



To assess the association between muscle strength and early cardiovascular risk (CVR) markers in sedentary adults.
Materials and methodsA total of 176 sedentary subjects aged 18–30 years were enrolled. Body mass index and fat percentage were calculated, and waist circumference, grip strength by dynamometry, systolic blood pressure, diastolic blood pressure, mean arterial pressure, and maximal oxygen uptake by VO2max were measured as CVR markers. A multivariate logistic regression analysis was used to assess associations between muscle strength and CVR markers.
ResultsInverse correlations were found between muscle strength and adiposity (r=−.317; P=.001), waist circumference (r=−.309; P=.001), systolic blood pressure (r=−.401; P=.001), and mean arterial pressure (r=−.256; P=.001). Subjects with lower levels of muscle strength had a 5.79-fold (95% CI 1.57–9.34; P=.008) risk of having higher adiposity levels (≥25%) and a 9.67-fold (95% CI=3.86–19.22; P<.001) risk of having lower physical capacity values for VO2max (≤31.5mL/kg/min−1).
ConclusionsIn sedentary adults, muscle strength is associated to early manifestations of CVR. It is suggested that muscle strength testing is added to routine measurement of VO2max and traditional risk factors for prevention and treatment of cardiovascular risk.
Evaluar la asociación entre la fuerza muscular y marcadores tempranos de riesgo cardiovascular (RCV) en adultos sedentarios.
Materiales y métodosUn total de 176 sujetos sedentarios, entre los 18 y 30 años de edad, fueron incluidos en el estudio. Se calculó el índice de masa corporal, el porcentaje de grasa o adiposidad y se midió la circunferencia de la cintura, la fuerza prensil por dinamometría, la tensión arterial sistólica, la tensión arterial diastólica, la tensión arterial media y el consumo máximo de oxígeno por VO2máx como marcadores de RCV. Un análisis de regresión logística multivariado fue usado para evaluar las asociaciones entre la fuerza muscular prensil y los marcadores de RCV.
ResultadosCorrelaciones inversas fueron encontradas entre la fuerza muscular y los indicadores de adiposidad (r=−0,317; p=0,001), circunferencia de la cintura (r=−0,309; p=0,001), tensión arterial sistólica (r=−0,401; p=0,001) y tensión arterial diastólica (r=−0,256; p=0,001). Los sujetos con menores niveles de fuerza muscular prensil mostraron 5,79 veces (IC 95%=1,57-9,34; p=0,008) mayor riesgo de presentar niveles de adiposidad más elevados (≥25%) y 9,67 veces (IC 95%=3,86-19,22; p<0,001) mayor riesgo de presentar menores valores de capacidad física por VO2máx (≤31,5mL/kg/min−1).
ConclusionesLa fuerza muscular en adultos sedentarios se relaciona con manifestaciones tempranas de RCV. Se sugiere incluir la evaluación de la fuerza muscular junto a la determinación convencional del VO2máx y la medición de los factores de riesgo tradicionales en la prevención y tratamiento del RCV.
Recent research unequivocally shows that fitness, estimated by aerobic fitness or VO2max, is a significant predictor of cardiovascular and all-cause morbidity and mortality in both sexes.1–3 Similarly, in both men4 and women,5 muscle strength represents a different and independent predictor of morbidity and mortality in adolescents and young adults.6
Low fitness has an even greater significance as a cardiovascular risk (CVR) indicator7 than other traditional CVR factors such as dyslipidemia, high blood pressure, smoking, or obesity.8 For example, in the non-Hispanic population there is evidence that a low-grade inflammatory state is inversely associated with muscle strength,9 VO2max,10 and lean body mass.11,12 While reference data in the Hispanic population are limited, the available data suggest that the values of these three variables related to muscle mass/quality may be lower. For example, upper body strength, as measured by dynamometry, is lower in the Colombian population13 as compared to reference values in the United Kingdom,14 and also in Brazilian adults when compared to the reference values in Europe or North America.15 The US National Health and Nutrition Examination Survey (NHANES) showed that Mexican American adults have a lower muscle mass than Caucasian Americans.16 A lower aerobic capacity has also been reported in Hispanic American adolescents and children, regardless of body composition.17
In support of this hypothesis, a recent study conducted in North America showed an inverse association between percent lean body mass and the risk of coronary heart disease in young Hispanic adults which was not seen in their Caucasian or non-Hispanic black counterparts.18,19 Although evidence to support an active lifestyle is available, a majority of the population leads a sedentary lifestyle. The search for public policies and effective strategies to promote physical activity and prevent sedentary lifestyles should therefore be a priority on the national agenda.20 The objective of this study was therefore to assess the association between grip muscle strength and early CVR markers in sedentary adults.
