






This study seeks to assess the influence of type 2 diabetes mellitus (T2DM) and its complications on the deterioration of muscle mass and function in patients with disease-related malnutrition (DRM).
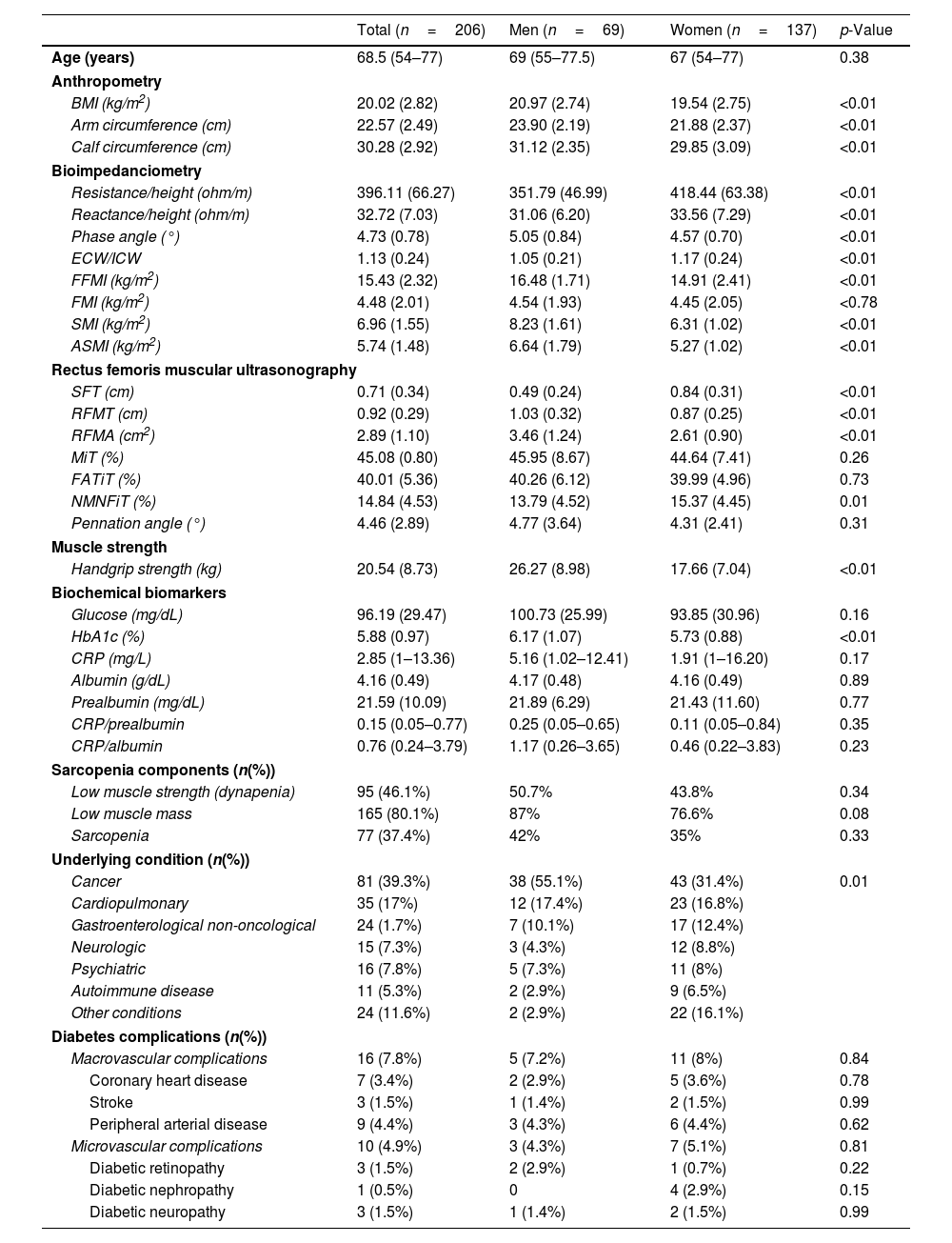
MethodsWe conducted a descriptive cross-sectional study in a sample of 206 patients (57.6% women) with DRM. Patients were compared based on the presence or absence of diabetes mellitus (DM). Differences were also observed based on the duration of DM and the presence of complications. Age, gender, body mass index (BMI), bioimpedanciometry (BIA) parameters, ultrasonography parameters and the diagnosis of dynapenia or sarcopenia were recorded.
