






To describe the proportion of patients with liver fibrosis in at-risk populations in primary care (PC). To know the agreement between FIB-4 and transitional elastography (TE), interobserver agreement between PC and hospital care (HC) in TE, and associated risk Factors (RF).
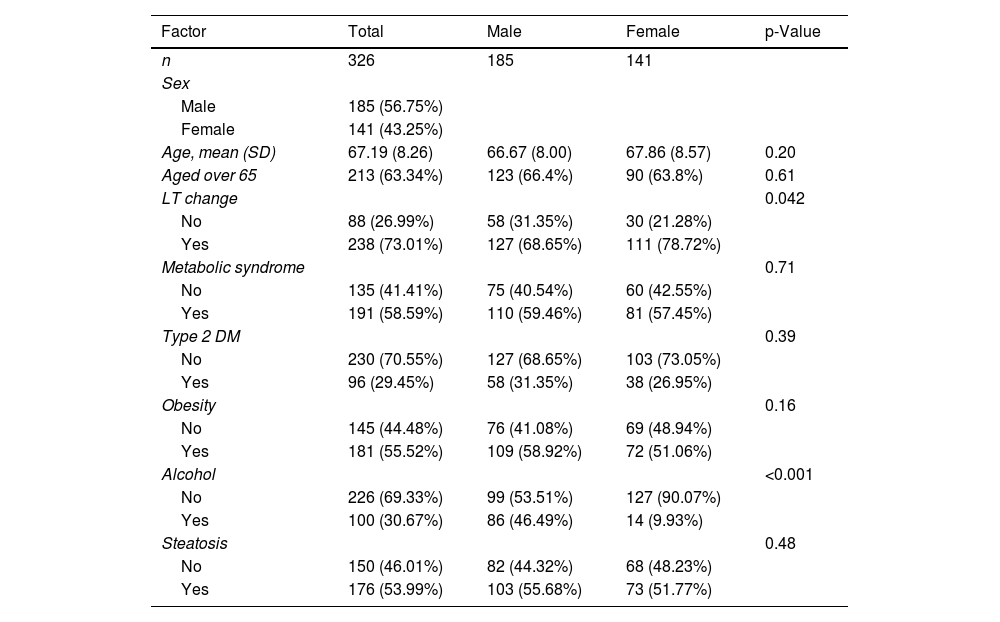
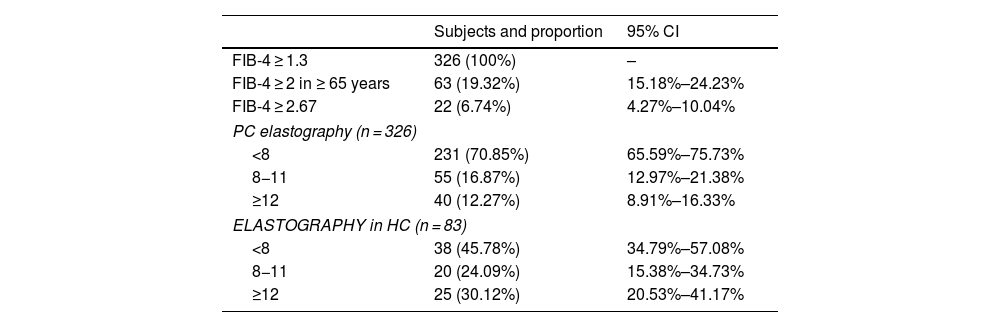
MethodsObservational, descriptive, cross-sectional study in ≥16 years of age with RF for chronic liver disease. Sex and age, RF (alteration of liver tests (LT), metabolic syndrome, diabetes, obesity, alcohol consumption, hepatic steatosis), and FIB-4, controlled attenuation parameter and TE in PC and in HC, were collected. According to a consensus algorithm, vibration-controlled TE was performed in PC in patients with FIB-4 ≥ 1,3, and those with measurement ≥ 8 kPa were referred to HC.
