






The most prominent problem resulting from decreased body function in older adults is declining quality of life. Walking and talking among older adults in peer group may become a nursing therapy to improve their quality of life. The objective of this study was to identify the impact of walking and talking intervention of quality of life among community dwelling older adults in Depok, Indonesia.
MethodThis study applied quasi-experimental design with 43 and 40 older adults in the intervention and control group, respectively. The participants were selected using multistage random sampling method.
ResultsBased on t test, the average quality of life score of older adults improved more significantly in the intervention group than that in the control group, with p value of 0.003, its mean p value < α, respectively. An ANCOVA analysis was used to detect confounding factors. The result showed that all characteristics have a p value of > 0.05, which means there were no confounding factors warranting further investigation.
ConclusionsIt was concluded that walking and talking therapy in peer group significantly increase the quality of life of older adults.
The number of older adults in the world is projected to grow to 600 million in 2020. Of the entire world population, 11.8% are older adults. According to the Indonesian Central Bureau of Statistics in 20101, 19 million people, or 8.5% of the population were older adults. This phenomenon may arise various health problems. Aging decreases the physical functions and ability. While an older person's needs continue to increase, it may cause the older adults fail to fulfill their physical and physiological needs. Thus, depression and feelings social powerless are inevitable for them.
Older adults are considered as a risk group for depression and lose the quality of life due to several factors. First, there is biological factor. As older people, encounter the aging process. Second, there is social factor. The changes in an older person's social life require adaptation. Lastly, there is lifestyle factor. This includes changes in lifestyle related to physical activity and diet, which may pose new challenges2,3.
Quality of life is the interaction of human needs and the subjective perception to fulfill the needs and achieve wellness4,5. The question of quality of life is often associated with chronic disease, and it is 87.3% older adults suffer from a chronic illness in Indonesia6. Older adults who are more than 75 years old often experience a decrease in quality of life especially in the social domain.
Current efforts to optimize the lives of older people for optimize quality of life is still limited. Therefore, this study was conducted to identify walking and talking activities in peer group as nursing therapy's impact toward older adults’ quality of life. The combination of walking and talking as nursing interventions for the elderly is believed to improve the quality of life for older adults. The previous study revealed that walking regularly may improve physical and psychological activity while talking therapy improve social skill and environmental aspects7,8. Their research focused on training brain capacity to allow an older people to perform multiple activities at the same time. The participants were assisted with walking while simultaneously being evaluated; their ability to stay focused on a particular the discussion topic.
Walking and talking activities is part of Nursing Interventions Classification in activities and rest domain. This therapy aims to meet the physical needs of patients9. Walking therapy requires appropriate circumstances and sufficient support to meet the specific needs of the older people5. Previous study about walking and talking therapy was conducted a study to identify the effect of walking intervention on elderly patients within aged range 60-74 years old10. A primary result of this study was demonstrated the daily improvement in the of step number and time. After 12 times walking for 4 weeks then the ability of older people to fulfill the increasing need, evidenced an increase in the average score Katz index amount 5 points10. In addition, this study showed the improvement of the quality of life, mood and ability to in sport activities for the participants.
For older people quality of life is an indicator to achieve optimum well-being. The combination of walking and talking therapy can be carried out by the healthcare provider. The combination of these interventions helps older adults have better performance compared to those who do not receive the intervention. The older people following the walking and talking therapy had the physical health and adaptability to changing situations better. In order to optimize quality of life for the older adults a population whose number is increasing both in Indonesia and worldwide. The combination of walking and talking therapy should be implemented as a nursing intervention2.
Based on the aforementioned background information, this current study was conducted to identify the impact of walking and talking therapy as a nursing intervention on older people quality of life.
MethodA quasi-experiment design, including pre and posttest with a control group, was selected for this study. Therefore, randomization was not carried out to determine the intervention and control group.
Walking and talking activities in peer group is a nursing intervention package with two phases; walking and talking. The first phase is motion exercise. Participants were asked to walk slowly for 30 minutes with some interruptions. Then, the second phase was participation carried out through having 20 minutes conversation light topic predetermined by the researchers. This phase of intervention was delivered by nurses to the elderly group. At the first time for the intervention group after that the walking and talking therapy given the control group after both of group complete the assessment of the instrument quality of life for the older people.
