



To analyze the differences and similarities of the concepts of comfort, well-being and quality of life (QoL).
MethodsReview of concept analysis research on PubMed, Cinahl (full text) and Scielo, using the search terms “Comfort”, “Well-being”, “Quality of Life” and “Concept Analysis”.
ResultsEighteen studies were included. Comfort is a broader holistic concept while well-being is mainly related to psycho-spiritual dimensions. QoL reflects the individual perception of satisfaction with life.
ConclusionsThe concepts are not surrogate terms, but related concepts sharing common attributes. Caution should be taken in further research, particularly as regards the correct use and framing of the concepts.
Quality of life (QoL), comfort and well-being have progressively been used as important goals in many contexts such as health, justice, economy or environment.1 Particularly in nursing, several research papers on these concepts have established the grounds for the development of theories and inclusion in the classifications and taxonomies.2–6 The distinction of the concepts is not always clear, as the terms are semantically close and this may result in the interchangeable use of the concept of well-being and the concept of comfort, for example. Several concept analysis studies have identified well-being as synonymous with the concept of comfort, and QoL as a related concept.5,7 Some inconsistencies have been identified in nursing knowledge classifications that may lead to the promotion of redundancies and gaps, with repercussions on clinical practice. The objective of this study is to analyze the differences and similarities of the concepts of comfort, well-being and QoL, based on a review of concept analysis research.
BackgroundThe concepts of comfort, well-being and QoL have been gaining particular relevance in the health context because of the scientific development and technological changes in the illness journey, and also because of concerns with the defense of human rights, particularly after the Second World War. In general, people live longer but not necessarily better, which has led several authors and disciplines to study the concepts of comfort,3,6,8 well-being,4 and QoL.9,10 Although several theories have been developed that specifically concern each concept, the lack of clarity regarding the use and appropriateness of the concepts sometimes exists.
The first inconsistencies can be identified when analyzing the semantics of the terms in regular dictionaries. Inconsistencies can also be identified in professional classifications, such as the International Classification for Nursing Practice (ICNP®). In spite of comfort and well-being being considered separate terms, this classification defines comfort (code 10004655) using the concept of well-being: “sensation of physical ease and bodily well-being”.11 The international classification of nursing diagnoses, NANDA-International (NANDA-I), also features a new taxonomy proposal in the last edition, wherein the domain entitled “existential” integrates two distinct classes, entitled “well-being” and “comfort”.12
The World Health Organization (WHO) defines health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity”.13 This definition proposes that individuals are not healthy unless they have achieved holistic well-being, regardless the absence of spiritual dimension.14 Also, when considering the changes in the course of diseases and chronic illness, the WHO definition seems to suggest that these patients are definitely ill.14 Although the several criticisms, namely the completeness of well-being in all human life dimensions, the definition has never been adapted.14 Redefining health is challenging, but a new definition should comprise a broader perspective, and attempt different conditions and cultures.14
These inconsistencies formed the basis for the questioning of the similarities and the distinguishing attributes of the concepts of comfort, well-being and QoL, particularly in nursing knowledge, as these concepts have been integrated in nursing theories and research.
ComfortThe term “comfort” derives from the Latin “confortare” which means “become strong, comfort or encourage.” In a linguistic dictionary, the term is a synonym of “well-being”, and is defined as aid and solace in moments of affliction.15,16 Comfort has always been a central concern and concept in nursing and it is particularly important in the definition of the nature of nursing knowledge, the discipline, and the profession. The work of Morse and Kolcaba is widely recognized among the different theories that have analyzed the theme of comfort. Morse defines comfort as a result of therapeutic nursing interventions and underlines the idea of comfort as a process inherent in the act of comforting.15,17,18 The studies of Kolcaba have been based on the well-known theory of comfort, in which the author operationalizes the concept and defines it as “the immediate state of being strengthened by having the needs for relief, ease, and transcendence addressed in the four contexts of holistic human experience: physical, psychospiritual, sociocultural, and environmental”.8,p.251
Despite the international projection of the Morse and Kolcaba studies,8,17 the concept of comfort is present in other nursing theorists’ studies, such as Ida Jean Orlando (whose study defines comfort as a response to human needs), Sister Callista Roy (who stressed the importance of psychological comfort), Madeleine Leininger and Jean Watson (who defended comfort as essential to the care process), and Hildegard Peplau (who defended comfort as a fundamental human need associated with food, rest, sleep and communication).15,18
Well-beingThe word “well-being” derives from the Latin words “bene” and “stare”, which mean “being well”. The Oxford Dictionary defines well-being as “the state of being comfortable, healthy, or happy”.16 When quoted in scientific literature, it is usually identified as a related term to the concepts of happiness, positive experiences or ideas, life satisfaction, pleasure and prosperity.19 Well-being is also a multidimensional concept, with implications on one's physical, mental, social and environmental aspects of living.20 It concerns individual care in a healthy way and covers aspects such as awareness of the physical condition, stress reduction and self-responsibility in care. The strategies for achieving well-being help people reach new ways of understanding and controlling their lives, both in an individual and a collective scope.21
Orem's self-care theory and Watson's transpersonal theory are particularly relevant among the nursing theories that evoke the concept of well-being. In fact, in all Health Sciences theories, including the Nursing theories, well-being is often present as important in patients’ assessment. Orem's Self-Care Theory defines self-care as the performance of activities that individuals or caregivers perform for their benefit in order to maintain life, health and well-being.22 Also, in Watson's Transpersonal Theory,23 the author advocates the shaping of a system of humanistic and altruistic values, the instillation of faith and hope and the recognition of sensibility and feelings on the part of the nurses themselves as fundamental principles for the development of the nurse-patient relationship, and for promoting well-being.