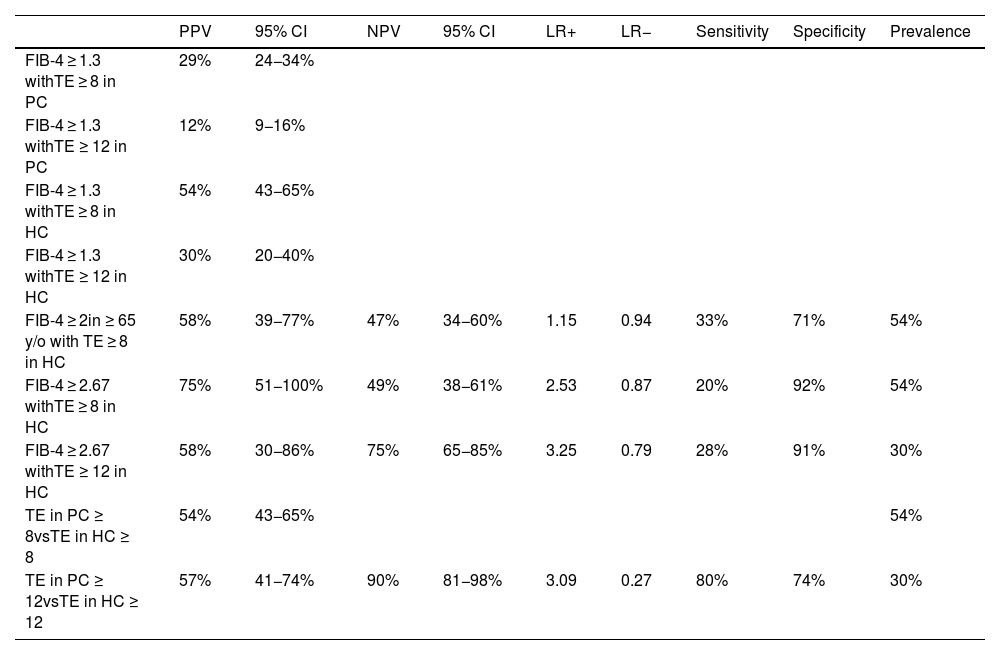
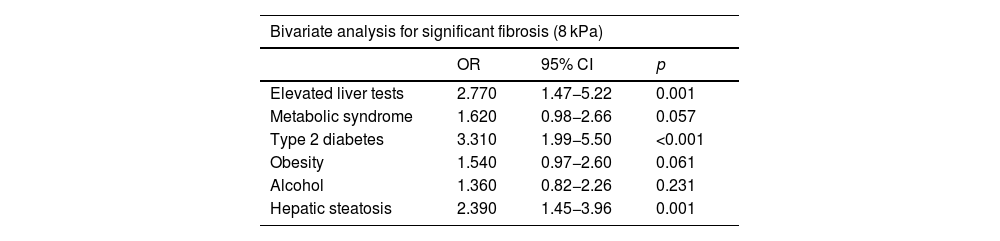
Results326 patients were studied. 71% were not referred to HC, due to liver stiffness<8 kPa. 83 of the 95 derivations did TE in HC. 45(54%) had TE ≥ 8, and 25(30%)≥12. The proportion of patients with stiffness≥8 kPa was 13,8%(45/326) and ≥12 kPa, 7,6%(25/326). The predictive values of the FIB-4 were low. The interobserver correlation coefficient between TE in PC and HC was 0,433. Variables associated with TE ≥ 8 in PC: LT alteration, diabetes and steatosis. With TE≥12: LT alteration, diabetes and obesity. Predictor variables: LT alteration and obesity.
ConclusionsThe study supports the sequential performance of serum indices and TE as a screening for fibrosis in the at-risk population in PC, which allows a reduction in the percentage of patients referred to AH, and a better stratification of risk patients.
Describir la proporción de pacientes con fibrosis hepática en poblaciones de riesgo en atención primaria (AP). Conocer la correlación entre el FIB-4 y la elastografía de transición (ET), correlación interobservador entre AP y atención hospitalaria (AH) en la ET, y factores de riesgo (FR) asociados.
MétodosEstudio observacional, descriptivo, transversal en ≥16 años con FR para hepatopatía crónica. Se recogieron sexo y edad, FR (alteración pruebas hepáticas (PH), síndrome metabólico, diabetes, obesidad, consumo alcohol, esteatosis hepática), y los valores del FIB-4, parámetro de atenuación controlada, ET en AP y en AH. Según algoritmo consensuado, se realizó ET de vibración controlada en AP a los pacientes con FIB-4 ≥ 1,3, derivándose a AH aquellos con medición≥8 kilopascales(kPa).
ResultadosSe estudiaron 326 pacientes. El 71% no se derivaron a AH, por rigidez hepática<8 kPa. 83 de los 95 derivados hicieron ET en AH. 45(54,2%) tenían ET ≥ 8, siendo en 25(30%)≥12. La proporción de pacientes con rigidez≥8 kPa fue del 13,8%(45/326) y ≥12 kPa, del 7,6%(25/326). Los valores predictivos del FIB-4 fueron bajos. El coeficiente de correlación interobservador entre la ET en AP y AH fue del 0,433. Variables asociadas con ET ≥ 8 en AP: alteración PH, diabetes y esteatosis. Con ET≥12: alteración PH, diabetes y obesidad. Variables predictoras en análisis multivariante: alteración PH y obesidad.
ConclusionesEl estudio apoya la realización secuencial de índices séricos y ET como cribado de fibrosis en población de riesgo en AP, que permite disminuir el porcentaje de pacientes que se derivan a AH, y una mejor estratificación de los pacientes de riesgo.
