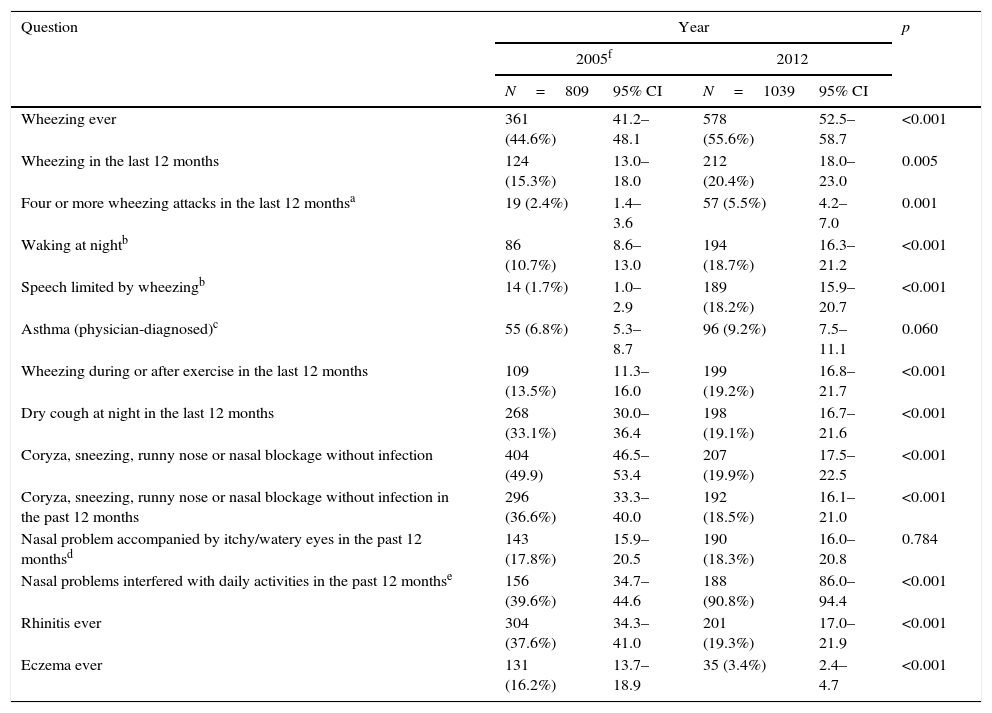
Table 1 describes the prevalence of asthma symptoms, rhinitis-related symptoms and the occurrence of eczema among the adolescents for each study year and the comparative analysis. The results showed significant increases in all asthma symptoms except physician-diagnosed asthma, which showed an increasing trend, and dry cough at night over the last 12 months, which exhibited a significant decrease. Regarding rhinitis-related symptoms (Table 1), the comparative analysis showed a significant reduction in “coryza, sneezing or nasal obstruction in the absence of infection”, “coryza, sneezing or nasal obstruction in the absence of infection in the last 12 months” and in the occurrence of “rhinitis.” However, the prevalence of “nasal problems interfering with daily activities within the past 12 months” showed a significant increase. A significant decrease in the prevalence of atopic eczema from 16.2% to 3.4% was observed (Table 1).
Prevalence of asthma-related symptoms, of rhinitis-related symptoms and of eczema ever among adolescents by study year.