Quality of lifeThe concept of QoL has been discussed in several areas of knowledge over time. Although there are several definitions of the concept, the majority of authors define the concept as the individual's perception of their personal situation in their own life in the physical, social, mental and spiritual dimensions.9,10 The study of QoL in the health field is relatively recent. The first studies emerged in the 1930s, but interest only began to grow from the 1960s, due to the unwanted consequences of the post-war period, when a search for the improvement of living conditions for humanity created greater interest in research of the concept by modern societies.10
Among the various definitions of the concept,2,5,24 the definition proposed by the World Health Organization Quality of Life Group is widely used9,p.1: “individuals’ perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns”. This definition considers the person's physical and psychological condition, the level of independence, social relationships, personal beliefs, the environment and culture. The assessment seems to be subjective and multidimensional, considering the cultural, social and environmental particularities of each person.9 It reflects the global condition of human life, personal interests with the enhancement of life dimensions, such as physical, political, moral, social, environmental, and spiritual dimensions.
Similar to previous concepts, several nursing theories have included the concept of QoL, such as Peplau, Rogers, King, Leininger and Parse.25 In Peplau's theory, QoL is a synonym for well-being or psychological health. Rogers and King describe QoL as a synonym for life satisfaction. Leininger believes that the concept of QoL is culturally constructed, which means, it is dependent on the values, beliefs and symbols of a given culture, representing a powerful force for promoting health and well-being. Parse describes the concept as representing the meaning that each individual attributes to the lived experiences.25
MethodsReview of nursing research using a concept analysis method and concerning the concepts of comfort, well-being and QoL. The search was conducted in the databases PubMed, Cinahl (with full text) and Scielo, using the terms “Comfort”, “Well-being”, “’Quality of Life” and “’Concept Analysis,” in the title and/or abstract. Concept analysis studies, regardless of the method, published in Portuguese, Spanish, English and French, up to 31 December 2015 were included. Narrative reviews, semantic analyses, editorials or letters to the editor, books or book chapters, and proceedings were excluded.
One researcher conducted the search in the first phase. Two researchers independently performed the analysis and screening of the results, and disagreements were subsequently analyzed by all researchers (Fig. 1). All references to the included studies were also analyzed.

The results were exported to EndNote X6, and a database was designed to collect the data according to the study objectives. Duplicates and studies that did not meet all the eligibility criteria were excluded. Since no instrument was found for the critical appraisal of concept analysis research, a generic consensual instrument was designed, based on the following criteria and research method procedures: clear definition of the concept, clear definition of the aim, and description of the concept analysis methodology in use. A score of 1 was given when the item was present and zero when it was unclear or absent. The differences in the scores were discussed by the researchers.
