





Colorectal cancer (CRC) is the second cause of cancer-related deaths worldwide. Five-year survival rate in Spain is 57%. The most important prognostic factor is the stage of the tumor at the diagnosis. CRC can be early diagnosed, but the adherence to screening programs is low (<50%). This study aims to ascertain the influence of social support and stressful life events on the adherence to the population screening of CRC with fecal occult blood test in Spanish average risk population.
MethodsMulticenter case–control study. We conducted a simple random sampling among individuals invited to participate in the colorectal cancer screening program. We analyzed epidemiological and social variables associated with lifestyle and behavioral factors. We performed a descriptive and a bivariant analyses and a logistic regression analysis.
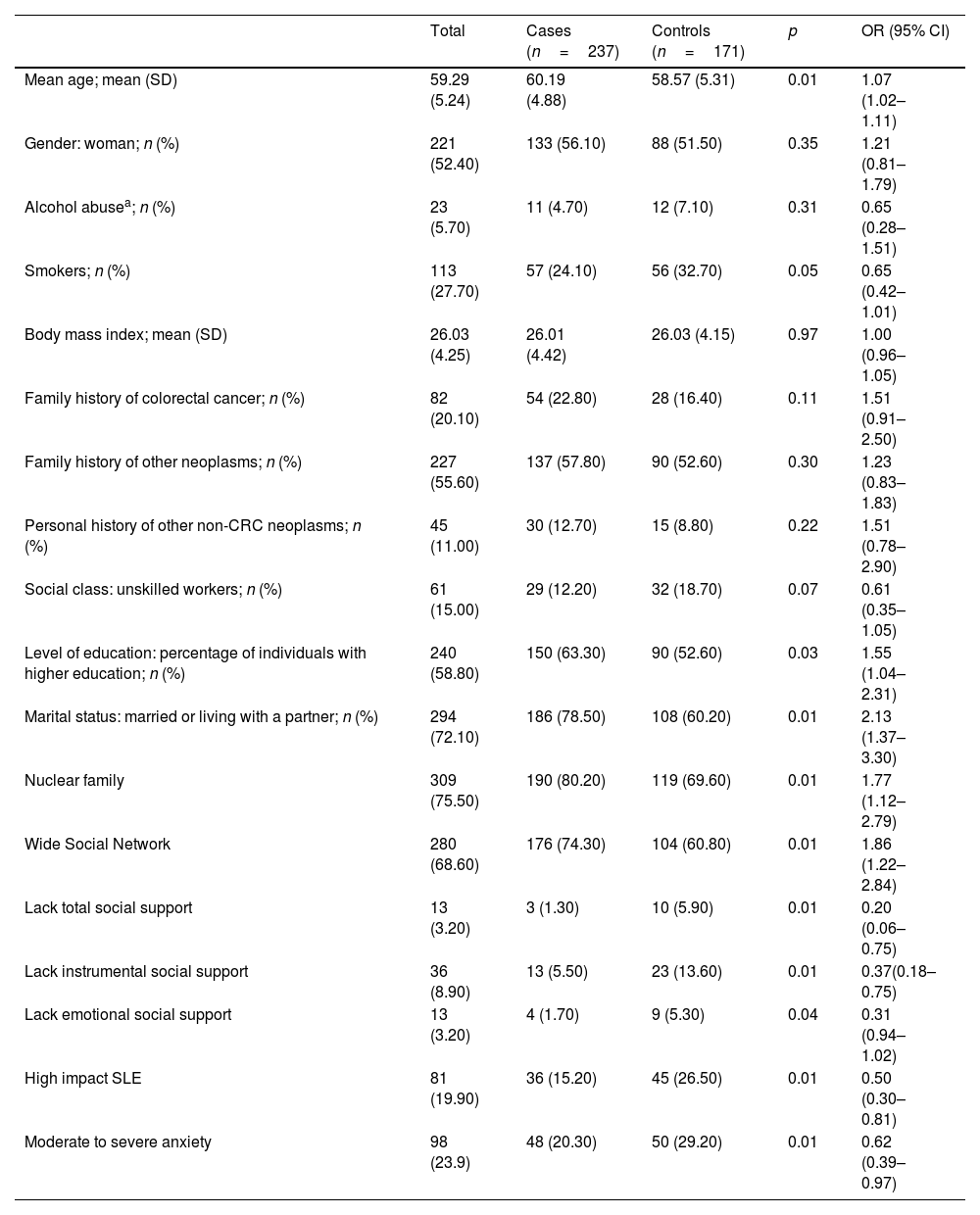
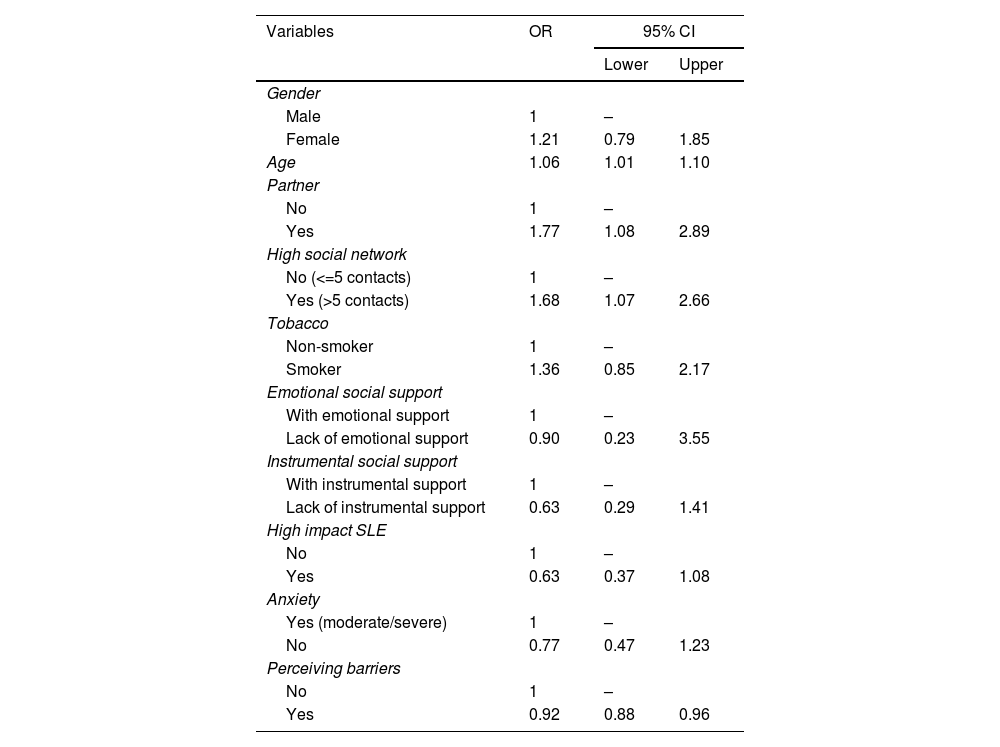
ResultsFour hundred and eight patients (237 cases and 171 controls) were included. Multivariant analyses showed independent association between higher adherence to the screening program and older age (OR: 1.06; 95% CI: 1.01–1.10), stable partner (OR: 1.77, 95% CI: 1.08–2.89) and wide social network (OR: 1.68; 95% CI: 1.07–2.66). Otherwise, lower adherence was associated to perceiving barriers to participate in the program (OR: 0.92; 95% CI: 0.88–0.96). We find a statistically significant association between lower adherence and high impact stressful life events in the bivariant analyses, and the tendency was maintained (OR: 0.63, 95% CI: 0.37–1.08) in the multivariant.
ConclusionSocial variables decisively influence the adherence to colorectal cancer screening. The implementation of social interventions that improve social support, reduce impact of stressful life events and the design of screening programs that decrease the perceived barriers, will contribute to increase the participation on these programs. Secondary, the colorectal cancer diagnosis will be made in early-stages with the consequent mortality reduction.
