




Debido a la escasez de estudios comparativos acerca del tratamiento adyuvante en esta dolencia, presentamos una revisión sistemática actualizada, analizando las distintas alternativas de terapias adyuvantes. Esta revisión está basada en la guía PRISMA.
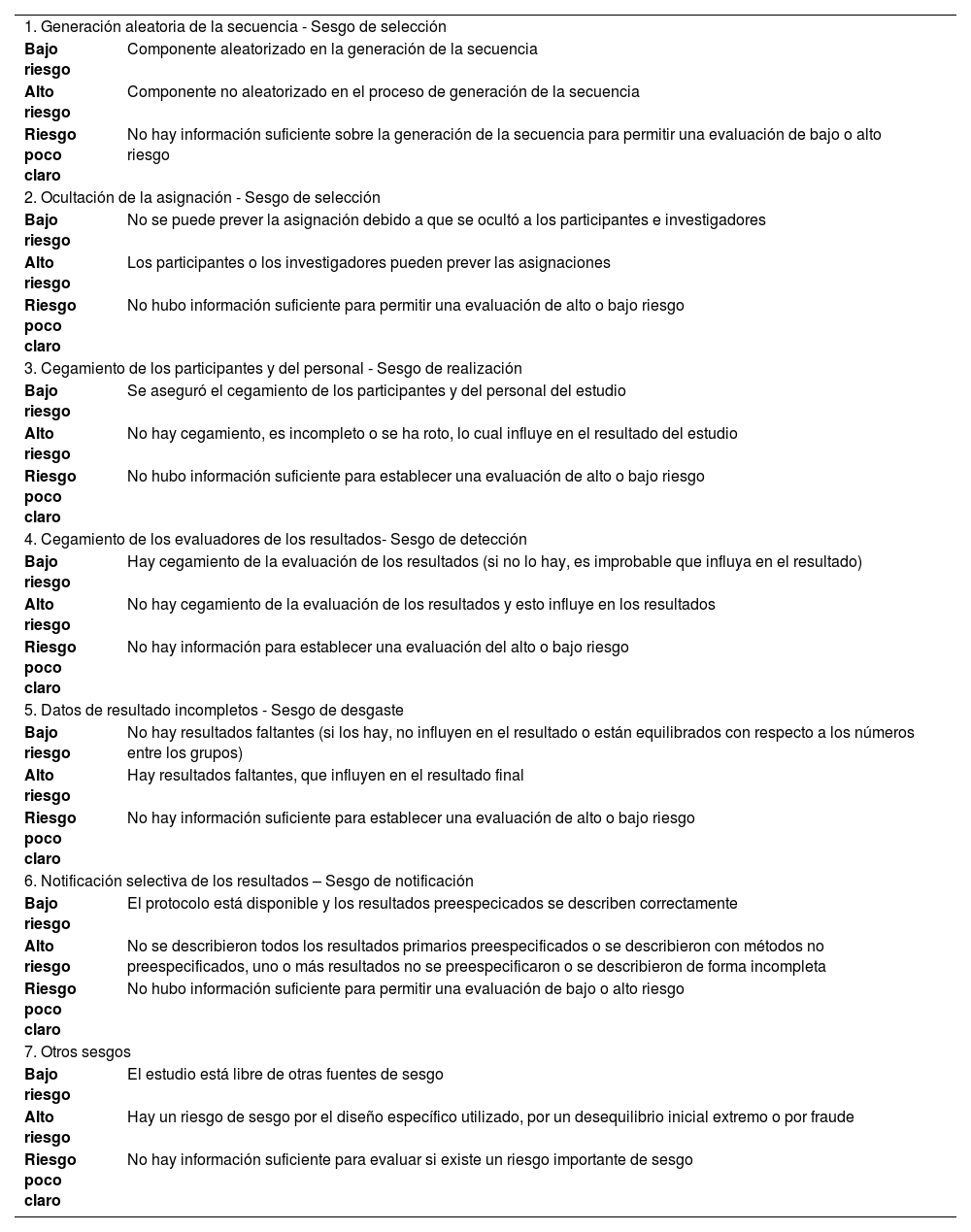
Material y métodosSe ha realizado una revisión sistemática de 13 ensayos clínicos siguiendo los criterios de inclusión preespecificados. Se han evaluado los posibles sesgos y la certeza de la evidencia. Finalmente, se han extraído los datos necesarios para presentar los resultados de los estudios.
Resultados y discusiónLa presente revisión sistemática establece que el pembrolizumab puede utilizarse como tratamiento adyuvante en pacientes con cáncer renal avanzado con mayor riesgo tras la nefrectomía, ya que el estudio KEYNOTE-564 concluyó que aumentaba la supervivencia libre de enfermedad (SLE) y la supervivencia global. Es discutido el uso de sunitinib, ya que el estudio publicado en NEJM muestra un beneficio modesto en cuanto a SLE, pero solo en una revisión central independiente y ciega. Pazopanib no obtiene beneficio de forma global según el estudio PROTECT. El estudio EVEREST no mostró beneficio significativo en cuanto al uso de everolimus. Se necesitan más estudios que confirmen el uso de axitinib, debido a que el ensayo ATLAS mostró resultados estadísticamente significativos en la SLE en población de mayor riesgo, según una evaluación por el investigador, pero no según una revisión central independiente. La terapia con 5-FU, α-IFN e IL-2, atezolizumab, sorafenib, talidomida, nivolumab+ipilimumab no debe utilizarse como tratamiento adyuvante.
Given the lack of comparative studies on adjuvant treatment for clear cell renal cell carcinoma, we present an updated systematic review, exploring the various options for adjuvant therapy. This review is conducted in accordance with the PRISMA guidelines.
Material and methodA systematic review was conducted, and 13 clinical trials were included after applying the pre-specified inclusion criteria. The risk of bias and the level of evidence were assessed. Subsequently, the requisite data were extracted in order to present the findings of the studies.
Results and discussionThe present systematic review establishes that pembrolizumab can be used as adjuvant therapy in patients with advanced renal cancer at high risk after nephrectomy. This is supported by the KEYNOTE-564 study, which concluded that it increased disease-free survival (DFS) and overall survival. The use of sunitinib is discussed, since the study published in NEJM shows a modest benefit in terms of DFS, but only in an independent and blinded central review. According to the PROTECT study, pazopanib has no overall benefit. The EVEREST study showed no significant benefit over everolimus. Further studies are needed to confirm the use of axitinib, as the ATLAS trial showed statistically significant results in DFS in higher-risk population based on investigator assessment, but not based on independent central review. Therapy with 5-FU, α-IFN and IL-2, atezolizumab, sorafenib, thalidomide, nivolumab+ipilimumab should not be used in the adjuvant setting.