










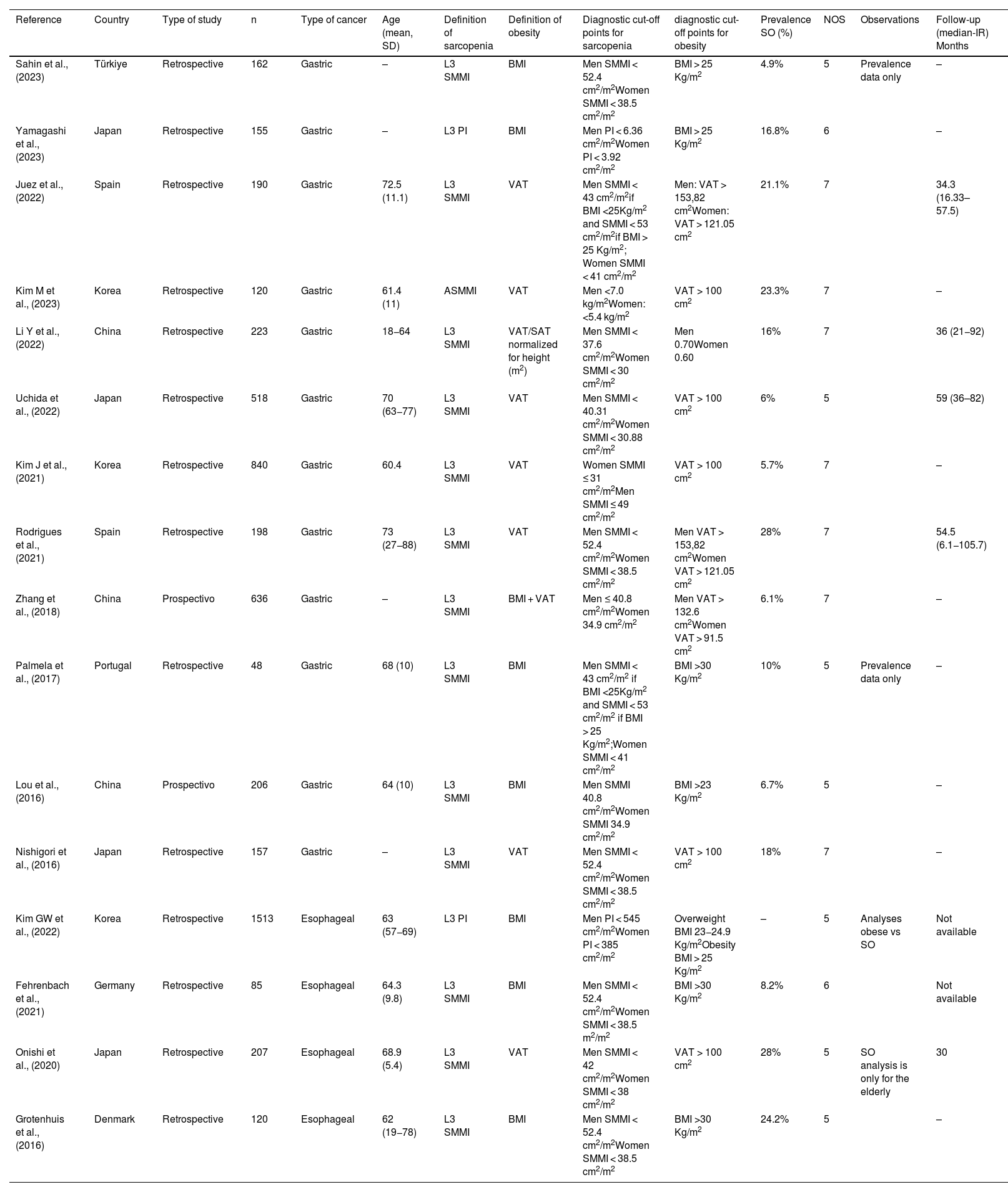
Sarcopenic obesity (SO) is a new entity whose definition encompasses the diagnosis of overweight in malnourished patients. The aim of the review was to assess the impact of body composition in patients with esophago-gastric tumors (EGT) on perioperative and oncological outcomes. This systematic review was conducted under the PRISMA guidelines. MEDLINE (PubMed), Embase, Web of Science and SCOPUS databases were searched until January 2024. Sixteen articles were identified for analysis analyzing 5,378 patients. The prevalence of SO was 10% (95%CI: 6–16; I2 = 94%). Preoperative diagnosis of SO was associated with a twofold increased risk of severe postoperative complications (OR 2.32 [95%CI 1.41–3.82] I2 = 70%). Meta-analysis of overall survival outcomes identified that SO was associated with worse overall survival (HR 2.30; 95%CI 1.46–3.61).
La obesidad sarcopénica (OS) es una nueva entidad que engloba su definición el diagnóstico de sobrepeso en pacientes desnutridos. El objetivo de la revisión fue evaluar el impacto de la composición corporal en pacientes con tumores esofago-gástricos (TEG) en los resultados perioperatorios y oncológicos. Esta revisión sistemática se ha realizado bajo las directrices PRISMA. Se realizaron búsquedas en las bases de datos MEDLINE (PubMed), Embase, Web of Science y SCOPUS hasta enero de 2024. Se identificaron 16 artículos para el análisis que analizaron 5.378 pacientes. La prevalencia de OS fue del 10% (IC95%: 6–16; I2 = 94%). El diagnóstico preoperatorio de SO se asoció con el riesgo doble de complicaciones postoperatorias graves (OR 2,32 [IC95%: 1,41−3,82] I2 = 70%). El metanálisis de los resultados de supervivencia global identificó que la OS se asociaba a una peor supervivencia global (HR 2,30; IC95%: 1,46−3,61).