ResultsA total of 98 results were identified (Fig. 1). After duplicates removal, the full text reading and the screening of the references of the included articles, 18 studies were included in this review. Three studies concern the concept of comfort, three studies the concept of well-being, and 12 studies the concept of QoL (Table 1). The methods of concept analysis used were as follows: Beth Rodgers evolutionary model (n=3),26,27 and Lorraine Walker & Kay Avant model (n=15).28,29
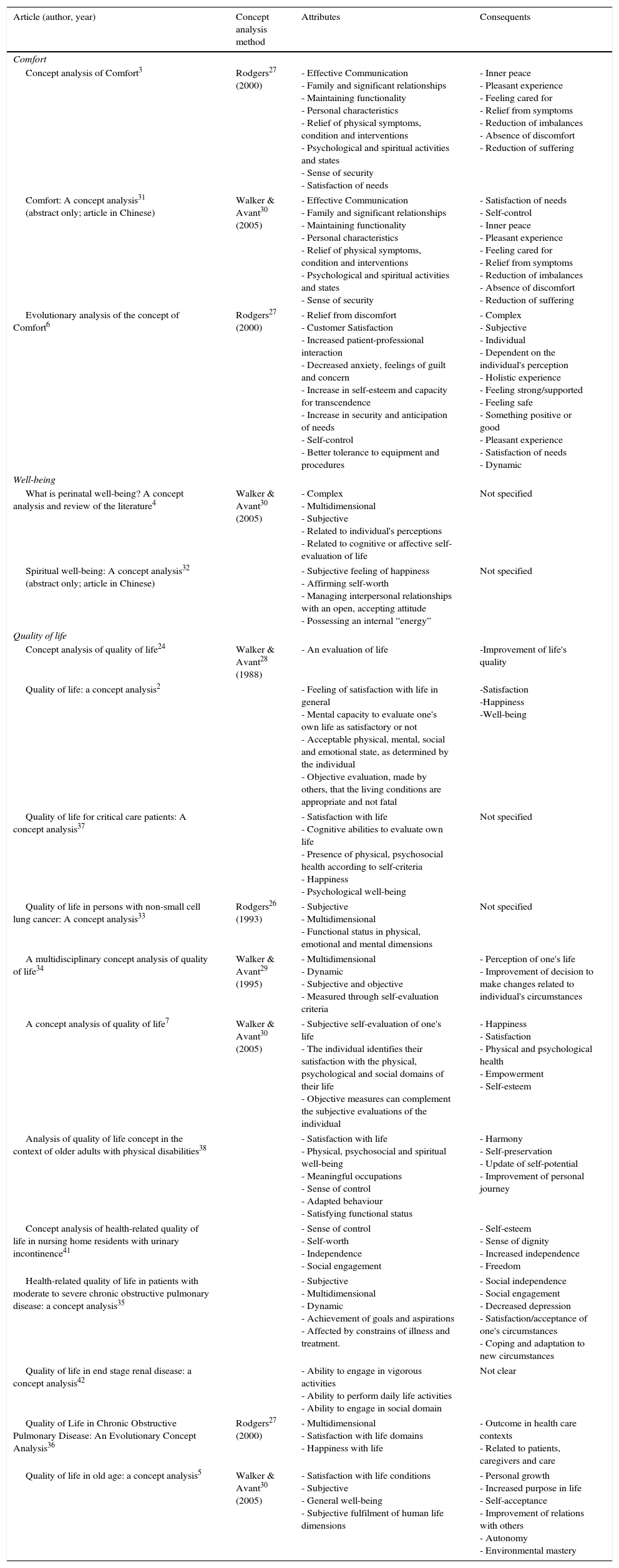
Attributes and consequents of the concepts of comfort, well-being and quality of life.
