






Locoregional recurrence occurs in up to 28% of patients with papillary thyroid cancer (PTC). Several risk factors contribute to this metastatic process. The latest of them is perinodal infiltration (PNI). PNI refers to the pathological extension of tumor cells through the lymph node (LN) capsule into the perinodal fibroadipose tissue. It has been accepted as a poor predictive variable. This study aimed to evaluate the prognostic significance of PNI in recurrence of PTC and identify predictive parameters associated with the recurrence in PNI (+) patients.
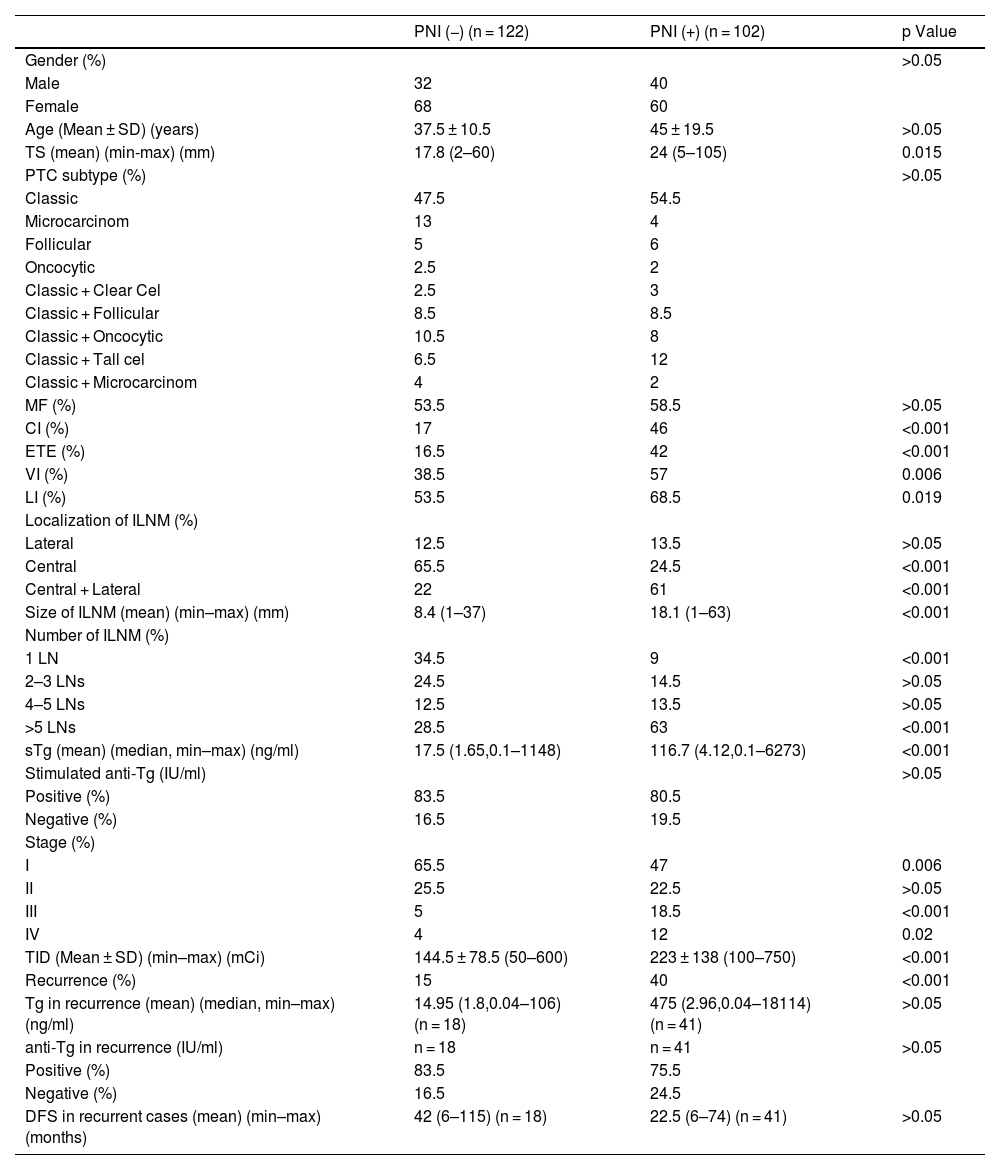
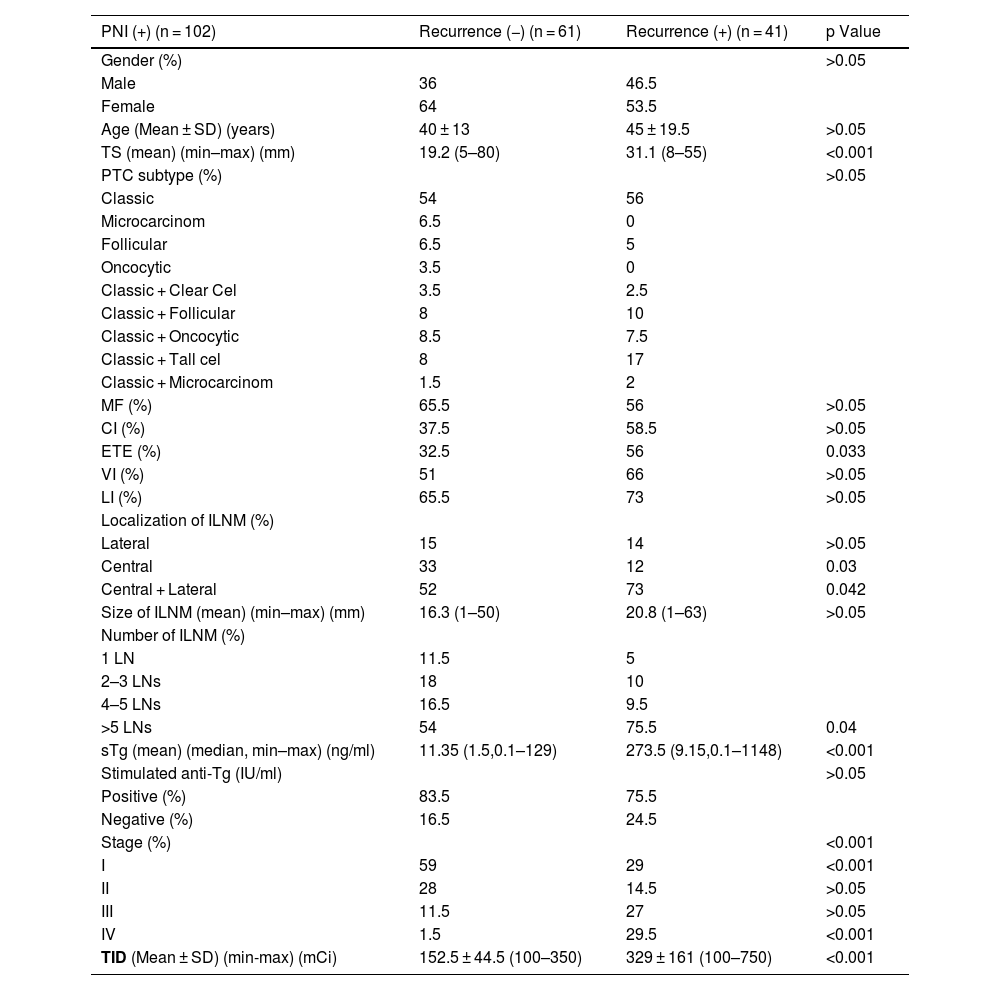
Material and methodsThe study included 680 PTC patients with initial LN metastasis (ILNM). Study population was selected from them according to presence or absence of PNI. Eventually, 102 PNI (+) and 122 PNI (−) patients remained eligible for the study. Patients were statistically compared according to demographic, clinicopathologic features both between PNI (+) and PNI (−) groups and within the PNI (+) group over recurrence status.