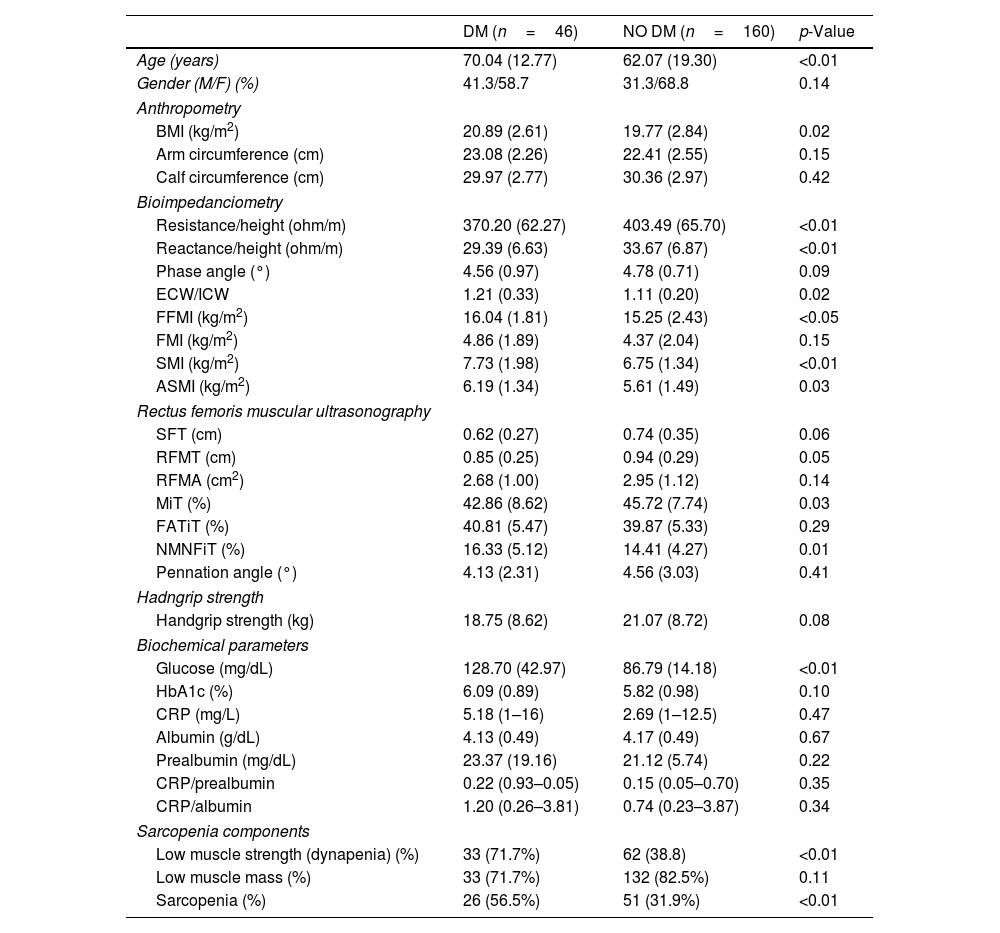
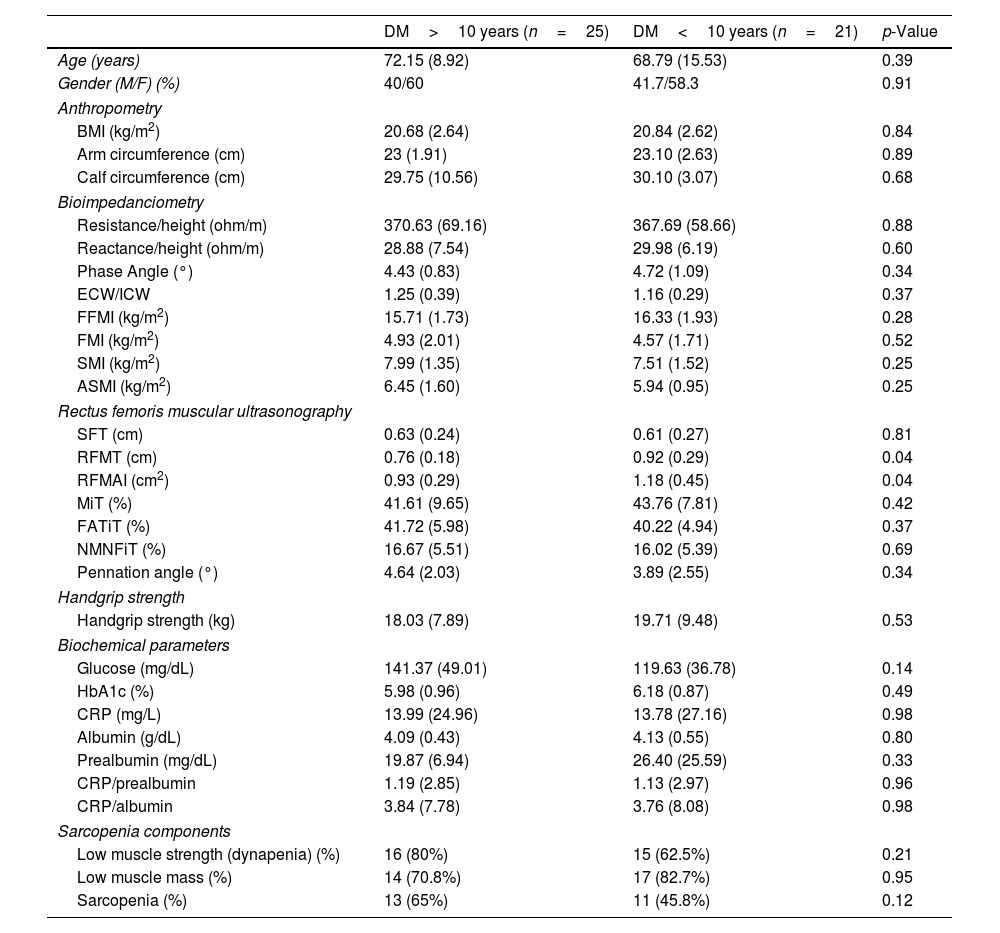
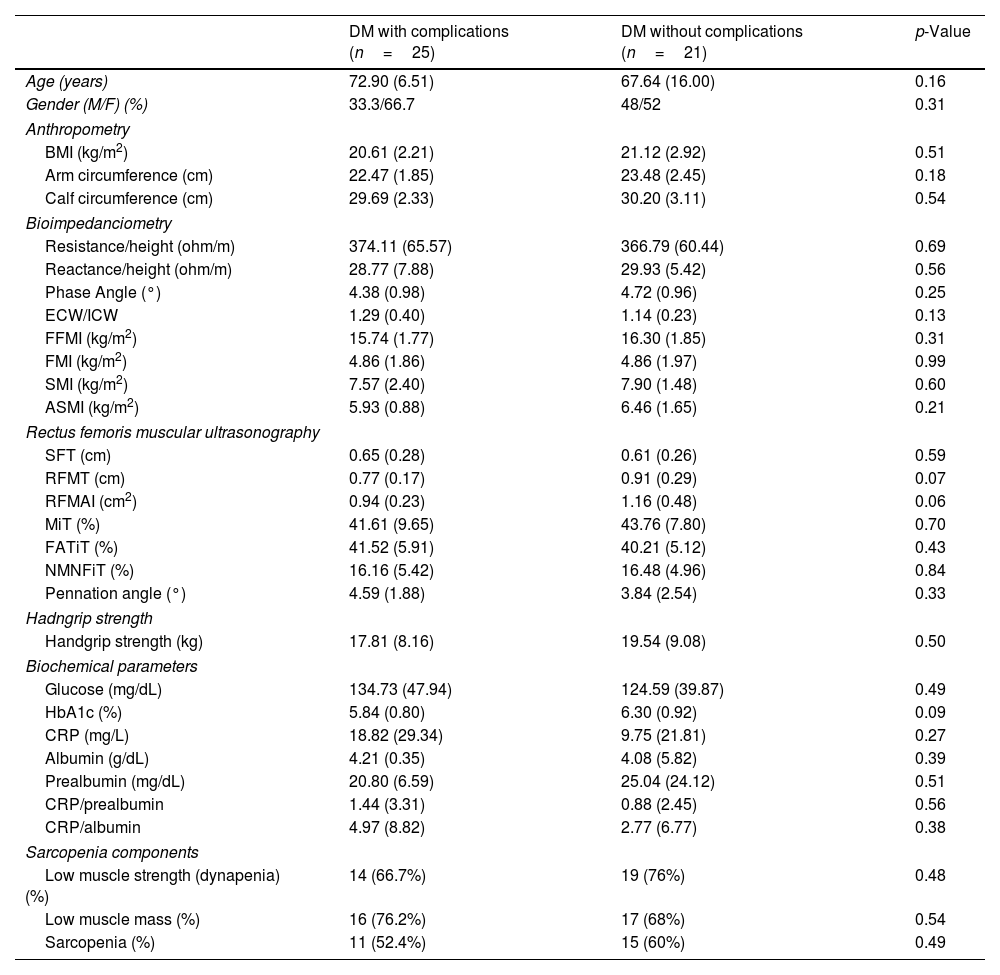
ResultsA total of 46 (22.33%) patients had DM, which was associated with higher values of skeletal muscle index (SMI) (DM, 7.73 (1.98)kg/m2 vs NoDM, 6.75 (1.34)kg/m2, p<0.01) in BIA analysis. Furthermore, it was associated with lower values of rectus femoris muscle thickness (RFMT) (DM, 0.85 (0.25) vs NoDM, 0.94 (0.29), p<0.05). Long-standing DM was associated with lower values of SMI (DM>10 years: 7.25 (1.46)kg/m2 vs DM<10 years: 8.18 (2.30)kg/m2, p<0.01) and with complicated DM (complicated DM, 7.57 (2.40)kg/m2 vs non-complicated DM, 7.90 (1.48)kg/m2, p<0.01). Moreover, these conditions were associated with lower values of RFMT (DM>10 years: 0.76 (0.18)cm vs DM<10 years: 0.93 (0.29) cm, p<0.05; Complicated DM, 0.77 (0.17) cm vs Non-complicated DM, 0.94 (0.29)cm, p<0.05). DM was a risk factor for the development for dynapenia (OR, 3.56, 95%CI, 1.52–8.29, p<0.01) and sarcopenia (OR, 3.08, 95%CI, 1.35–7.02, p<0.05) adjusted for age, gender, BMI and inflammatory status (determined by CRP). The presence of diabetic complications was a risk factor for dynapenia (OR, 2.08, 95%CI, 1.18–3.66; p=0.01) and sarcopenia (OR, 1.92, 95%CI, 1.12–3.28; p=0.02), after adjusting for gender, age, oncologic condition, BMI and CRP levels.
