



This study examined the Jordanian registered nurses’ perceptions of the obstacles and supportive behaviors of End-of-Life Care in Intensive Care Units and examined the differences in the concepts based on the samples’ demographics.
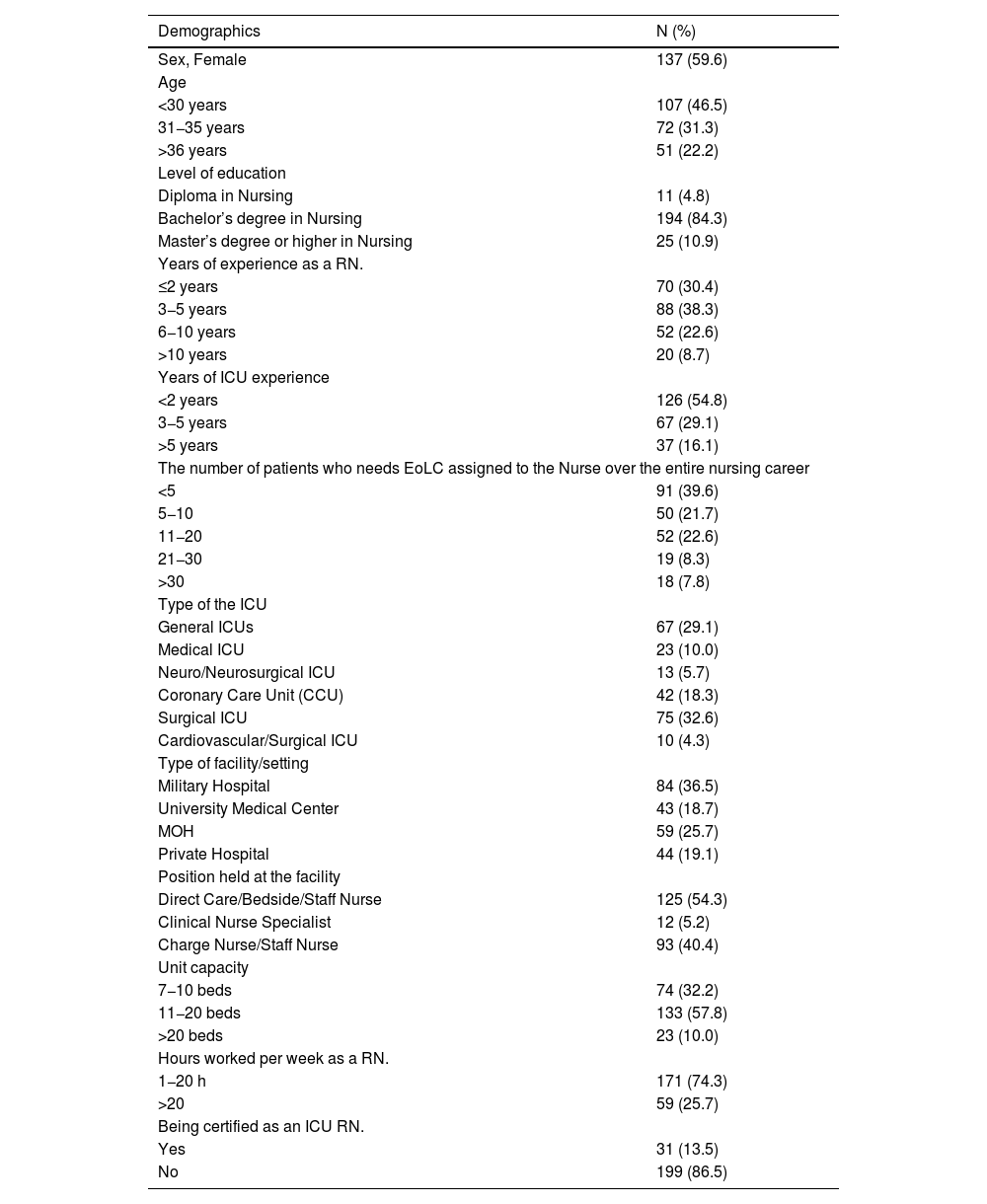
MethodsA cross-sectional and comparative study was conducted using a convenience sample of 230 Intensive Care Unit registered nurses in Jordan. Data were analyzed descriptively, and differences were measured using the independent sample t-test, the one-way Analysis of Variance, and Scheffe’s post hoc test.