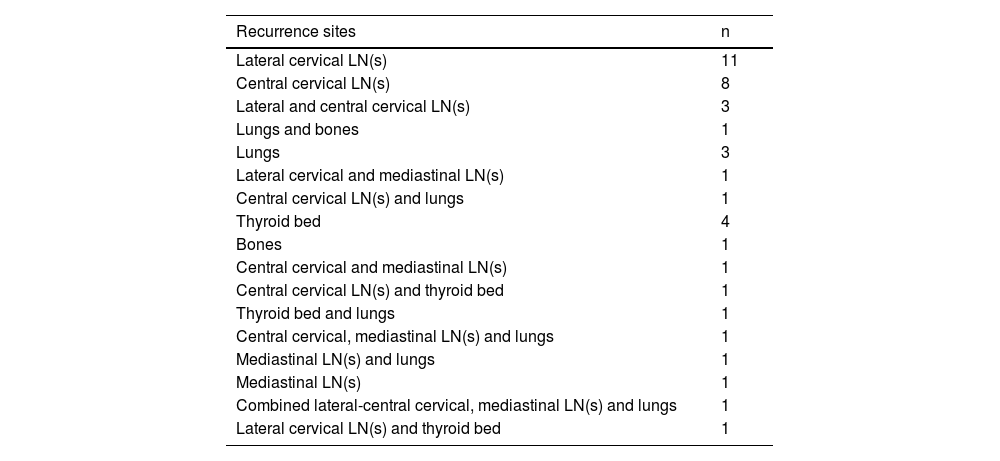
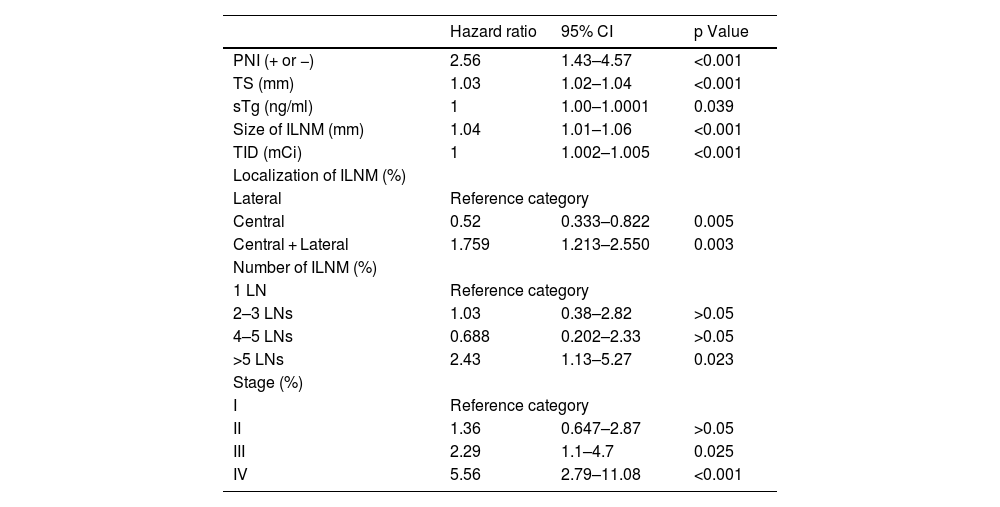
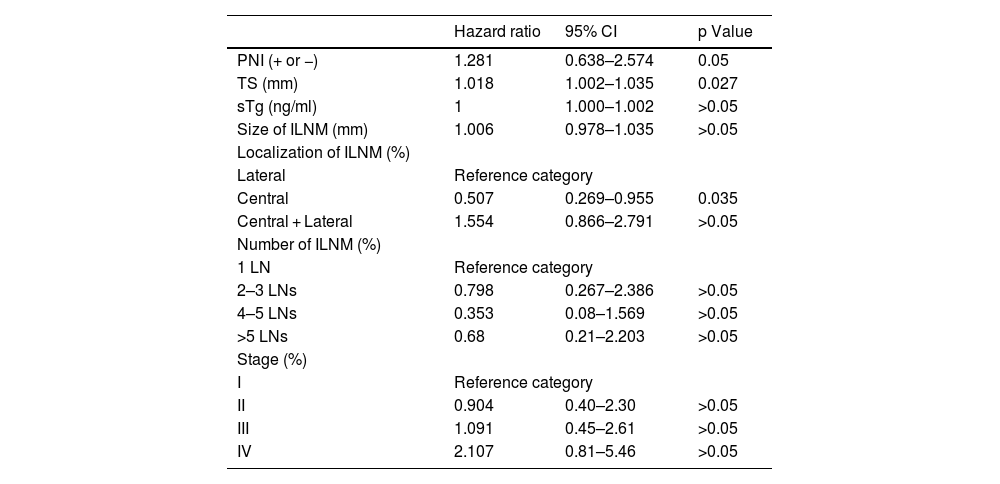
ResultsThe recurrence rates were 40% and 15% in PNI (+) and PNI (−) patients, respectively (p < 0.001). The independent predictive factors associated with recurrence were central ILNM (p = 0.005), combined central and lateral ILNM (p = 0.003), ILNM > 5 (p = 0.023), stage III–IV (p = 0.025 and p < 0.001), tumor size (TS) (p < 0.001), ILNM size (p < 0.001), stimulated thyroglobulin (sTg) (p = 0.039). PNI (p = 0.05), central ILNM (p = 0.035) and TS (p = 0.027) remained prognostic variables after multivariate analysis.
ConclusionPNI positivity is a poor prognostic factor for PTC recurrence. PNI, especially with large TS and central ILNM, should be taken into account when planning RAI therapy in PTC patients.
La recurrencia locorregional se presenta hasta en el 28% de los pacientes con carcinoma papilar de tiroides (CPT). Diversos factores de riesgo contribuyen a este proceso metastásico, siendo el más recientemente reconocido la infiltración perinodal (IPN). La IPN se define como la extensión patológica de células tumorales a través de la cápsula del ganglio linfático (GL) hacia el tejido fibroadiposo perinodal. Actualmente se considera un factor predictivo de mal pronóstico. El objetivo de este estudio fue evaluar la importancia pronóstica de la IPN en la recurrencia del CPT e identificar los parámetros predictivos asociados a la recurrencia en pacientes con IPN positiva.
