






No existen datos relativos al efecto del tratamiento anticoagulante oral sobre el pronóstico en pacientes con insuficiencia cardiaca aguda (ICA). El objetivo del estudio fue evaluar el efecto del tratamiento anticoagulante oral en el pronóstico a corto y a largo plazo de pacientes con un episodio de ICA que han precisado atención en un Servicio de Urgencias Hospitalaria (SUH).
MétodoEstudio observacional, multicéntrico, prospectivo con seguimiento de cohortes. Se recogieron datos basales y clínicos del episodio de pacientes con ICA en el servicio de urgencias de 41 hospitales españoles. Se realizó un emparejamiento mediante un propensity scores (PS) y se analizó la asociación cruda y ajustada del tratamiento anticoagulante oral con mortalidad a 30 días (objetivo principal) y anual.
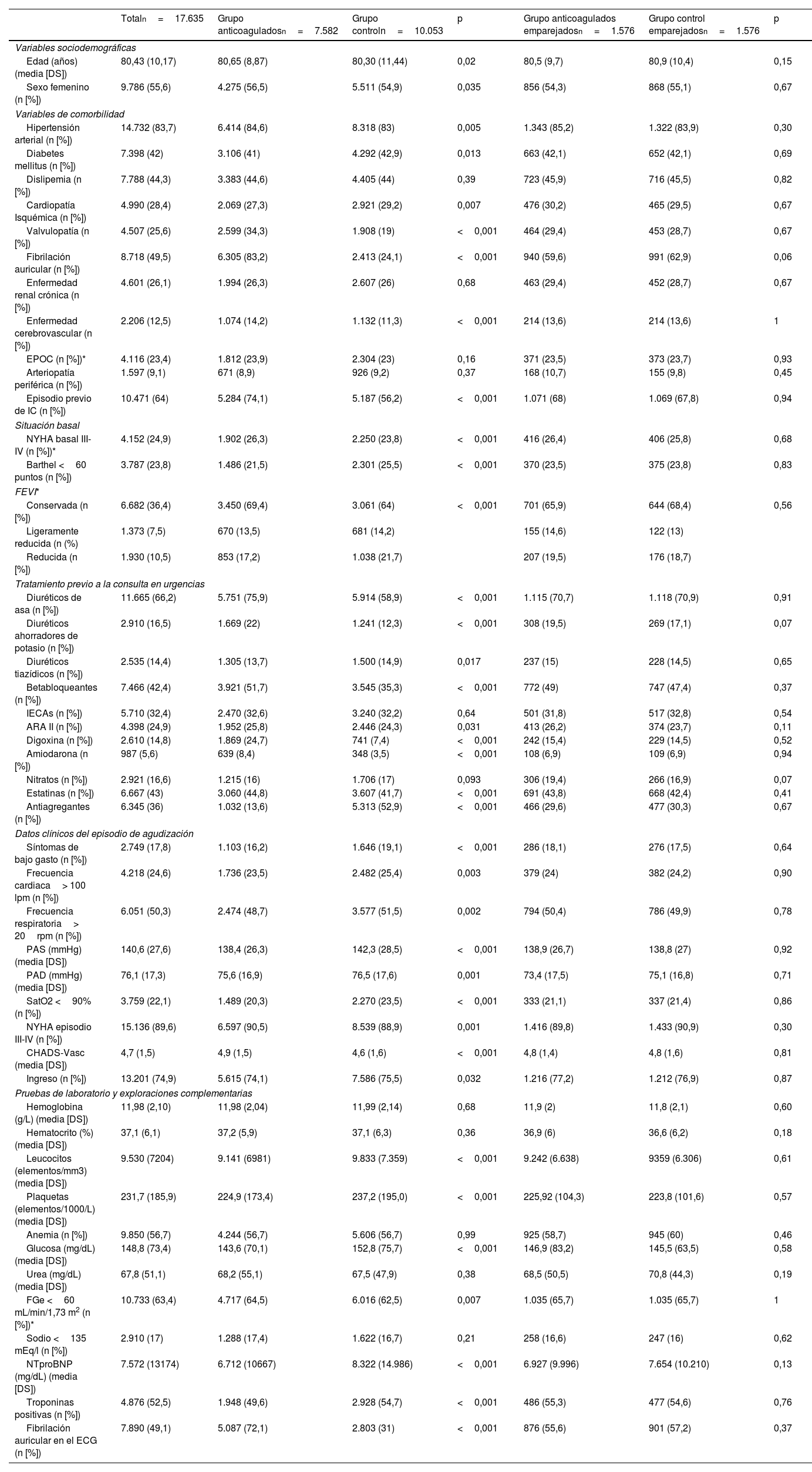
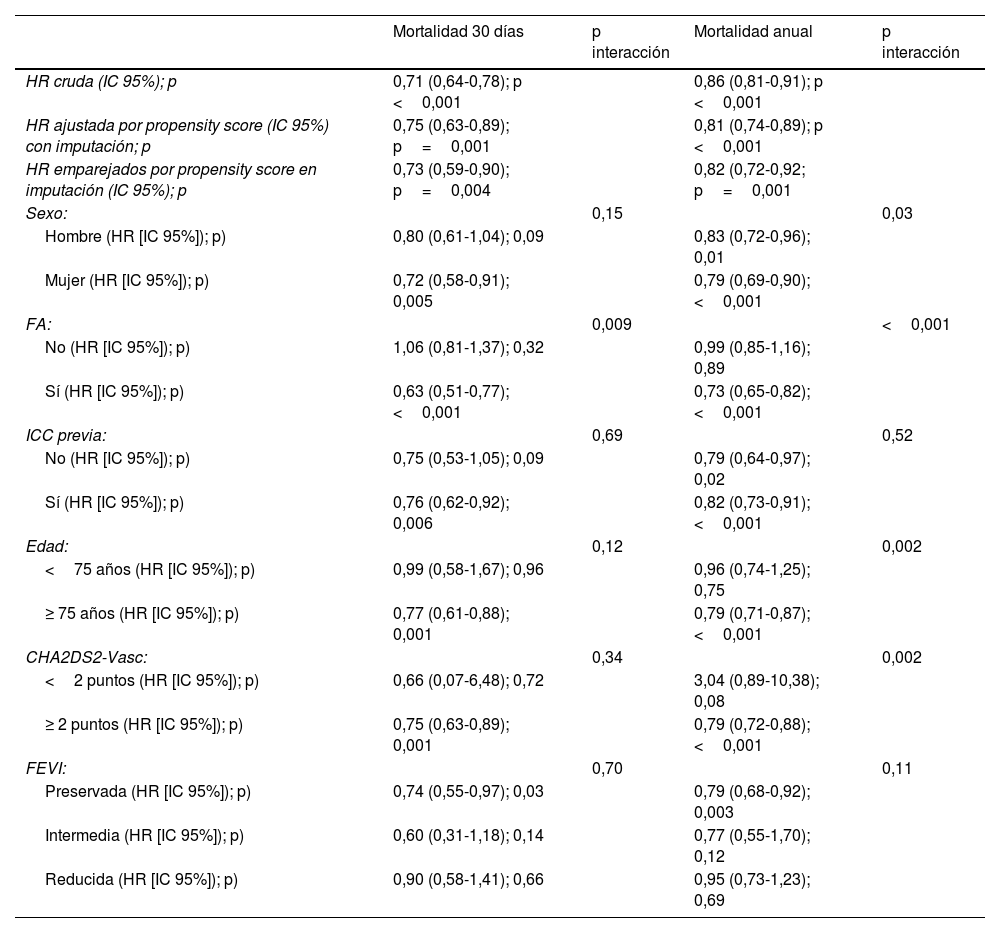
ResultadosSe incluyeron 17.635 pacientes, de los que recibían previamente tratamiento con anticoagulantes orales 42,9%. En comparación con pacientes no anticoagulados, los pacientes anticoagulados tenían una edad media superior (80,6 vs. 80,3, p=0,02), había un predominio del sexo femenino (56,5 vs. 54,9; p=0,035), tenían una alta prevalencia de factores de riesgo y enfermedad cardiovascular y su riesgo trombótico era superior. El pronóstico a 30 días (HR ajustada:0,75 [IC 95%:0,63-0,89]; p <0,001) y al año (HR ajustada: 0,81 [IC 95%:0,73-0,89]; p <0,001) fue mejor en los pacientes del grupo que estaba anticoagulado. Tras el emparejamiento por PS, los resultados no difrerían a los 30 días (HR:0,73 [IC 95%:0,59-0,90]; p <0,001) y al año (HR: 0,82 [IC 95%:0,72-0,92]; p <0,001).