Subjects and methodsA descriptive, cross-sectional study was conducted during the first six months of 2012 in 176 sedentary men aged 18–30 years from the metropolitan area of Cali (Colombia). The concepts of sedentary lifestyle of the US Department of Health and Human Services21 and other authors22–26 were applied. These define a sedentary individual as any subject who spends less than 10% of his daily energy expenditure in the performance of physical activities or performs less than 150min of aerobic activity of moderate intensity weekly or 75min of aerobic physical activity weekly, as estimated by the International Physical Activity Questionnaire. The sample was selected by advertising and sampling by intention. Subjects with a medical or clinical diagnosis of major systemic disease (including malignant conditions such as cancer), type 1 or 2 diabetes mellitus, high blood pressure, hypothyroidism/hyperthyroidism, a history of drug or alcohol abuse, were using multivitamin preparations, had a body mass index (BMI)≥35kg/m,2 and inflammatory (trauma, contusions) or infectious conditions were excluded from the study. Written informed consent was obtained from each participant, and the ethics committee of the academic center approved the intervention in compliance with the ethical standards set out in the Declaration of Helsinki and the applicable legal regulations in Colombia governing research in humans (Decision 008430 of the Colombian Ministry of Health). The participants who accepted and signed informed consent were appointed for the following procedures:
Clinical measurementThe following data were collected from each participant: (a) a family history of CVR, (b) a personal history, (c) a completed physical activity questionnaire, and (d) an anthropometric assessment including height, weight, and waist circumference (WC), measured using procedures standardized by López et al.22 for the Colombian population. Height was measured using a portable stadiometer (SECA 206®, Hamburg, Germany) (range 0–220cm) with a precision of 1mm. Weight was measured using a Tanita® scale, model BC554 Inerscan Ironman™ (Continental Scale Corp., Bridgeview, IL, USA) (range 0–150kg), with a precision of 500g. These variables were used to calculate BMI in kg/m.2 WC was measured at the midpoint between the iliac crests and lower costal margin using a plastic measuring tape with a precision of 0.5cm (Holtain Ltd., Crymych Dyfed, United Kingdom). Adiposity or percent fat (%F) was estimated using the four-point tactile electrode segmented bioelectrical impedance equipment BC554 Inerscan Ironman™ from Tanita® (Continental Scale Corp., Bridgeview, IL, USA) in accordance with the indications and equations given in the user's manual. Induction frequency was assessed at an intensity of 50kHz, with a sensitivity for estimating fat mass of 0.1kg (0.1%). The measurement was taken after the participants had fasted for 2h, with the bladder empty, and on a non-conducting surface. Blood pressure was measured twice on the right arm, with a 5-min interval, with the participants in a sitting position and after a 10-min rest, using a Welch Allyn® digital sphygmomanometer, model OSZ 5 (Inc, Arden, Illinois, USA). Mean arterial pressure (MAP) was calculated using the formula: (2×systolic blood pressure [SBP]+diastolic blood pressure [DBP])/3.
Muscle strength by hand dynamometryThis was measured using a T-18 TKK SMEDLY III® analogical dynamometer (Takei Scientific Instruments Co., Ltd, Niigata, Japan), making two alternate attempts with each hand in a standardized standing position, with arms parallel to the body and no contact.