Materiales y métodosEl estudio se realizó en 680 pacientes con CPT y metástasis ganglionar inicial (MGI). La población del estudio se seleccionó en función de la presencia o ausencia de IPN. Finalmente, 102 pacientes con IPN (+) y 122 con IPN (−) cumplieron los criterios de inclusión. Se realizaron comparaciones estadísticas entre los grupos IPN (+) e IPN (−), así como dentro del grupo IPN (+) según el estado de recurrencia, teniendo en cuenta variables demográficas, clínicopatológicas, terapéuticas y de desenlace.
ResultadosLas tasas de recurrencia fueron del 40% en los pacientes con IPN (+) y del 15% en aquellos con IPN (–) (p < 0.001). Los factores predictivos independientes asociados con la recurrencia fueron: MGI central (p = 0.005), MGI central y lateral combinada (p = 0.003), más de 5 G L metastásicos iniciales (p = 0.023), estadios III–IV (p = 0.025 y p < 0.001), tamaño tumoral (TT) (p < 0.001), tamaño del GL metastásico inicial (p < 0.001) y niveles de tiroglobulina estimulada (sTg) (p = 0.039). Tras el análisis multivariado, la IPN (p = 0.05), la MGI central (p = 0.035) y el TT (p = 0.027) se mantuvieron como variables pronósticas significativas.
ConclusiónLa positividad para IPN representa un factor pronóstico desfavorable para la recurrencia del CPT. La IPN, especialmente en presencia de un gran tamaño tumoral y MGI central, debe considerarse al planificar la terapia con yodo radiactivo (RAI) en pacientes con CPT.
Article
If you experience access problems, you can contact the SEMNIM Technical Secretariat by email at secretaria.tecnica@semnim.es or by phone at +34 619 594 780.
Revista Española de Medicina Nuclear e Imagen Molecular (English Edition)