| Article (author, year) | Concept analysis method | Attributes | Consequents |
|---|---|---|---|
| Comfort | |||
| Concept analysis of Comfort3 | Rodgers27 (2000) | - Effective Communication - Family and significant relationships - Maintaining functionality - Personal characteristics - Relief of physical symptoms, condition and interventions - Psychological and spiritual activities and states - Sense of security - Satisfaction of needs | - Inner peace - Pleasant experience - Feeling cared for - Relief from symptoms - Reduction of imbalances - Absence of discomfort - Reduction of suffering |
| Comfort: A concept analysis31 (abstract only; article in Chinese) | Walker & Avant30 (2005) | - Effective Communication - Family and significant relationships - Maintaining functionality - Personal characteristics - Relief of physical symptoms, condition and interventions - Psychological and spiritual activities and states - Sense of security | - Satisfaction of needs - Self-control - Inner peace - Pleasant experience - Feeling cared for - Relief from symptoms - Reduction of imbalances - Absence of discomfort - Reduction of suffering |
| Evolutionary analysis of the concept of Comfort6 | Rodgers27 (2000) | - Relief from discomfort - Customer Satisfaction - Increased patient-professional interaction - Decreased anxiety, feelings of guilt and concern - Increase in self-esteem and capacity for transcendence - Increase in security and anticipation of needs - Self-control - Better tolerance to equipment and procedures | - Complex - Subjective - Individual - Dependent on the individual's perception - Holistic experience - Feeling strong/supported - Feeling safe - Something positive or good - Pleasant experience - Satisfaction of needs - Dynamic |
| Well-being | |||
| What is perinatal well-being? A concept analysis and review of the literature4 | Walker & Avant30 (2005) | - Complex - Multidimensional - Subjective - Related to individual's perceptions - Related to cognitive or affective self-evaluation of life | Not specified |
| Spiritual well-being: A concept analysis32 (abstract only; article in Chinese) | - Subjective feeling of happiness - Affirming self-worth - Managing interpersonal relationships with an open, accepting attitude - Possessing an internal “energy” | Not specified | |
| Quality of life | |||
| Concept analysis of quality of life24 | Walker & Avant28 (1988) | - An evaluation of life | -Improvement of life's quality |
| Quality of life: a concept analysis2 | - Feeling of satisfaction with life in general - Mental capacity to evaluate one's own life as satisfactory or not - Acceptable physical, mental, social and emotional state, as determined by the individual - Objective evaluation, made by others, that the living conditions are appropriate and not fatal | -Satisfaction -Happiness -Well-being | |
| Quality of life for critical care patients: A concept analysis37 | - Satisfaction with life - Cognitive abilities to evaluate own life - Presence of physical, psychosocial health according to self-criteria - Happiness - Psychological well-being | Not specified | |
| Quality of life in persons with non-small cell lung cancer: A concept analysis33 | Rodgers26 (1993) | - Subjective - Multidimensional - Functional status in physical, emotional and mental dimensions | Not specified |
| A multidisciplinary concept analysis of quality of life34 | Walker & Avant29 (1995) | - Multidimensional - Dynamic - Subjective and objective - Measured through self-evaluation criteria | - Perception of one's life - Improvement of decision to make changes related to individual's circumstances |
| A concept analysis of quality of life7 | Walker & Avant30 (2005) | - Subjective self-evaluation of one's life - The individual identifies their satisfaction with the physical, psychological and social domains of their life - Objective measures can complement the subjective evaluations of the individual | - Happiness - Satisfaction - Physical and psychological health - Empowerment - Self-esteem |
| Analysis of quality of life concept in the context of older adults with physical disabilities38 | - Satisfaction with life - Physical, psychosocial and spiritual well-being - Meaningful occupations - Sense of control - Adapted behaviour - Satisfying functional status | - Harmony - Self-preservation - Update of self-potential - Improvement of personal journey | |
| Concept analysis of health-related quality of life in nursing home residents with urinary incontinence41 | - Sense of control - Self-worth - Independence - Social engagement | - Self-esteem - Sense of dignity - Increased independence - Freedom | |
| Health-related quality of life in patients with moderate to severe chronic obstructive pulmonary disease: a concept analysis35 | - Subjective - Multidimensional - Dynamic - Achievement of goals and aspirations - Affected by constrains of illness and treatment. | - Social independence - Social engagement - Decreased depression - Satisfaction/acceptance of one's circumstances - Coping and adaptation to new circumstances | |
| Quality of life in end stage renal disease: a concept analysis42 | - Ability to engage in vigorous activities - Ability to perform daily life activities - Ability to engage in social domain | Not clear | |
| Quality of Life in Chronic Obstructive Pulmonary Disease: An Evolutionary Concept Analysis36 | Rodgers27 (2000) | - Multidimensional - Satisfaction with life domains - Happiness with life | - Outcome in health care contexts - Related to patients, caregivers and care |
| Quality of life in old age: a concept analysis5 | Walker & Avant30 (2005) | - Satisfaction with life conditions - Subjective - General well-being - Subjective fulfilment of human life dimensions | - Personal growth - Increased purpose in life - Self-acceptance - Improvement of relations with others - Autonomy - Environmental mastery |
The oldest study was published in 1991 and was related to the concept of QoL.24 The majority of studies were developed with adult populations, and some reported specific groups such as critically-ill patients (n=1), cancer patients (n=1), the elderly (n=2), patients with urinary incontinence (n=1), patients with chronic obstructive pulmonary disease (n=2), and renal patients (n=1) (Table 1). One study with neonates was also found.