Aerobic capacityThis was assessed using the Course Navette, aka the multi-stage fitness test or 20-m shuttle run test, a maximum incremental indirect field test. VO2max was calculated from the result of the test using the following formula:
where V is the final velocity achieved in the test (V=8+0.5×last stage completed) and E the age in years.Early cardiovascular risk markers
The CVR criteria reported by the National Cholesterol Education Program,23 the International Diabetes Federation,24 and the US Department of Health21 were used: BMI≥25kg/m2, abdominal obesity (WC≥88cm), SBP ≥ 130mmHg, DBP≥85mmHg, adiposity ([%F]≥25%), and fitness by VO2max (≤31.5mL/kg/min−1). The abovementioned measurements were taken using certified devices and according to the standards of the international biological program prepared by the International Council of Scientific Unions, including the essential procedures for the biological study of human populations.25
Statistical analysisData were analyzed using the Statistical Package for the Social Sciences, version 18 (SPSS, Chicago, IL, USA). A Levine test was used for testing the normal distribution of the study variables. Each of these dependent variables was recoded into tertiles to test its relationship to muscle strength and early CVR markers. For differences between the tertiles, a one-way analysis of variance (ANOVA) was used for the continuous variables. The p value of post hoc hypothesis tests was determined using the Tukey correction for multiple comparisons adjusted for age, BMI, and WC. ORs and 95% CI adjusted for the confounding factors BMI and WC were estimated. Forward selection and step by step selection methods were used. The variable incorporation procedure was terminated when the significance of p provided by a variable upon inclusion in the regression exceeded 0.05 between grip muscle strength and early CVR markers.
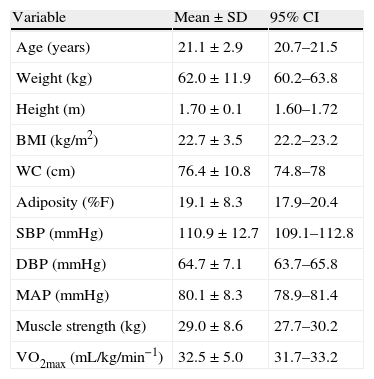
ResultsTable 1 summarizes the general characteristics of the participants. All the parameters evaluated were within the range considered healthy for their age.
Anthropometric and clinical characteristics of the study population (n=176).
| Variable | Mean±SD | 95% CI |
| Age (years) | 21.1±2.9 | 20.7–21.5 |
| Weight (kg) | 62.0±11.9 | 60.2–63.8 |
| Height (m) | 1.70±0.1 | 1.60–1.72 |
| BMI (kg/m2) | 22.7±3.5 | 22.2–23.2 |
| WC (cm) | 76.4±10.8 | 74.8–78 |
| Adiposity (%F) | 19.1±8.3 | 17.9–20.4 |
| SBP (mmHg) | 110.9±12.7 | 109.1–112.8 |
| DBP (mmHg) | 64.7±7.1 | 63.7–65.8 |
| MAP (mmHg) | 80.1±8.3 | 78.9–81.4 |
| Muscle strength (kg) | 29.0±8.6 | 27.7–30.2 |
| VO2max (mL/kg/min−1) | 32.5±5.0 | 31.7–33.2 |
WC: waist circumference; SD: standard deviation; 95% CI: 95% confidence interval; BMI: body mass index; DBP: diastolic blood pressure; MAP: mean arterial pressure; SBP: systolic blood pressure; VO2max: maximal oxygen consumption; %F: percent fat.
Subjects with higher grip muscle strength (third tertile) showed lower values in the CVR markers, WC and adiposity (first tertile), p<0.05. This same trend (first vs third tertile) was found in aerobic capacity by VO2max and in muscle strength by dynamometry (30.4±4.3, 95% CI=29.2–31.5 vs 36.2±4.4, 95% CI=35.1–37.4) and (20.7±8.5, 95% CI=20.5–25.0 vs 38.4±3.9, 95% CI=37.3–39.4) respectively (Table 2).