ConclusionesEl tratamiento anticoagulante oral ofrece un beneficio sobre la mortalidad global tanto a corto plazo (30 días) como a largo plazo (anual) en pacientes con ICA atendidos en SUH.
There are no data on the effect of oral anticoagulant treatment on the prognosis of patients with acute heart failure (AHF). This study aimed to evaluate the effect of oral anticoagulant treatment on the short- and long-term prognosis of patients with an episode of AHF requiring hospital emergency department (ED) care.
MethodThis was a prospective, multicentre, observational study with cohort follow-up. Basal and clinical data of the episode of patients diagnosed with AHF in the EDs of 41 Spanish hospitals were collected. Propensity score matching was performed and the crude and adjusted association of oral anticoagulant treatment with mortality was analysed at 30 days (primary objective) and at one year.
ResultsA total of 17635 patients were included, 42.9% of whom were previously receiving oral anticoagulants. Compared with non-anticoagulated patients, anticoagulated patients had a higher mean age (80,6 vs. 80,3, p=0,02), were predominantly female (56,5 vs. 54,9; p=0,035), had a high prevalence of risk factors and cardiovascular disease, and had a higher thrombotic risk. The 30-day [adjusted HR: 0,75 (95% CI: 0,63-0,89); p <0.001] and 1-year [adjusted HR: 0,81 (95% CI: 0,73-0,89); p <0,001] prognosis was better in patients in the anticoagulated group. After propensity score matching, the results did not differ at 30 days [HR: 0,73 (95% CI: 0,59-0,90); p <0,001] and at 1 year [HR: 0,82 (95% CI: 0,72-0,92); p <0,001].
ConclusionsOral anticoagulation may be beneficial in patients with heart failure, regardless of the presence of AF. However, more randomized studies are needed to evaluate this hypothesis.