ConclusionsIn patients with DRM, poorly controlled T2DM was associated with worse muscle quantity and quality in muscle ultrasound. Long-standing DM and complicated DM were risk factors of dynapenia and sarcopenia. For clinical practice, multidisciplinary management to prevent these events is essential.
Este estudio tiene como objetivo evaluar la influencia de la diabetes mellitus tipo 2 (DM2) y sus complicaciones en el deterioro de la masa y función muscular en los pacientes con desnutrición relacionada con la enfermedad (DRE).
MétodosSe realizó un estudio descriptivo transversal en una muestra de 206 pacientes (57,6% mujeres) con DRE. Los pacientes se compararon según la presencia o ausencia de diabetes mellitus (DM), y se observaron diferencias en función de la duración de la DM y la presencia de complicaciones. Se registraron la edad, el género, el índice de masa corporal (IMC), los parámetros de bioimpedanciometría (BIA), los parámetros de ecografía y el diagnóstico de baja fuerza muscular o sarcopenia.
ResultadosCuarenta y seis (22,33%) pacientes presentaban DM, que se asoció con valores superiores del índice de masa muscular esquelética (IMME) (DM: 7,73 [1,98] kg/m2 vs. sin DM: 6,75 [1,34] kg/m2; p<0,01) en el análisis de BIA. Además, se asoció con valores inferiores