


To evaluate satisfaction and short-term impact on metabolic control of diabetes monitoring through the DiabeTIC website.
Patients and methodsA prospective, uncontrolled intervention study was conducted in 32 patients aged 29.7±9.7 years (65% female) incorporated to the telemedicine platform DiabeTIC between March and September 2012. All patients completed a satisfaction questionnaire in the first month, and impact on metabolic control was evaluated at three and six months.
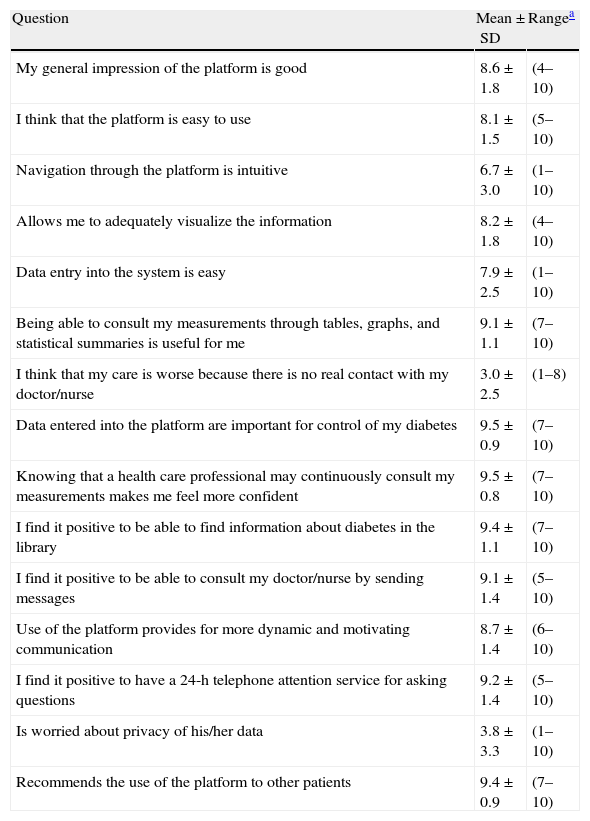
ResultsIn the satisfaction survey conducted in the first month of follow-up, the following mean scores (0–10) were obtained: overall impression with the platform: 8.6±1.8; ease of use: 8.1±1.5; intuitive navigation: 6.7±3.0; value of measurements: 9.1±1.1; importance of the platform in diabetes management: 9.5±0.9; sense of security: 9.5±0.8; value of the library: 9.4±1.1; value of messages: 9.1±1.4, and recommendation to use the platform: 9.4±0.9. Glycosilated hemoglobin concentrations significantly improved at six months as compared to study start (7.0±0.8 versus 8.1±1.9; p=0.007). Nine patients were discharged from DiabeTIC before completing six months of follow-up.
ConclusionsPatients with diabetes monitored through the DiabeTIC website report a high degree of satisfaction, showing improved metabolic control at short-term follow-up.
Evaluar la satisfacción y el impacto sobre el control metabólico a corto plazo del seguimiento de la diabetes a través de la página web DiabeTIC.
Material y métodosEstudio prospectivo de intervención no controlado realizado en 32 pacientes de 29,7±9,7 años de edad (65% mujeres) incorporados a la plataforma de telemedicina DiabeTIC entre marzo y septiembre de 2012. Todos los pacientes cumplimentaron en el primer mes un cuestionario de satisfacción, analizándose la evolución del control metabólico a los 3 y 6 meses de seguimiento.
ResultadosEn la encuesta de satisfacción realizada en el primer mes de seguimiento se obtuvieron las siguientes puntuaciones medias (0 a 10): impresión general con la plataforma: 8,6±1,8; facilidad de uso: 8,1±1,5; navegación intuitiva: 6,7±3,0; utilidad de las mediciones: 9,1±1,1; importancia de la plataforma en el control de la diabetes: 9,5±0,9; sensación de seguridad: 9,5±0,8; utilidad de la biblioteca: 9,4±1,1; utilidad de los mensajes: 9,1±1,4, y recomendación de uso de la plataforma: 9,4±0,9. Las concentraciones de hemoglobina glicosilada mejoraron significativamente a los 6 meses de seguimiento respecto al inicio del estudio (7,0±0,8 versus 8,1±1,9%; p=0,007). Nueve pacientes fueron dados de baja de DiabeTIC antes de completar 6 meses de seguimiento.
ConclusionesLos pacientes con diabetes seguidos a través de la página web DiabeTIC comunican un elevado grado de satisfacción, observándose a corto plazo una evolución favorable del control metabólico.