The Walking and talking activities were carried out in a group. Overall number of participants is 83 older people, consists of 43 people for intervention group and 40 people for the control group. When carrying out the walking and talking therapy, the participants will divide in one small group. One group consisted of 6 to 10 participants. Following the model Based on the previous study, the exercise was conducted three times a week for four weeks, in the morning between 07 am until 10 am, and afternoon at 02 pm. until 04 pm. The primary activities began with physical training through walking. Talking therapy carried out afterwards within in group setting leads by the researchers.
Participants who did not attend the walking and talking therapy more than twice were eliminated. However, participants who did not attend the training session twice or less were given an extra session at the end of the intervention. Meanwhile, in the control group, the researchers would provide walking and talking activities, right after posttest for both groups were completed. In this study the exercise walking and talking therapy carry out 4 times for 4 weeks it means the all participants must finished all the 16 session.
The population in this study consisted of 93,314 older adults or the entire older adults living in Depok; this number based on Central bureau of statistics1. The number of sampling for this study was determined by using the formula of pairing two population hypothesis tests7. The outcome was 43 participants for the intervention group and 40 participants for the control group. Multistage random sampling was performed for this study.
Based on the result of sampling method, Kecamatan Sukmajaya in Depok was selected for conducting the study. This study for the intervention group took place in smaller part of Kecamatan Sukmajaya, namely Kelurahan Abadijaya and Kelurahan Cisalak, while the control group activities were conducted in Kelurahan Mekarjaya. Since expected sample number could not be reached in the first area alone (Kelurahan Abadijaya), the second area (Kelurahan Cisalak) was added.
This research study was approved by the Faculty of Nursing Universitas Indonesia Ethical Committee in March 2016. The design of this research study ensured there was no possibility of physical or mental harm to the participants. Personal information, such as names and dates of birth, were not included in the research tools. All data were managed using identification numbers.
To assess quality of life, This study used WHOQOL-Bref (world health organization quality of life) questionnaire which developed by World Health Organization (WHO)11. There were 26 questions within four major components; physical, psychological, social relationships and environment. The questionnaire was designed using a 1-5 likert scale.
Before conducting data analysis, the researchers carried out an editing process. This was carried done to ensure that the data obtained is complete. Researchers evaluated the retrieved data, including checking on the accuracy and completeness of answers in the assessment forms. Then, the data were managed by coding each variable to make the analysis and tabulation easier.
Univariate analysis was presented in the form of frequency and proportion of each variable, including mean and standard deviation. Since this research used interval parametric scale, two group mean differences test (paired t test) was carried out before and after the intervention. In order to identify the influence of walking and talking activities on the control and intervention groups, the researchers used an independent t-test. Multivariate analysis was conducted to assess the influence of confounding factors using the analysis of covariance (ANCOVA) test.
ResultsThe respondents’ characteristics will describe at the beginning to explain the research. The average age of the intervention group was higher than the average age of the control group. The average age of the intervention group was 68.47 years old, while the control group's average age was 68.83 years old (Table 1).
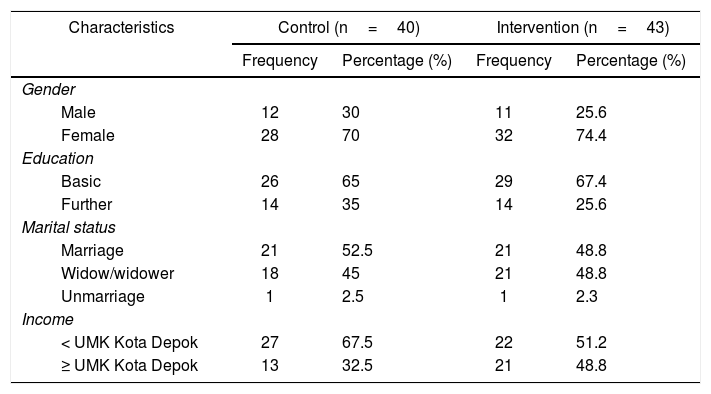
Regarding gender, proportion of females included in the study sample was larger than proportion of males, both in the intervention group (74.4% or 32 participants) and the control group (70% or 28 participants). Regarding education, the largest proportion of participants had a basic education level both in the control group and (65% or 26 participants) in the intervention group. Regarding the marital status, the largest proportion of participants in the control group were older adults with spouse (52.5% or 21 participants), while widows/widowers were the largest proportion in the intervention group (48.8% or 21 participants). Regarding total income, most participants in the control group received salary below the city's minimum wage (67.5% or 27 participants), while in the intervention group, there was same number of people who had salary below minimum wage as those who had a salary above the minimum wage (51.2% or 22 participants) (Table 2).