| Question | Year | p | |||
|---|---|---|---|---|---|
| 2005f | 2012 | ||||
| N=809 | 95% CI | N=1039 | 95% CI | ||
| Wheezing ever | 361 (44.6%) | 41.2–48.1 | 578 (55.6%) | 52.5–58.7 | <0.001 |
| Wheezing in the last 12 months | 124 (15.3%) | 13.0–18.0 | 212 (20.4%) | 18.0–23.0 | 0.005 |
| Four or more wheezing attacks in the last 12 monthsa | 19 (2.4%) | 1.4–3.6 | 57 (5.5%) | 4.2–7.0 | 0.001 |
| Waking at nightb | 86 (10.7%) | 8.6–13.0 | 194 (18.7%) | 16.3–21.2 | <0.001 |
| Speech limited by wheezingb | 14 (1.7%) | 1.0–2.9 | 189 (18.2%) | 15.9–20.7 | <0.001 |
| Asthma (physician-diagnosed)c | 55 (6.8%) | 5.3–8.7 | 96 (9.2%) | 7.5–11.1 | 0.060 |
| Wheezing during or after exercise in the last 12 months | 109 (13.5%) | 11.3–16.0 | 199 (19.2%) | 16.8–21.7 | <0.001 |
| Dry cough at night in the last 12 months | 268 (33.1%) | 30.0–36.4 | 198 (19.1%) | 16.7–21.6 | <0.001 |
| Coryza, sneezing, runny nose or nasal blockage without infection | 404 (49.9) | 46.5–53.4 | 207 (19.9%) | 17.5–22.5 | <0.001 |
| Coryza, sneezing, runny nose or nasal blockage without infection in the past 12 months | 296 (36.6%) | 33.3–40.0 | 192 (18.5%) | 16.1–21.0 | <0.001 |
| Nasal problem accompanied by itchy/watery eyes in the past 12 monthsd | 143 (17.8%) | 15.9–20.5 | 190 (18.3%) | 16.0–20.8 | 0.784 |
| Nasal problems interfered with daily activities in the past 12 monthse | 156 (39.6%) | 34.7–44.6 | 188 (90.8%) | 86.0–94.4 | <0.001 |
| Rhinitis ever | 304 (37.6%) | 34.3–41.0 | 201 (19.3%) | 17.0–21.9 | <0.001 |
| Eczema ever | 131 (16.2%) | 13.7–18.9 | 35 (3.4%) | 2.4–4.7 | <0.001 |
p, chi-square test or Fisher Exact test; 95% CI, 95% confidence interval.
Fig. 1 shows the distribution of the adolescents according to the symptoms presented and place of residence. Most (85%) who lived far from PDH did not exhibit any disease in the previous 12 months. However, those who lived near or very near PDH exhibited a significantly higher frequency of disease. The combination of asthma and rhinitis was more frequently reported by participants who lived near the highway than by those who lived far from it (23.2% vs. 10.4%); the same pattern was observed for the occurrence of asthma only (5.8% vs. 0.9%).
Discussion, near (from 200m to 1km) or far (more than 1km away).")
This cross-sectional study analyses the prevalence of asthma, rhinitis, and eczema and the association between traffic-related air pollution and adverse respiratory and skin health effects in Brazilian adolescents (13–14 years) in 2012. A cross-sectional study with the same methodology was done in 2005 and was used by the authors for comparison of prevalence of asthma and rhinitis symptoms and eczema over time. However, in the 2005 study the effect of air pollution on respiratory and skin health was not evaluated.15
This current study has showed an increase on prevalence of asthma and decrease on prevalence of rhinitis and eczema when it was compared in both of our surveys over time.
In the present study, we have found an increase in the prevalence of active asthma and physician-diagnosed asthma compared to the previous study.15 There was also a possible increase in severity of asthma, particularly asthma symptoms during and after physical exercise (Table 1).