In 2008, the Andalusian Agency for Health Technology Assessment (AETSA) and the Spanish Ministry of Health and Consumer Affairs jointly issued the results of a systematic review of the medical literature and an economic evaluation whose main objective was to ascertain whether the use of information and communication technologies (ICTs) could improve the effectiveness and efficiency of and satisfaction with metabolic control in patients with diabetes.1 The authors of this study concluded that telemedicine applied to diabetes control is effective (good quality of evidence) and efficient (good to fair quality of evidence) and that its users are highly satisfied with it (good quality of evidence). They recommended that health care institutions should have the infrastructure required to provide ICTs to patients with diabetes, and that research should be conducted to find the best way to implement these ICTs in health care organizations.1
Two years later, the Group of New Technologies of the Spanish Diabetes Society (SED) issued a position statement on the use of telemedicine for diabetes control that described some characteristics and results of the use of telemedicine for the care of patients with diabetes and proposed a ten point plan for the use of telematic systems in diabetes care. Like AETSA, this group also stressed the importance of creating the infrastructure for the development of telemedicine.2
Despite these recommendations, few Spanish health centers have implemented telematic care for people with diabetes, as is shown by the low number of papers referring to this modality of care which are submitted to national meetings and publications.3–9 Moreover, most such reports refer to patients with very specific profiles, such as pregnant women3,4 or patients with insulin pumps.5–8 Finally, in most studies published to date on telemedicine and diabetes, the information was transmitted between patients and professionals by telephone, short message services (SMS), video conference, or electronic mail.1,10–12 Very few studies used web sites specifically developed for the telematic care of diabetic patients.9,13–15 Thus, the purpose of this study was to assess satisfaction with short-term metabolic control and its impact in a cohort of diabetic patients monitored through the DiabeTIC web site, recently developed in Spain for the telematic monitoring of patients with diabetes.
Subjects and methodsA prospective, open-label, non-controlled, intervention pilot study was designed to analyze the satisfaction with and the impact on metabolic control in a cohort of diabetic patients monitored through the DiabeTIC telemedicine platform. This web site, developed by Sanofi and Orange, is specifically designed for monitoring people with diabetes and has been accessible on the Internet to patients and professionals since mid-2012 at the address https://www.diabeticservicios.es/. This web site allows for remote two-directional communication between health care professionals and patients with diabetes, providing for the remote monitoring of blood glucose control, remote diabetic education, consultation through messages between professionals and patients, and the design and conduct of remote surveys. Professionals may sign up patients, assign them to specific groups and subgroups (e.g. “type 1 diabetes with pump”) where the measurements to be made (blood glucose, blood glucose/insulin, or blood glucose/insulin/carbohydrate servings) and the periodicity of these measurements as well as visits to be made by health care professionals are established, and may prescribe the treatment to be received by the patient. Once included, patients may enter their measurements (blood glucose, insulin dose, and carbohydrate servings), consult their statistics, see and modify the treatment prescribed by their physicians, write and read messages, see documents in the library, and answer questionnaires proposed by the assigned professionals.
The subjects eligible for the study were patients with diabetes older than 14 years on insulin treatment who attended the outpatient clinics of the endocrinology unit of Hospital Universitario Puerto Real (Cádiz) from March to September 2012, had Internet access in their homes, and could potentially achieve a greater benefit from the implementation of telemedicine. These included patients with type 1 diabetes on intensive therapy, type 1 diabetes in preconception control and during pregnancy, gestational diabetes, and patients with difficult access to hospital, mainly because of the long distances involved.2 This study was approved by the research ethics committee of Hospital Puerto Real (Cádiz) before study start.
After signing the corresponding informed consent, the patients were provided with an individual access code and password and were instructed on the use of the DiabeTIC web site platform on the same day of consultation. Blood glucose control levels entered by the patients into the web platform were monitored every 15 days. At these evaluations, health care staff proposed any treatment changes required. Blood glucose controls were also assessed through the web site whenever the patients deemed it appropriate, and all messages were answered. In all cases, the patients continued to be routinely monitored at the clinics, and there was no telephone contact. Patients were informed of the possibility of withdrawing telematic monitoring at any time and continuing with routine monitoring.
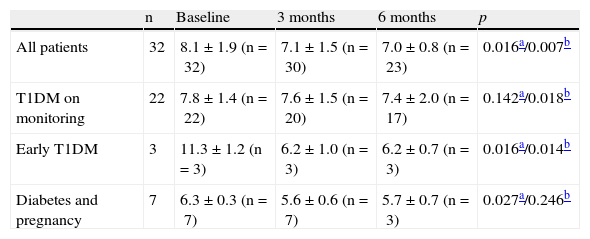
At the end of the first month of telematic monitoring, the patients completed a satisfaction questionnaire online consisting of 15 items which patients scored using a 10-point Likert scale where 1 point denoted that the patient “completely agreed” and 10 points that he/she “completely disagreed” with the statement in the item. The items in the questionnaire were mostly taken from other studies analyzing satisfaction levels in patients on telematic monitoring.16,17 Finally, glycosylated hemoglobin (HbA1c) levels in venous blood were assessed in all patients at study entry and after three and six months of monitoring at the DiabeTIC platform (Table 3).