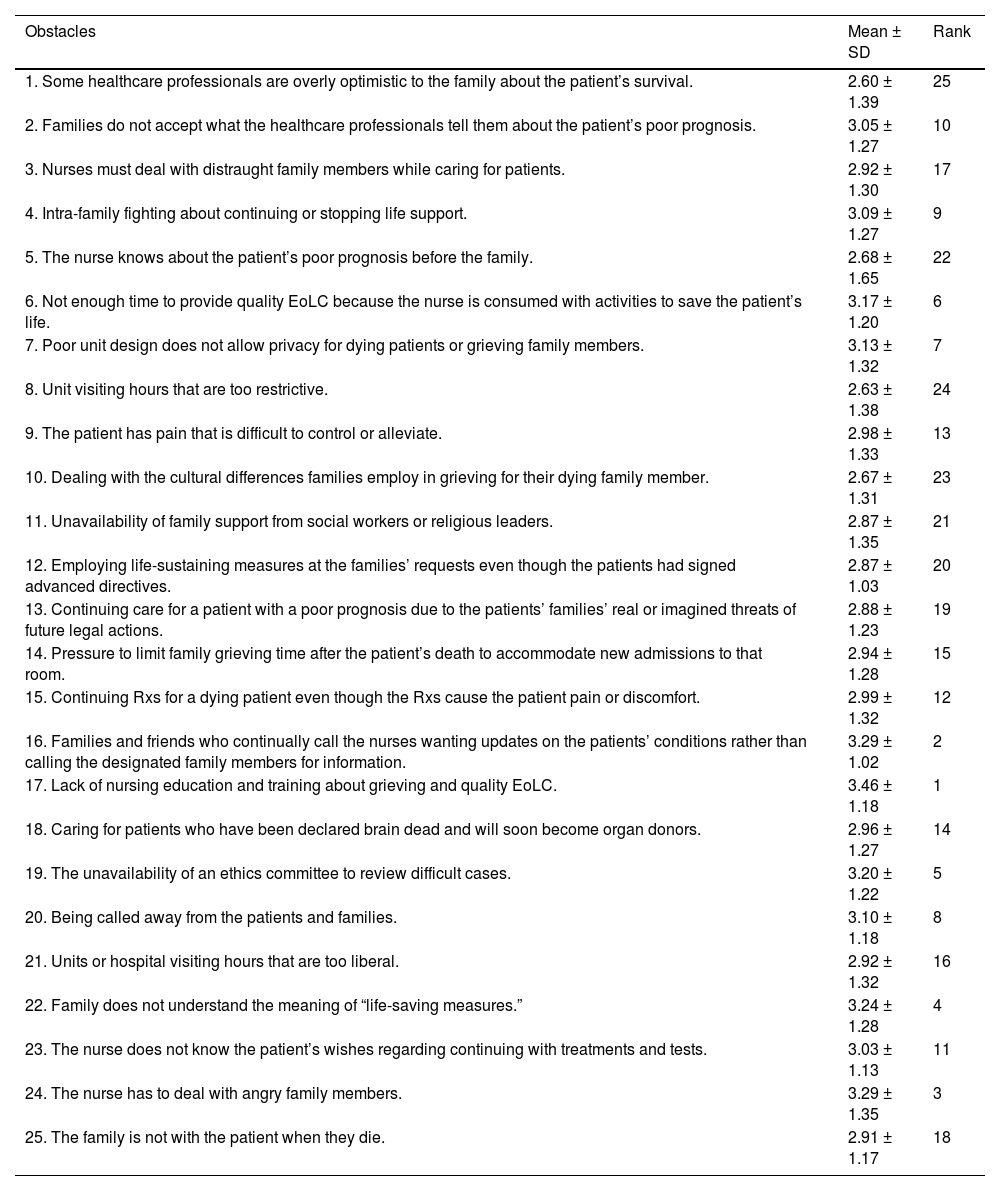
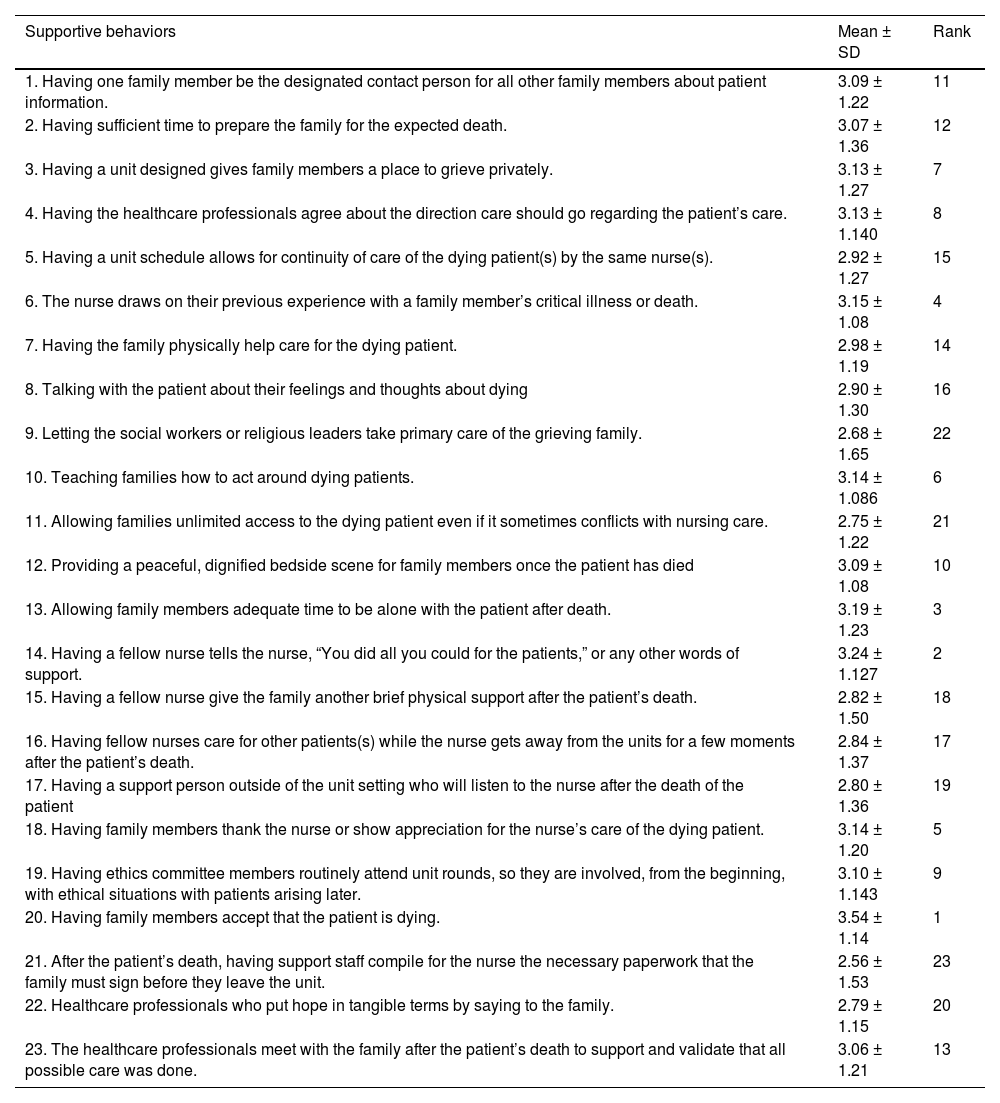
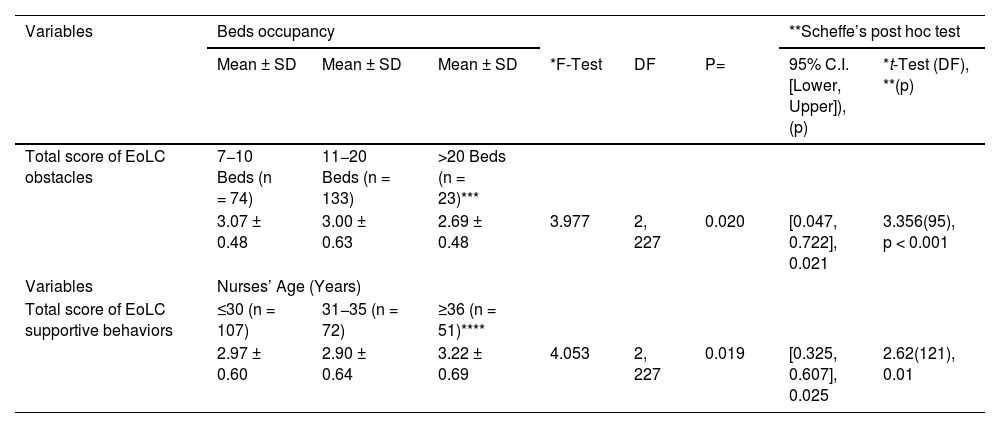
ResultsThe registered nurses’ scored moderately on obstacles (74.98 ± 14.54) and supportive behaviors (69.22 ± 4.84). The commonly perceived obstacle and supportive behaviors to End-of-Life Care in Intensive Care Units s were reported. The perceived obstacles differ based on the registered nurses’ certification as an Intensive Care Units nurse (3.04 ± 0.58 vs. 2.74 ± 0.49, p = 0.008), type of Intensive Care Unit (3.28 ± 0.34 vs. 2.86 ± 0.62, p < 0.001), type of facility (3.16 ± 0.59 vs. 2.77 ± 0.61, p < 0.001), number of beds in the unit (3.07 ± 0.48 vs. 2.69 ± 0.48, p = 0.020), and the number of hours worked per week (3.06 ± 0.56 vs. 2.81 ± 0.60, p = 0.005). In contrast, supportive behaviors only differ based on the registered nurses’ age (3.22 ± 0.69 vs. 2.90 ± 0.64, p = 0.019).