del grosor del músculo recto femoral (GMRF) (DM: 0,85 [0,25] vs. sin DM: 0,94 [0,29]; p<0,05). La DM de larga duración se vinculó a valores inferiores de IMME (DM>10 años: 7,25 [1,46] kg/m2 vs. DM<10 años: 8,18 [2,30] kg/m2; p<0,01), así como con DM complicada (DM complicada: 7,57 [2,40] kg/m2 vs. DM no complicada: 7,90 [1,48] kg/m2; p<0,01). Además, estas condiciones se relacionaron con valores inferiores de GMRF (DM>10 años: 0,76 [0,18] cm vs. DM<10 años: 0,93 [0,29] cm; p<0,05). La DM se asoció con un mayor riesgo de dinapenia (OR: 3,56, IC 95%: 1,52-8,29; p<0,01) y de sarcopenia (OR: 3,08, IC 95%: 1,35-7,02; p<0,05), tras el ajuste por género, edad, IMC y estado inflamatorio (determinado por PCR). La presencia de complicaciones de la diabetes fue factor de riesgo de dinapenia (OR: 2,08, IC 95%: 1,18-3,66; p=0,01) y sarcopenia (OR: 1,92, IC 95%: 1,12-3,28; p=0,02), tras el ajuste por edad, género, enfermedad oncológica, IMC y estado inflamatorio.
ConclusionesEn los pacientes con DRE, la DM2 mal controlada se asoció con una peor cantidad y calidad muscular, en la ecografía muscular. La DM de larga duración y la DM con complicaciones crónicas resultaron ser factores de riesgo para la dinapenia y la sarcopenia. Para la práctica clínica, es esencial un manejo multidisciplinar que prevenga estos eventos.
