









Describir nuestra experiencia en el cateterismo de venas suprarrenales (CVS) y evaluar su utilidad en el diagnóstico y el tratamiento de pacientes con hiperaldosteronismo primario (HAP).
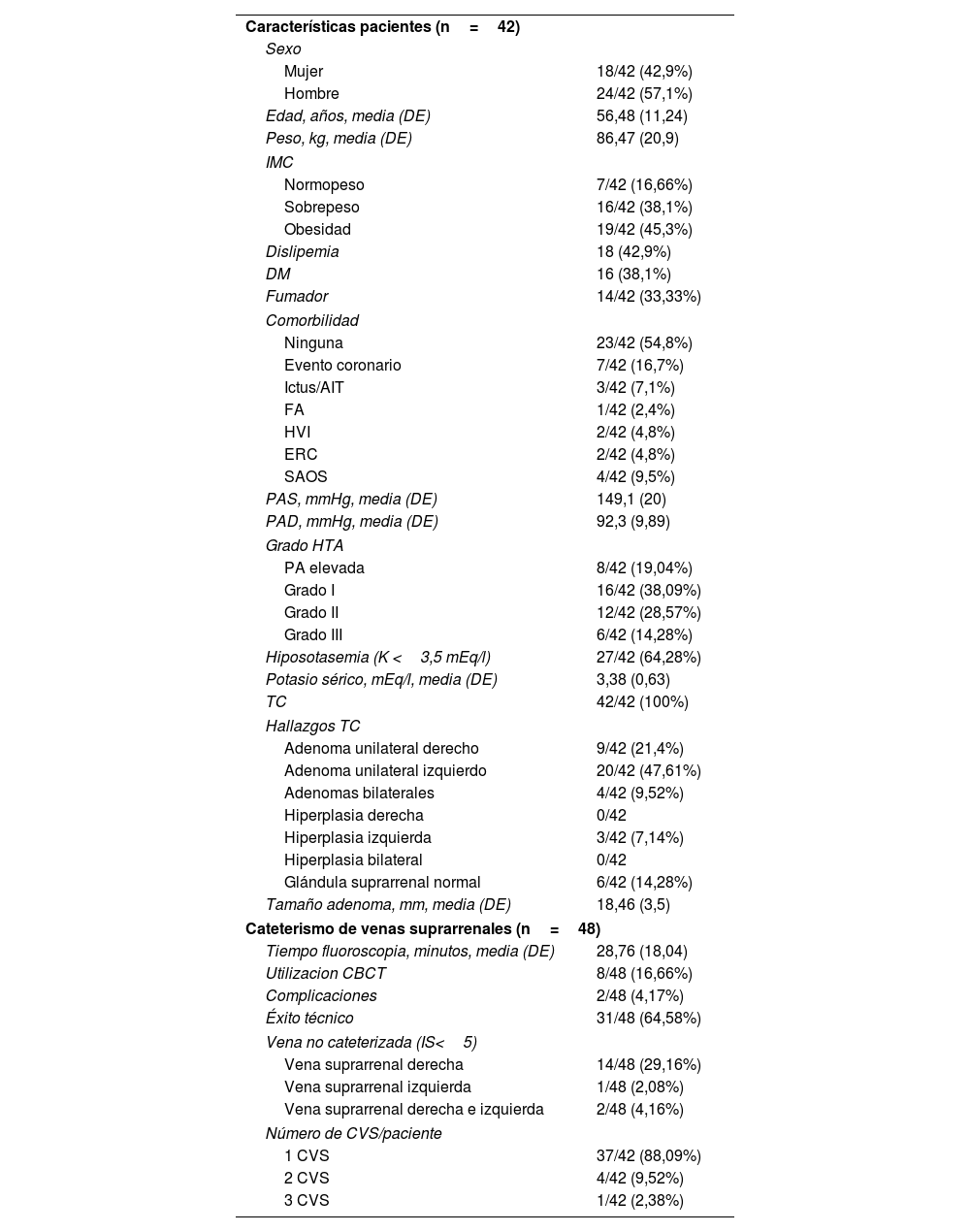
Material y métodosEstudio retrospectivo de 42 pacientes con HAP (57,1% hombres, edad media 56,48años) sometidos a un CVS entre 2020 y 2024. Se recogieron datos clínicos, éxito técnico y complicaciones tras el CVS. Se evaluaron factores relacionados con el éxito técnico y la concordancia entre la TC y el CVS. Se realizó un seguimiento clínico y analítico de hasta 6meses postratamiento.