Some studies applying the same methodology have showed similar results. A study assessing temporal trends in the prevalence of asthma among Brazilian adolescents observed a reduction in the average prevalence of active asthma, while the number of cases of severe asthma and physician-diagnosed asthma increased.20 Another temporal study observed an increase on prevalence of asthma and a reduction in the frequency of physician-diagnosed rhinitis.21
The aforementioned increase in the prevalence of active asthma among adolescents from Taubaté from 2005 to 2012 might be related to improvements in asthma diagnoses and treatment starting in the 2000s. The establishment of the National Plan for the Control of Asthma (Plano Nacional de Controle da Asma – PNCA) and the national pharmaceutical care programme in 2010 were also helpful, as previously observed.4 The implementation of medical guidelines might have helped to disseminate the term “asthma” among doctors and to more thoroughly standardise the treatment of disease in an empirical manner.22
Although living near a highway was not studied in 2005, the present study has showed that the residential proximity of a highway was an important risk factor for asthma and may be associated with the increase in the prevalence of this disease among adolescents from Taubaté and also might be related to the increase in automotive vehicle fleets between 2005 and 2012.23 This factor is supported by other studies that found a relationship between increased emissions of harmful gases from vehicles and higher asthma prevalences.24,25
Although we did not have data on the toxic emissions from the heavy traffic on PDH, we could establish that the prevalence of asthma and other allergic diseases was higher among the participants who lived near or very near the highway, similar to the observations of other studies.9,10
Despite the decrease in the rhinitis prevalence among adolescents in Taubaté from 2005 to 2012, there was an increase in the “nasal problems interference with daily activities in the past 12 months”. Although rhinitis is considered a trivial and/or transient disease that is less severe than asthma, it can considerably impair the patients’ quality of life, performance, learning at school and productivity at work. The physical, psychological, and social impacts of rhinitis are numerous and affect adults as well as children and adolescents.26
The increase in the severity of rhinitis and asthma symptoms observed in the present study might be associated with inadequate treatment or inadequate monitoring of treatments. A lack of adherence to asthma treatment is common among adolescents.27 Acknowledgement of the central role that patients play in the management of their chronic diseases, including asthma and allergies, patient education makes a major component of the global treatment of such conditions.28 Certainly, after the epidemiological studies as ISAAC and International treatment guidelines for asthma, there was an improvement in diagnosis, especially for asthma. In our country, a better diagnostic was not followed by better control of this disease, which may partly explain the major severity found.
In this study, the association between asthma and rhinitis symptoms was the most frequent presentation. Those diseases are known to exhibit similar inflammatory mechanisms, and they frequently coexist in the same patient.29,30 In study conducted in Fortaleza, Ceará20 the results also showed a significant association between asthma and rhinitis symptoms.
The hypothesis that asthma and rhinitis are different expressions of a single airway disease has consolidated and strengthened the need to develop therapies that target this comorbidity in an integrated manner.31
In our study, a comparison of the prevalence rates over a 7-year period demonstrated an increased prevalence of asthma and a decreased prevalence of rhinitis and atopic dermatitis in the same study area and under conditions very similar to those of the previous study.15 We believe it likely that by having increased prevalence and severity of asthma symptoms, the symptoms of rhinitis might have been underestimated by adolescents.
The prevalence of asthma and allergy has been widely investigated in the past decades worldwide; however, there is still no consensus on the reasons for the variability in disease prevalence, including the variation in allergic symptoms in different study regions. Genetic, phenotypic and environmental factors might influence those differences,8,9,32,33,34 which would thus partially explain the differences in the prevalence of the investigated allergic diseases found among the adolescents from Taubaté (SP).
In conclusion, there was an increase in prevalence of active asthma and although physician-diagnosed asthma has also increased, it was not significant. The prevalence of rhinitis and eczema decreased in the city of Taubaté (SP) from 2005 to 2012. The severity of rhinitis increased, and the frequency of asthma and rhinitis symptoms was higher among the adolescents who lived near the PDH than those who lived far from the highway.
Ethical disclosuresConfidentiality of dataThe authors declare that they have followed the protocols of their work centre on the publication of patient data and that all of the patients included in the study have received sufficient information and have given their informed consent in writing to participate in the study.
Right to privacy and informed consentThe authors must have obtained the informed consent of the patients and/or subjects mentioned in the article. The author for correspondence must be in possession of this document.
Protection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the responsible Clinical Research Ethics Committee and in accordance with those of the World Medical Association and the Helsinki Declaration.
Conflict of interestThe authors have no conflict of interest to declare.