Muscle strength values and their relationship to cardiovascular risk markers in the study population (n=176).
| Variable | 1st Tertile (n=59). | 2nd Tertile (n=63) | 3rd Tertile (n=54) |
| BMI (kg/m2) | 23.0±3.9 | 22.4±3.2 | 22.7±3.5 |
| WC (cm) | 79.1±7.9 | 75.3±15.0 | 75.2±7.3* |
| Adiposity (%F) | 20.0±8.0 | 22.6±8.6 | 14.3±5.9*** |
| SBP (mmHg) | 115.1±13.0 | 111.9±14.1** | 106.5±9.5** |
| DBP (mmHg) | 66.2±7.6 | 64.9±6.6 | 63.2±6.9 |
| MAP (mmHg) | 81.4±9.0 | 81.6±7.9 | 77.6±7.3** |
| Muscle strength (kg) | 20.7±8.5 | 26.8±3.2*** | 38.4±3.9*** |
| VO2max (mL/kg/min−1) | 30.4±4.3 | 31.2±4.2 | 36.2±4.4*** |
WC: waist circumference; BMI: body mass index; DBP: diastolic blood pressure; MAP: mean arterial pressure; SBP: systolic blood pressure; VO2max: maximal oxygen consumption; %F: percent fat.
Differences between measurements (one-way ANOVA, Tukey post hoc), adjusted for age, BMI, and WC.
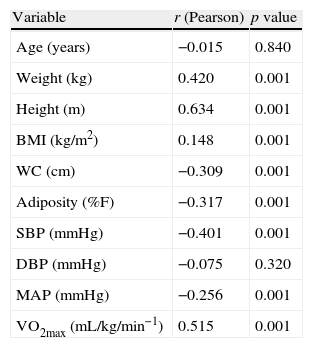
Higher values of grip muscle strength showed a significant positive correlation to body weight (r=0.420; p=0.001), height (r=0.634; p=0.001), BMI (r=0.148; p=0.001), and aerobic capacity by VO2max (r=0.515; p=0.001). Inverse correlations were also found between muscle strength and the indicators of adiposity (r=−0.317; p=0.001), WC (r=−0.309; p=0.001), SBP (r=−0.401; p=0.001), and MAP (r=−0.256; p=0.001) (Table 3).
Relationship between muscle strength and cardiovascular risk markers in the general population (n=176).
| Variable | r (Pearson) | p value |
| Age (years) | −0.015 | 0.840 |
| Weight (kg) | 0.420 | 0.001 |
| Height (m) | 0.634 | 0.001 |
| BMI (kg/m2) | 0.148 | 0.001 |
| WC (cm) | −0.309 | 0.001 |
| Adiposity (%F) | −0.317 | 0.001 |
| SBP (mmHg) | −0.401 | 0.001 |
| DBP (mmHg) | −0.075 | 0.320 |
| MAP (mmHg) | −0.256 | 0.001 |
| VO2max (mL/kg/min−1) | 0.515 | 0.001 |
WC: waist circumference; BMI: body mass index; DBP: diastolic blood pressure; MAP: mean arterial pressure; SBP: systolic blood pressure; VO2max: maximal oxygen consumption; %F: percent fat.
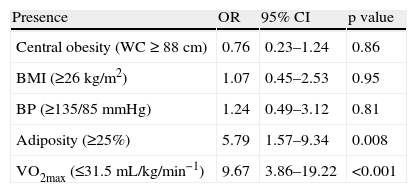
In this study, subjects with low muscle strength levels (first tertile) had a 5.79-fold (95% CI=1.57–9.34; p=0.008) greater risk of having higher adiposity levels (≥25%) and a 9.67-fold (95% CI=3.86–19.22; p<0.001) greater risk of having lower values of physical fitness by VO2max (≤31.5mL/kg/min−1). No associations were found in any other markers related to CVR (Table 4).
