







Atypical endometriosis is considered a precursor lesion to cancer associated with endometriosis. Two types of atypical endometriosis have been proposed: an architectural type with a higher risk of malignancy and a cytological type with a lower potential for malignancy.
Main symptoms and/or clinical findingsA 37-year-old Caucasian woman presented with umbilical bleeding coinciding with menstruation. On physical examination, two small, bluish lesions were observed in the umbilical scar.
Primary diagnosisThis clinical case is of interest because it describes a lesion of atypical architectural endometriosis located in the navel.
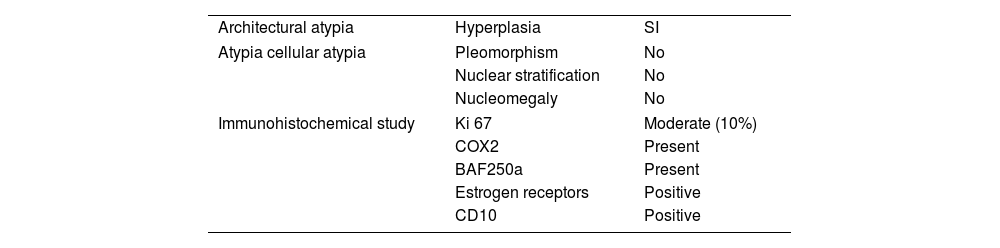
Therapeutic interventions and resultsThe microscopic and immunohistochemical characteristics of the lesion were examined. The presence of nuclear stratification, hyperchromatism, and pleomorphism were observed as microscopic qualities. In terms of the immunohistochemical panel, the degree of cell proliferation was analyzed using Ki 67, BAF250a was used as the surrogate marker of ARID 1A, inflammation was assessed through COX, and estrogen and progesterone receptors were examined. The results showed increased cellular activity, the presence of inflammation, and no mutation of the ARID1a gene, with moderate cell proliferation.
ConclusionUmbilical endometriosis is rare, and while malignancy is infrequent, it is possible. For this reason, a complete anatomopathological study including an immunohistochemical panel should be performed to diagnose atypical endometriosis.
La endometriosis atípica está considerada como una lesión precursora de cáncer asociado a endometriosis. Se han propuesto 2 tipos de endometriosis atípica, una arquitectural con mayor riesgo de malignización y otra citológica cuyo potencial de malignización es menor.
Principales síntomas y/o hallazgos clínicosUna mujer de 37 años caucásica consulta por sangrado catamenial umbilical. A la exploración física se observan 2 pequeñas lesiones umbilicales azuladas.
Diagnóstico principalEste caso clínico es interesante porque se describe una lesión de endometriosis atípica arquitectural localizada en el ombligo.
Intervenciones terapéuticas y resultadosSe ha descrito sus características microscópicas e inmunohistoquímicas para caracterizarla. La presencia de estratificación nuclear, hipercromatismo y pleomorfismo como cualidades microscópicas y en cuanto al panel inmunohistoquímico se ha analizado el grado de proliferación celular mediante el Ki-67, BAF250a como el marcador subrogado del ARID1A, el grado de inflamación mediante COX y los receptores estrogénicos y gestagénicos. Los resultados demuestran que tiene una actividad celular aumentada, presencia de inflamación y no mutación del gen ARID1A con moderación proliferación celular.
ConclusiónLa endometriosis umbilical es poco frecuente y su malignización, aunque rara es posible. Por esta razón, se debería realizar un estudio anatomopatológico completo que incluya un panel inmunohistoquímico en aras de diagnosticar endometriosis atípica.