Two of the studies were in Chinese and only the abstract was in English,31,32 but the clarity and completeness of the results in the abstract was considered relevant and both were included in the analysis. One of these studies focused on the concept of comfort,31 and the other focused on the concept of spiritual well-being.30 All studies included in the review were analyzed in relation to the attributes and consequents of the three concepts under study (Table 1).
The results demonstrate the complex and subjective nature of the concepts and their relation with the individuals’ self-esteem and perception (Table 2). Despite this, distinct attributes were also observed for each concept. Thus, comfort seems to be more related to the symptom relief and/or reduction of imbalances or discomfort, inner peace, security and effective communication. The concept of well-being lies on a psycho-spiritual basis, associated with happiness and an “internal energy”. QoL appears as a broader concept, associated with life improvement, dignity and achieving autonomy and personal goals (Table 2).
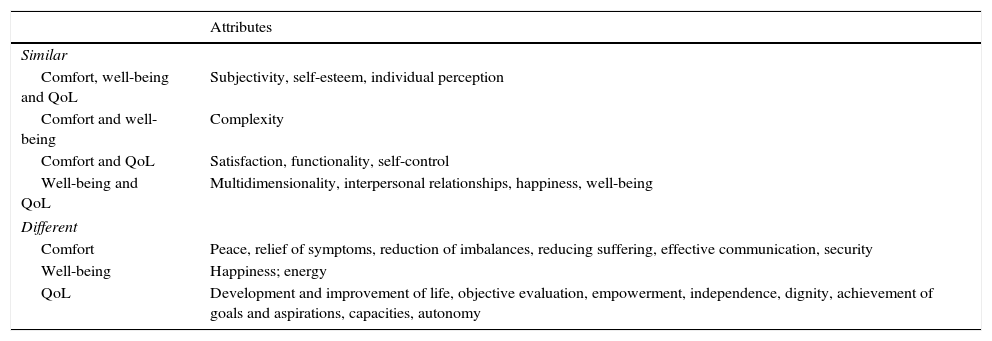
Summary of similar and different attributes between the concepts of comfort, well-being and quality of life (QoL).
| Attributes | |
|---|---|
| Similar | |
| Comfort, well-being and QoL | Subjectivity, self-esteem, individual perception |
| Comfort and well-being | Complexity |
| Comfort and QoL | Satisfaction, functionality, self-control |
| Well-being and QoL | Multidimensionality, interpersonal relationships, happiness, well-being |
| Different | |
| Comfort | Peace, relief of symptoms, reduction of imbalances, reducing suffering, effective communication, security |
| Well-being | Happiness; energy |
| QoL | Development and improvement of life, objective evaluation, empowerment, independence, dignity, achievement of goals and aspirations, capacities, autonomy |
In spite of all three concepts having been widely studied in different contexts (concept analysis, theory development, empirical studies), the data show that there is still a lot of subjectivity in the definition. Also, no studies of comparison between the concepts were found.
One of the strongest points focuses on defining the attributes of the concept, since it is on this level that weaknesses can be shown to exist. The studies were based on the methods proposed by Beth Rodgers26,27 and Lorraine Walker & Kay Avant.28,29 Despite the methodological differences, both are similar in the definition of the attributes, which represent the core of the concept or the unique characteristics of each concept. Several studies highlight the complex, multidimensional, subjective, individual and dynamic nature of the concepts of comfort, well-being and QoL.4–6,33–35 However, these are not unique qualities of the concepts. The existence of such a wide set of attributes common to the three concepts backs the inherent difficulties in their definition and operationalization. Further specific and exclusive attributes need to be identified to clarify each concept.