Risk indices (odds ratio) of lower grip muscle strength values with early cardiovascular risk markers in the general population (n=176).
| Presence | OR | 95% CI | p value |
| Central obesity (WC≥88cm) | 0.76 | 0.23–1.24 | 0.86 |
| BMI (≥26kg/m2) | 1.07 | 0.45–2.53 | 0.95 |
| BP (≥135/85mmHg) | 1.24 | 0.49–3.12 | 0.81 |
| Adiposity (≥25%) | 5.79 | 1.57–9.34 | 0.008 |
| VO2max (≤31.5mL/kg/min−1) | 9.67 | 3.86–19.22 | <0.001 |
WC: waist circumference; 95% CI: 95% confidence interval; BMI: body mass index; OR: odds ratio; BP: blood pressure; VO2max: maximal oxygen consumption.
Association estimated using multivariate logistic regression models.
Based on the results of this study, grip muscle strength of the tested adults is significantly associated with early CVR markers. The role of lower fitness as a CVR factor is even greater than that of other traditional CVR factors such as dyslipidemia, high blood pressure, smoking, and obesity, as recently reported by Lee et al.26 In addition to fat mass amount and distribution, the amount, quality, and function of muscle mass may contribute to inflammatory cytokine increase or decrease, endothelial dysfunction, and altered glucose and lipid levels.27,28
The findings in this study show that adults with a higher grade of muscle strength (third tertile) have lower SBP, WC, %F, and BMI values, regardless of the fitness level measured by VO2max, as compared to those with lower grip muscle strength assessed by dynamometry (Table 2). Previous studies showed a relationship between muscle strength and some CVR factors in populations with similar characteristics to our study population.29,30 Several prospective studies similarly showed that muscle strength was inversely associated with all-cause mortality,31,32 including that caused by cardiovascular disease and cancer.33,34
Inverse relationships were also similarly found between grip strength and lower SBP (r=−0.401; p=0.001) and MAP (r=−0.256; p=0.001), a finding which agrees with the findings recently reported by Artero et al.35 in a sample of 1506 men with CVR. After a 20-year follow-up, these authors found a lower risk of all-cause and CVR mortality in participants who had higher values of both muscle strength and fitness by VO2max. The findings by Silventoinen et al.30 in subjects with similar characteristics to our study participants also showed that lower muscle fitness values (as assessed by grip dynamometry) were inversely associated with a prevalence of ischemic heart disease and subarachnoid hemorrhage. However, the hypothesis that an improved muscle condition is related to lower CVR marker values (and may thus be considered as a protective factor) could not be elucidated in this study due to the limitations inherent in its design.
On the other hand, subjects with low muscle strength levels (first tertile) had a 5.79-fold (95% CI=1.57–9.34; p=0.008) greater risk of having higher adiposity levels (%F≥25). As regards this CVR indicator, two studies have hypothesized the protective role of fat-free mass in early manifestations of CVR. In the first study, published by Mason et al.,36 low muscle fitness was seen to be associated with a greater chance of gaining at least 10kg of weight regardless of BMI and VO2max in men and women. In the second study, Jackson et al.37 showed a greater prevalence of excess total fat (adiposity>25%) and abdominal obesity (WC>102cm) in the group with lower muscle fitness. However, in order to be able to recommend the measurement of this particular health indicator, validation and follow-up studies need to be conducted in our population.
Some study limitations should be considered. For example, the sample size, population characteristics, study design, and type of sampling may have introduced bias. On the other hand, other variables possibly associated with CVR such as race, socioeconomic, nutritional, and social aspects, and physical activity levels were not considered. However, our results agree with data reported by other international studies.7,15,16,29–38 In conclusion, the findings show that muscle strength in sedentary adults is related to early signs of CVR. It is recommended that muscle strength assessment be included, together with the conventional measurement of VO2max and the traditional risk factors, in CVR prevention and treatment.
FundingThis study had no external funding source.
Conflicts of interestThe authors state that they have no conflicts of interest.
Please cite this article as: Triana-Reina HR, Ramírez-Vélez R. Asociación de la fuerza muscular con marcadores tempranos de riesgo cardiovascular en adultos sedentarios. Endocrinol Nutr. 2013;60:433–438
This article is part of the Master Thesis of HRTR by Antioquia University.