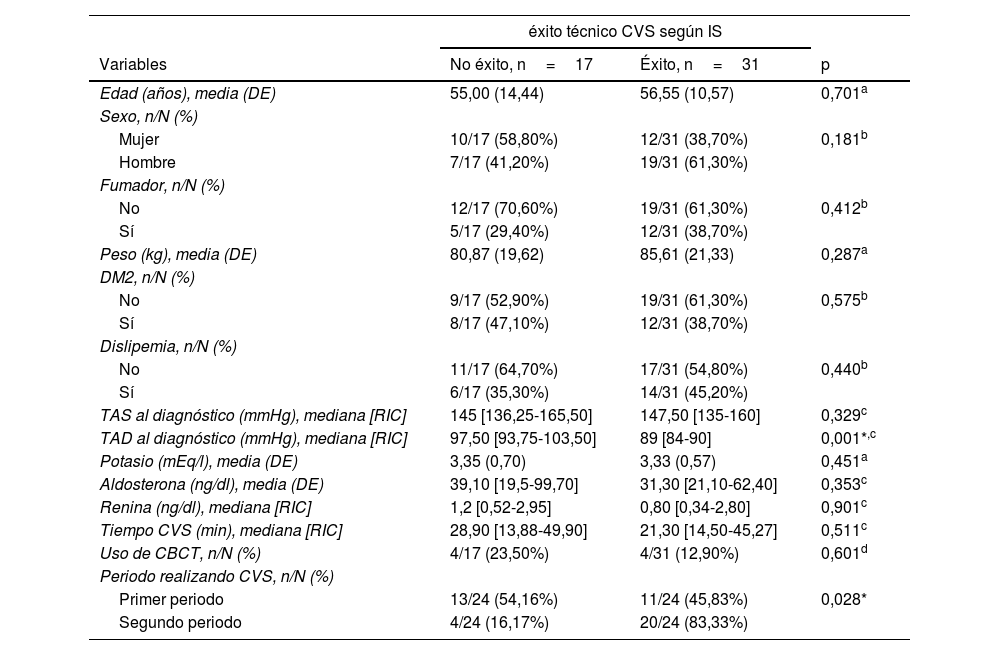
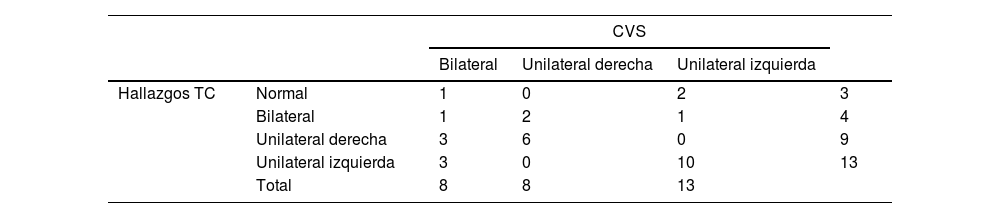
ResultadosTodos los pacientes con HAP tenían hipertensión arterial y tomaban 3fármacos de media. El número de procedimiento/paciente fueron 1 en el 88,4% de los pacientes, 2 en 4 (4,8%) y 3 en un paciente (2,4%). De 48 CVS, 31 fueron exitosos (64,6%) y la tasa de complicaciones fue del 4,16% (2/48). El sexo masculino, el peso <82kg, la presión arterial diastólica <90mmHg y el segundo período realizando CVS se asociaron con mayor éxito técnico del CVS (p=0,016, p=0,026, p=0,032 y p=0,001, respectivamente). La concordancia entre pruebas de imagen y CVS fue del 58,6% (k=0,203; p=0,0005). De 32 pacientes, el 75% redujo número de fármacos. El control de la PA fue mayor en los pacientes con CVS exitoso frente a aquellos con CVS no exitoso (64,51% vs 28,57%) (p=0,032).
ConclusionesEl CVS es una técnica segura con alta tasa de éxito técnico en manos expertas que permitió localizar la hiperproducción de aldosterona y seleccionar a los pacientes con HAP candidatos a adrenalectomía o tratamiento farmacológico reduciendo las cifras tensionales y el número de antihipertensivos.
This work aims to describe our experience with adrenal vein sampling (AVS) and to assess its utility in the diagnosis and management of patients with primary aldosteronism (PA).
Materials and methodsThis retrospective single-centre study enrolled 42 patients with PA (57.1% men, mean age 56.48 years) who underwent AVS between 2020 and 2024. Clinical data, technical success and post-procedural complications were collected. Factors associated with technical success and the concordance between CT findings and AVS results were evaluated. Clinical and laboratory follow-up was carried out for up to six months post-treatment.
ResultsAll patients with PA had hypertension and were taking an average of three antihypertensive medications. The number of procedures per patient was 1 in 37 patients (88%), 2 in 4 patients (4.8%) and 3 in 1 patient (2.4%). In the 48 AVS procedures, 31 were technically successful (64.6%), with a complication rate of 4.16% (2/48). Male sex, body weight <82kg, diastolic blood pressure <90mmHg, and procedures performed during the second time period of AVS practice were associated with higher technical success (P=.016, P=.026, P=.032 and P=.001 respectively). Concordance between imaging and AVS findings was 58.6% (k=.203; P=.0005). During follow-up, 75% of patients reduced the number of medications. Blood pressure control was better in patients with successful AVS compared to those with unsuccessful procedures (64.51% vs. 28.57%, P=.032).
ConclusionsAVS is a safe technique with a high technical success rate in experienced hands, allowing localisation of aldosterone hypersecretion and selection of PA patients for either adrenalectomy or medical treatment, leading to reduced blood pressure levels and a lower number of antihypertensive medications.