Change in glycosylated hemoglobin levels after six months of monitoring in DiabeTIC.
| n | Baseline | 3 months | 6 months | p | |
| All patients | 32 | 8.1±1.9 (n=32) | 7.1±1.5 (n=30) | 7.0±0.8 (n=23) | 0.016a/0.007b |
| T1DM on monitoring | 22 | 7.8±1.4 (n=22) | 7.6±1.5 (n=20) | 7.4±2.0 (n=17) | 0.142a/0.018b |
| Early T1DM | 3 | 11.3±1.2 (n=3) | 6.2±1.0 (n=3) | 6.2±0.7 (n=3) | 0.016a/0.014b |
| Diabetes and pregnancy | 7 | 6.3±0.3 (n=7) | 5.6±0.6 (n=7) | 5.7±0.7 (n=3) | 0.027a/0.246b |
T1DM: type 1 diabetes mellitus.
The data were coded, entered, and analyzed using statistical software SPSS version 12.0 for Windows. Descriptive analysis of qualitative variables was performed by calculating frequencies and percentages, while mean, standard deviation, median, and range were determined for quantitative variables. Differences between means were analyzed using Wilcoxon and Friedman tests for related samples. A value of p<0.05 was considered statistically significant.
ResultsUntil November 30, 2012, 32 patients with diabetes (27 patients with type 1 diabetes and 5 with gestational diabetes) entered telematic monitoring through the DiabeTIC web platform and underwent telematic monitoring for a mean time of 183.1±90.8 days. In parallel, patients attended scheduled visits to outpatient clinics, and only when requested by the patient and provided telematic monitoring was adequate, was the time between the scheduled visits prolonged. All patients (including women with gestational diabetes) were administered insulin at study start.
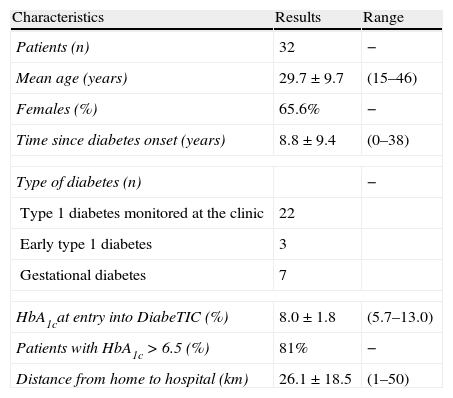
As shown in Table 1, most patients selected for this study were females (65%), young (mean age, 29.7±9.7 years), with inadequate metabolic control (mean HbA1c, 8.1±1.9%; 81% of patients with HbA1c>6.5%), and lived at some distance from the hospital, as they had to cover a mean of 52.2±37.0km to go to the hospital and return home. In the satisfaction survey (Table 2), high scores were obtained for most of the items analyzed, both those corresponding to the design of the DiabeTIC web site and to the telematic monitoring of diabetes.
Description of study population.
| Characteristics | Results | Range |
| Patients (n) | 32 | − |
| Mean age (years) | 29.7±9.7 | (15–46) |
| Females (%) | 65.6% | − |
| Time since diabetes onset (years) | 8.8±9.4 | (0–38) |
| Type of diabetes (n) | − | |
| Type 1 diabetes monitored at the clinic | 22 | |
| Early type 1 diabetes | 3 | |
| Gestational diabetes | 7 | |
| HbA1cat entry into DiabeTIC (%) | 8.0±1.8 | (5.7–13.0) |
| Patients with HbA1c>6.5 (%) | 81% | − |
| Distance from home to hospital (km) | 26.1±18.5 | (1–50) |
HbA1c: glycosylated hemoglobin; km: kilometers; n: number.
Results of the satisfaction survey performed at one month of monitoring.
| Question | Mean±SD | Rangea |
| My general impression of the platform is good | 8.6±1.8 | (4–10) |
| I think that the platform is easy to use | 8.1±1.5 | (5–10) |
| Navigation through the platform is intuitive | 6.7±3.0 | (1–10) |
| Allows me to adequately visualize the information | 8.2±1.8 | (4–10) |
| Data entry into the system is easy | 7.9±2.5 | (1–10) |
| Being able to consult my measurements through tables, graphs, and statistical summaries is useful for me | 9.1±1.1 | (7–10) |
| I think that my care is worse because there is no real contact with my doctor/nurse | 3.0±2.5 | (1–8) |
| Data entered into the platform are important for control of my diabetes | 9.5±0.9 | (7–10) |
| Knowing that a health care professional may continuously consult my measurements makes me feel more confident | 9.5±0.8 | (7–10) |
| I find it positive to be able to find information about diabetes in the library | 9.4±1.1 | (7–10) |
| I find it positive to be able to consult my doctor/nurse by sending messages | 9.1±1.4 | (5–10) |
| Use of the platform provides for more dynamic and motivating communication | 8.7±1.4 | (6–10) |
| I find it positive to have a 24-h telephone attention service for asking questions | 9.2±1.4 | (5–10) |
| Is worried about privacy of his/her data | 3.8±3.3 | (1–10) |
| Recommends the use of the platform to other patients | 9.4±0.9 | (7–10) |
SD: standard deviation.
