
The aim of the study was to analyze the clinical-demographic variables of the series and the predictors of urethral stricture recurrence after endoscopic urethrotomy.
Material and methodsWe retrospectively analyzed 67 patients who underwent Sachse endoscopic urethrotomy between June 2006 and September 2014. Those patients who had previously undergone endoscopic urethrotomy or urethroplasty were excluded. The other patients who presented urethral stricture were included.
We analyzed age, weight, smoking habit, and cardiovascular risk factors, as well as the number, location, length and etiology of the strictures, previous urethrotomies, vesical catheter duration and postsurgical dilatations.
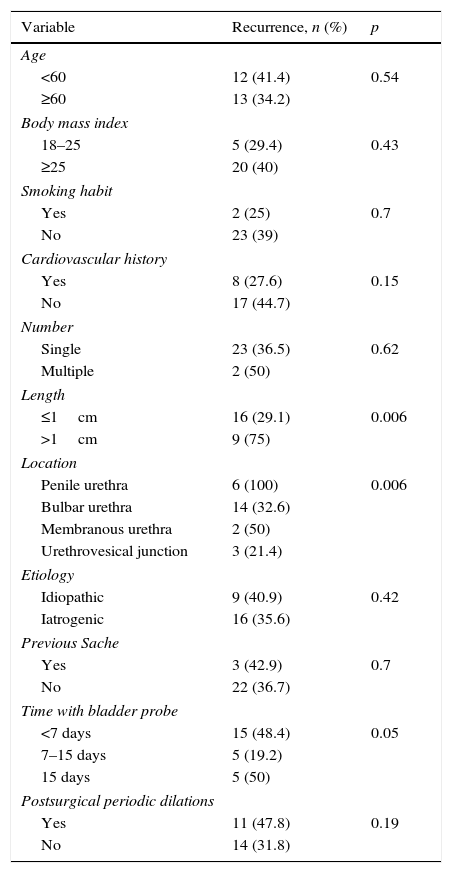
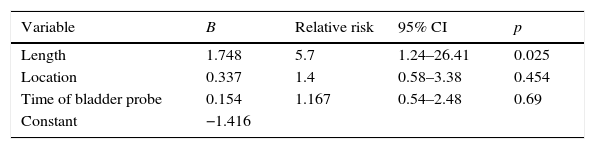
A univariate and multivariate analysis was conducted using the chi-squared test or Fisher's test and logistic regression to identify the variables related to recurrence.
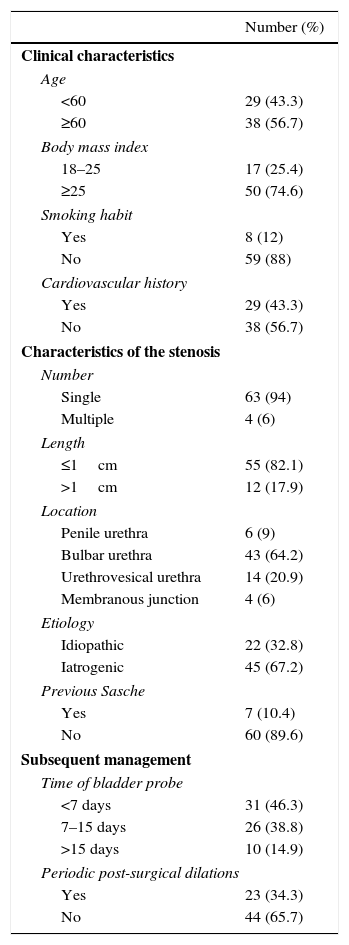
ResultsThirty-seven percent of the patients had a relapse. The majority of the patients were older than 60 years (56.7%), obese (74.6%), nonsmokers (88%) and had no cardiovascular factors (56.7%). The majority of the strictures were single (94%), <1cm (82%), bulbar urethral (64.2%), iatrogenic (67.2%) and with no prior urethrotomy (89.6%). The majority of the patients carried a vesical catheter for <15 days (85.1%) and did not undergo postsurgical dilatation (65.7%).
Only the length of the stricture was an independent risk factor for recurrence (p=.025; relative risk, 5.7; 95% CI 1.21–26.41).
ConclusionsIn the treatment of urethral strictures through endoscopic urethrotomy, a stricture length >1cm is the only factor that predicts an increase in the risk of recurrence. We found no clinical or demographic factors that caused an increase in the incidence of recurrence. Similarly, technical factors such as increasing the bladder catheterization time and urethral dilatations did not change the course of the disease. Their routine use is therefore unnecessary.
El objetivo del trabajo fue analizar las variables clínico-demográficas de la serie y los factores predictores de recidiva de estenosis uretral tras uretrotomía endoscópica.
Material y métodosSe analizó retrospectivamente a 67 pacientes tratados mediante uretrotomía endoscópica tipo Sachse entre junio de 2006 y septiembre de 2014. Se excluyó a los intervenidos previamente de uretrotomía endoscópica o uretroplastia y se incluyó al resto de los pacientes que presentaban estenosis uretral.
Se analizó edad, peso, hábito tabáquico, factores de riesgo cardiovascular, número, localización, longitud y etiología de la estenosis, uretrotomía previa, tiempo de sonda vesical y dilataciones posquirúrgicas.
Se realizó un análisis univariado y multivariado mediante el test de chi-cuadrado o de Fisher y regresión logística para identificar las variables relacionadas con la recidiva.
ResultadosEl 37% recidivaron. La mayoría eran>60 años (56,7%), obesos (74,6%), no fumadores (88%) y sin factores cardiovasculares (56,7%). La mayoría de las estenosis fueron únicas (94%),<1cm (82%), de uretra bulbar (64,2%), iatrogénicas (67,2%) y sin uretrotomía previa (89,6%). La mayoría llevaron sonda vesical durante<15 días (85,1%) y no realizaron dilataciones posquirúrgicas (65,7%).
Solamente la longitud de la estenosis resultó factor de riesgo independiente de recidiva (p=0,025) con un riesgo relativo de 5,7 para un IC 95% (1,21-26,41).
ConclusionesEn el tratamiento de la estenosis uretral mediante uretrotomía endoscópica, la longitud de la estenosis >1cm es el único factor que predice un incremento del riesgo de recidiva. No se encontró factores clínicos ni demográficos que condicionaran un incremento en la incidencia de recidiva. Del mismo modo, factores técnicos como incrementar el tiempo de sondaje vesical o las dilataciones uretrales no alteran el curso de la enfermedad, por lo que su uso rutinario es innecesario.