El cáncer colorrectal (CCR) es la segunda causa de muerte por cáncer en el mundo. La tasa de supervivencia a cinco años en España es de 57%. El factor pronóstico más importante es el estadio del tumor en el momento del diagnóstico. El CCR se puede diagnosticar precozmente, pero la adherencia a los programas de cribado es baja (< 50%). Este estudio pretende conocer la influencia del apoyo social y los acontecimientos vitales estresantes en la adherencia al cribado poblacional de CCR con sangre oculta en heces en población española de riesgo medio.
MétodosEstudio multicéntrico de casos y controles. Realizamos un muestreo aleatorio simple entre los individuos invitados a participar en un programa de cribado de CCR. Analizamos variables epidemiológicas y sociales asociadas al estilo de vida y factores conductuales. Realizamos un análisis descriptivo, un análisis bivariante y una regresión logística.
ResultadosSe incluyeron 408 pacientes (237 casos y 171 controles). El análisis multivariante demostró una asociación independiente entre una mayor adherencia al programa de cribado y mayor edad (OR: 1,06; IC 95%: 1,01-1,10), tener pareja estable (OR: 1,77, IC 95%: 1,08-2,89) y disponer de una amplia red social (OR: 1,68; IC 95%: 1,07-2,66). Por el contrario, la menor adherencia se asoció a la percepción de barreras para participar en el cribado (OR: 0,92; IC 95%: 0,88-0,96). Encontramos una asociación estadísticamente significativa entre menor adherencia y acontecimientos vitales estresantes de alto impacto en el análisis bivariante. La tendencia se mantuvo (OR: 0,63, IC 95%: 0,37-1,08) en el análisis multivariante.
ConclusiónLas variables sociales influyen decisivamente en la adherencia al cribado del CCR. La implementación de intervenciones sociales que mejoren el apoyo social y reduzcan el impacto de los acontecimientos vitales estresantes junto al diseño de programas que disminuyan las barreras percibidas, contribuirá a aumentar la participación en el cribado. Con ello, el diagnóstico de CCR en estadios precoces será mayor, con la consiguiente reducción en la mortalidad.