Distribution characteristics of respondents by gender, education level, marital status, income.
| Characteristics | Control (n=40) | Intervention (n=43) | ||
|---|---|---|---|---|
| Frequency | Percentage (%) | Frequency | Percentage (%) | |
| Gender | ||||
| Male | 12 | 30 | 11 | 25.6 |
| Female | 28 | 70 | 32 | 74.4 |
| Education | ||||
| Basic | 26 | 65 | 29 | 67.4 |
| Further | 14 | 35 | 14 | 25.6 |
| Marital status | ||||
| Marriage | 21 | 52.5 | 21 | 48.8 |
| Widow/widower | 18 | 45 | 21 | 48.8 |
| Unmarriage | 1 | 2.5 | 1 | 2.3 |
| Income | ||||
| < UMK Kota Depok | 27 | 67.5 | 22 | 51.2 |
| ≥ UMK Kota Depok | 13 | 32.5 | 21 | 48.8 |
The univariate test showed that the average quality of life before therapeutic intervention was higher in the control group than the intervention group which was 57.54 with a standard deviation of 12.54. Following the intervention, the quality of life for the intervention group was higher than it was for the control group reaching 71.86 with a standard deviation of 7.86.
The mean difference in the intervention group for the average quality of life score before and after the therapeutic was 15.12. A further paired t test experiment showed p value of 0.000. It can be concluded that there was difference between the average quality of life value before and after walking and talking therapy. The mean difference of the control group was by 6.83, while further paired t-test showed a p-value of 0.054. From this, it can be concluded that there was no mean difference between the pre- and post-measurement in the control group (Table 3).
Based on Table 4, walking and talking therapy activities were significant impacts on the older adults’ quality of life with p-value of 0.003.
The multivariate test result using the ANCOVA test towards the confounding factors of age, gender, level of education, income and marital status, shows that all of older people characteristics did not affect the impact of walking and talking intervention on quality of life for older adults, as which every characteristic had a p-value of > 0.05.
DiscussionThe average age of this study sample was 68.83 for the intervention group and 68.35 for the control group. WHO stated that an older adult is someone older than 60 years old12. According to the Central Bureau of statistic, 84.96% older adults in Depok have age range from 60 to 74 years old.
Female older adults made up the largest proportion of the participants with 58 participants (72.5%). This study corresponded to a previous study13 which revealed that older people female show a higher level of participation in physical activities than older people males. Thus situation was also supported by the fact that a female life expectancy is higher than a male life expectancy. In addition, females tend to have better social interaction than males.
Most participants in this study had a basic level of education with 53 participants or 66.25% of the total sample. This corresponds to Trihandini's study in 2010 which also found that the majority of the elderly population had basic level of educations, such as elementary school and junior high school. As a result higher level of effort is required when trying to deliver information to this population, such as in and preventive activities13.
The proportion of older adults with spouse in our sample was approximately 40 participants (50%). This corresponded Desiningrum's study which discovered that the number of older adults with spouse was higher than the number of older adults without spouse or whose spouse has passed away6,14. A spouse is the closest kind of social support a person may have. Additionally, a spouse plays an important role in older adult's life which is supported by their health status. Older adult with spouses demonstrated higher levels of participation in walking and talking therapy.
The highest proportion of participants in this study based on income was older adult with income lower than Depok minimum wage which is IDR3.046.180 (Kompas, 2016).Their incomes mostly came from pension funds and temporary jobs. Economic level undeniably affects a people health status. It corresponded to previous study15 which indicated that older adult receive lower income compared to non-elderly adults. This result is also associated with the productivity levels at work.