ConclusionsThe common End-of-Life Care perceived obstacle in Intensive Care Units was the lack of nursing education and training regarding the studies concept, which warrants immediate intervention such as on-job training. The common End-of-Life Care perceived supportive behavior in Intensive Care Units was when family members accepted that the patient was dying when nurses offered support to family members; motivational interventions are needed to sustain such behavior. Differences in the perceived obstacles and supportive behaviors should be leveraged for the benefit of patients, nurses, and hospitals.
Este estudio examinó las percepciones de las enfermeras registradas jordanas sobre los obstáculos y comportamientos de apoyo de la atención al final de la vida en las Unidades de Cuidados Intensivos y examinó las diferencias en los conceptos basados en la demografía de las muestras.
MétodosSe realizó un estudio transversal y comparativo utilizando una muestra de conveniencia de 230 enfermeras registradas en la Unidad de Cuidados Intensivos en Jordania. Los datos se analizaron descriptivamente y las diferencias se midieron mediante la prueba t de muestra independiente, el análisis unidireccional de varianza y la prueba post hoc de Scheffe.
ResultadosLas enfermeras registradas obtuvieron una puntuación moderada en obstáculos (74,98 ± 14,54) y comportamientos de apoyo (69,22 ± 4,84). Se informaron los obstáculos comúnmente percibidos y los comportamientos de apoyo a la atención al final de la vida en las Unidades de Cuidados Intensivos. Los obstáculos percibidos difieren según la certificación del enfermero registrado como enfermero de las Unidades de Terapia Intensiva (3,04 ± 0,58 vs. 2,74 ± 0,49, p < 0.001), tipo de Unidad de Cuidados Intensivos (3,28 ± 0,34 vs. 2,86 ± 0,62, p < 0.001), tipo de instalación (3,16 ± 0,59 vs. 2,77 ± 0,61, p < 0.001), número de camas en la unidad (3,07 ± 0,48 vs. 2,69 ± 0,48, p = 0,020), y número de horas trabajadas por semana (3,06 ± 0,56 vs. 2,81 ± 0,60, p = 0,005). En contraste, los comportamientos de apoyo solo difieren según la edad de las enfermeras registradas (3,22 ± 0,69 vs. 2,90 ± 0,64, p = 0,019).
ConclusionesEl obstáculo común percibido en la Atención al Final de la Vida en las Unidades de Terapia Intensiva fue la falta de educación y capacitación de enfermería sobre el concepto de estudios, lo que justifica una intervención inmediata, como la capacitación en el trabajo. El comportamiento de apoyo común percibido en la atención al final de la vida en las Unidades de Cuidados Intensivos fue cuando los miembros de la familia aceptaron que el paciente estaba muriendo cuando las enfermeras ofrecieron apoyo a los miembros de la familia; Se necesitan intervenciones motivacionales para mantener tal comportamiento. Las diferencias en los obstáculos percibidos y los comportamientos de apoyo deben aprovecharse para el beneficio de los pacientes, las enfermeras y los hospitales.
Artículo
Diríjase al área de socios de la web de la SEEIUC, (https://seeiuc.org/mi-cuenta/iniciar-sesion/) y autentifíquese.