By analyzing the attributes of the concept of well-being it is possible to state that the concept can be assimilated to comfort. When looking at the etymological origin of both words, the concept of comfort is derived from the Latin word confortare which means to give strength, force, and the concept of well-being refers to a pleasant corporal or spiritual experience. Even though it is identified in literature as a state, a process and an outcome, the etymological origin of the concept of comfort leads to an action or intervention (to comfort). This intervention, in turn, seems to be centred on the activities that help the person to feel stronger, supported or empowered. The etymology of well-being refers to a state, highlighting at once the Cartesian dualism between body and spirit. Despite the scarcity of concept analysis studies in the area of well-being, one such study uses the terminology “spiritual well-being”.32 In fact, while comfort tends to be used in a more holistic perspective, well-being tends to be more confined to the psychological or spiritual dimensions, as in the studies of Bond and Levasseurs and colleagues,37,38 in which the authors identify “psychological or spiritual well-being” as attributes of QoL (instead of using the concept of spiritual comfort). This idea is also present in nursing theories, where well-being tends to be presented on a psychological, social and spiritual perspective rather than on a physical perspective. The WHO reinforces this idea through the definition of mental health “as a state of well-being in which every individual realizes his or her own potential”.43
This idea is also sustained by Kolcaba's Comfort Theory,8 in which the author presents comfort as a holistic concept represented by three types of comfort (relief, ease and transcendence) that may occur in four contexts: physical, psycho-spiritual, social and environmental. Despite the holistic nature of the concept, the environmental perspective seems to represent a unique characteristic of the concept. If, on the one hand, it seems to be more intuitive and consensual to talk about spiritual well-being (instead of spiritual comfort), on the other hand the use of environmental comfort seems to be more intuitive.39 In addition to these ideas, comfort is closely associated with the nature of nursing care, as previously stated by Nightingale in “Notes on Nursing”.40 This significant study made it possible, later on, for the development of the well-known Kolcaba's Comfort Theory,8 and it is also present in many others, such as the theories of Roy, Leinninger, Watson or Peplau.15,17 Furthermore, well-being is a concept traditionally associated with psychology.37,38,43
The concept of QoL seems a broad concept, and has been well discussed by authors and defined as the individual's perception of their own life through personal beliefs and values.5,7,34 Independence and the sense of freedom appear as attributes presented exclusively in the concept of QoL,41 and satisfaction is a critical attribute. However, studies also emphasize the satisfaction of specific needs,3,6,31 since general satisfaction with life is highlighted in QoL.2,5,36–38 On the other hand, in both concepts (comfort and QoL), the state of satisfaction across physical, psychological, social and spiritual dimensions is common, although it may depend on the individual's perception of their own values and beliefs and the support they have.
Despite these considerations, the results highlight the paradoxical nature of the concept of well-being. On the one hand, studies demonstrate the use of the concept essentially concerning the psychological and spiritual dimensions. On the other hand, the concept is used in an almost indistinct way in the concepts of comfort and QoL. This suggests that caution should be taken in future studies, particularly as regards the correct use and framing of the concepts.
These three concepts are also related to the health definition proposed by the WHO, and are raised as an attempt to measure the subjective dimensions of health. As highlighted in the results section, the concept of comfort tends to be used more often in a holistic perspective, within the specific context of nursing or life-threatening situations. QoL represents a broader concept, specifically related to the perception and satisfaction of the individual with own life, which is probably more in accordance with the concept of health. Well-being is particularly related with the psychological dimension, which is reinforced by the definition of mental health proposed for the WHO.43
LimitationsResults should be addressed as a contribution to further research and discussion. The search was based in three databases looking for concept analyses studies. No grey literature or other publications were considered. This study explored shared attributes of the concept, but further research should address specific and exclusive attributes in order to clarify each concept.
ConclusionsComfort and well-being are commonly used interchangeably and both are presented as concepts related to QoL. The inconsistencies at a theoretical level could be the basis of several studies for the analysis of these concepts, as well as knowledge dispersion without any clear direction. This study concerns the results of several concept analysis research studies, supporting the idea that comfort, well-being and QoL are not surrogate terms but, rather, related concepts that share common attributes.
QoL is a broader concept, predominantly characterized by the satisfaction with life in general. It is a state that depends on each person's perception of such. Comfort is a concept that is inherently linked to the practice of nursing care and in a health context. It is characterized by the satisfaction of one's needs, by the person feeling strong, safe, supported and cared for. Well-being tends to be used in a more psychologically or spiritually oriented perspective and, even though it can be used in a broader and more holistic way, it is traditionally linked to psychology-sourced thinking. Thus, it seems that the concept of comfort is particularly used within the nursing profession, while the concept of well-being is particularly addressed to the psychological dimension and the mental health definition. The concept of QoL seems to be more adequate to the overall definition of health, since it is a broader concept, which includes the individual's perception about their own life, including health in all human life dimensions.
This study opens a new perspective about the correct use and framing of the concepts in practice, but also in research and education.
AuthorshipSP and LF contributed equally to this study. Conception and design of the work, acquisition of data, or analysis and interpretation of data (SP, LF); drafting the article or revising it critically for important intellectual content (SP, LF, AM, SC, JCM); final approval of the version to be published (SP, LF, AM, SC, JCM).
Conflicts of interestThe authors declare no conflicts of interest.
FundingFunding for completion of this paper was supported by São Paulo Research Foundation (FAPESP).