Impact of walking and talking therapy activities on quality of life for older adultsThese results demonstrate differences in the average score of quality of life scores for in the intervention group before and after walking and talking activities in peer group. The average score improved from 56.76 to 71.88 (an average difference 15.12), with p-value of 0.003. With the control group, there was also an improvement in the average score of the quality of life from 57.4 to 12.52 (an average difference of 6.83) although the p-value was 0.054. Based on this result, it was can be concluded that there was no difference between in the first and second measurement for the control group.
The aforementioned results corresponded with Hewitt et al study16 which implied that physical exercise which was practiced with 300 older adults for six months in Australia, showed significant impacts on quality of life of older adults in nursing home. In the current study, it was revealed that longer physical exercise, such as walking and balance exercise improved the quality of life for those whose quality of life declined due to aging. According to Yenny and Herwana17, in Indonesia older adult experience a decrease in quality of life after reaching the age of 75. De Souza Santos et al18 stated that physical exercise such as walking which was undertook by 323 female elderly with an average age of 69 years old improved their quality of life by 9.19% (p=0.0001). Based on results from current study and previous study evident that physical exercise, like walking together in a scheduled regularly, can improve the quality of life of elderly consist of physical, psychological, social and environmental support. Walking therapy give the elderly to the ability to increase strength and improved physical function of the body, and helps the elderly has the adaptability to changes in their environment.
The next discussion in the current study impact the walking and talking therapy on improve the ability physical older people. Previous study Hayasaka19 conducted a study to identify the physical exercise using muscle training, stretching exercise, and walking for eight weeks, which resulted in reducing pain and improving quality of life. The quality of life measurement included happiness, loneliness, life satisfaction and depression. The researchers in this study were assisted by a physiotherapist. There were 200 older adults in the intervention group and 171 older adults in the control group, with an average age of 82.02. The result showed a significant difference in the pain scale for the intervention group with a p-value < 0.05. In addition, there was a significant result quality of life with a p-value, 0.023. Walking and talking therapy in the current study evident that this therapy can help older people have distraction for their symptom chronic illness, and then older people can improve their independency for activity daily living. The final goal the older people can fulfillment needs.
Research on the domains of in the WHOQOL-BREF questionnaire was carried out previous study in San Paolo and Sao Jose dos Campos, Brazil, using 120 older adults as participants. Based on the WHOQOL-BREF questionnaire, the average score for the physical domain was 62.11, for the psychological domain 66.22, the social domain 72.15, and environmental domain 66.30. We can compare this to the older adults in our study in Depok, Indonesia. The average value for the physical domain was 62.27, for the psychological domain 68.75, the social domain 61.88 and the environmental domain 66.17. This result revealed that quality of life older adults in Depok was better than for those in Brazil in physical, psychological, and environmental domains while the social domain is better Brazil. These differences result from differences in the characteristics of the elderly and the availability of better services in Brazil compared to Indonesia3,4.
Regularly scheduled physical exercise allows older adults to compensate for their decreasing body function, being especially beneficial to their musculoskeletal system. Active physical exercise encourages the body to improve muscle strength, helps prevent larger muscle mass lost, and improves nutrients absorption.
Impact of walking and talking therapy in quality of life of older adults after considering the confounding factorsAfter analyzing the confounding factors, it was can concluded that none of these characteristics were confounding factors. Walking and talking therapy had a direct impact on the quality of life of older adults. Regular walking and talking therapy creates a pattern or new habit for the elderly5,20. During this therapy, the body slowly repairs functional coordination as well as neuromuscular system, which improves body function as a whole. Furthermore, the happiness-induced hormone endorphin is released during walking and talking therapy which improve the quality of life. Walking and talking therapy impacts physical, psychological, social support, and environment components.
The author thanks all the staff of Puskesmas Sukmajaya and Abadijaya, and also the participants for their dedicated support and involvement. We would also like to extend our gratitude. The research was funded by PITTA Grant Directorate of Research and Community Services Universitas Indonesia for 2016 fiscal year.