In the study population, HbA1c levels significantly improved at three and six months of telematic monitoring (8.1±1.9 versus 7.1±1.5 versus 7.0±0.8%; p=0.016 as compared to the third month and p=0.007 as compared to six months of monitoring). Patients with gestational diabetes experienced a significant improvement in blood glucose control at three months of monitoring (5.6±0.6 versus 6.3±0.3%; p=0.027), but the improvement was not statistically significant at six months (5.7±0.7 versus 6.3±0.3%; p=0.246). However, only three patients were monitored for six months. Nine patients were discharged from DiabeTIC before completing six months of monitoring: two patients because they moved outside the province, three women due to end of pregnancy, and four patients because they voluntarily discontinued monitoring due to low or no use of the web platform.
DiscussionAlthough telemedicine has been used with more or less success in patients with diabetes for the past 30 years, most interventions used telephone, short message services (SMS), video conference, multi-access systems, or electronic mail.1,10,12 Although these technologies have been widely shown to be effective, efficient and easy to use,1,10–12 most of them have significant limitations as regards the visualization of blood glucose controls, the storage of information provided by patients, or the possibility of a real time change in treatment schemes, amongst others. Moreover, in patients with diabetes on insulin therapy, treatment decisions should be taken based on a wide range of information (not only capillary blood glucose levels, but also diet, insulin dose, exercise, etc.) which cannot always be obtained through these systems.2,18
Because of this, the current trend in telemedicine and diabetes is to develop “virtual spaces” of cooperative work that promote the shared care of patients and professionals and also allow for real time changes in insulin doses or act as a supervisor of adjustments in therapy performed by patients.13,19 In this regard, the DiabeTIC platform is a web site currently available for patients and professionals which provides the possibility of the remote monitoring of different variables, including weight, blood pressure, blood glucose, insulin dose, and carbohydrate servings. DiabeTIC also provides a remote message service allowing for two-directional communication between patients and professionals, as well as remote education through a virtual library which may contain educational materials of all kinds. In addition, both patients and professionals may modify insulin treatment in real time on this web site, so facilitating shared decision-making and the optimization of metabolic control.
The results of this pilot study conducted on a small sample of patients with type 1 and gestational diabetes show that, after six months of telematic monitoring, metabolic control significantly improved. Obviously, as the study design included no control group, we cannot conclude that improvements in HbA1c levels at six months by 1.1% (in the overall study population) and 0.4% (in the subgroup of patients with type 1 diabetes not pregnant or in an early disease stage) was the result of telematic monitoring, but we can at least infer that it did not impair these levels. The results are consistent with improvements in HbA1c levels ranging from 0.2% to 1.4%reported in other studies after 3–12 months of telematic monitoring.5,10,12,13,18–22 It should be noted, however, that other studies concluded that telemedicine has few effects on metabolic control and that the differences between telemedicine and conventional care were not significant, despite finding HbA1c decreases.23–25
It would be of interest to discuss the reasons that appear to promote improved metabolic control in patients on telematic monitoring. One potential factor is that diabetes is a chronic disease requiring continuous control and for which the traditional model based on “meetings” is inadequate as compared to more continuous monitoring such as may be provided through telemedicine systems.19 Another potential explanation may be that most patients with diabetes need a supervised autonomy that prevents them from taking inadequate decisions and allows, on the one hand, as much independence as possible, and on the other hand the assurance that the decisions taken by patients are validated, the possibility of which is maximized when real time changes are made in telematic treatments. In addition, in periods of poorer metabolic control (e.g. in early disease) and during pregnancy, adequate care for diabetes usually requires the continuous review of therapy, which is not always possible at a patient visit but which, however, may be relatively easy to do by telematic means. Finally, it seems logical to think that patients with diabetes on regular telematic monitoring show a greater involvement in the self-care of their disease as the result of regular supervision of their decision-making.19,26
The satisfaction survey showed that the diabetic patients participating in our telematic monitoring study were extremely satisfied with both the design of the DiabeTIC platform and with the telematic monitoring performed. It should be emphasized that the highest mean score was given for the item “Data entered into the platform are important for control of my diabetes” (mean score, 9.5±0.9; 88.9% of scores ≥8 points), which appears to support the idea that autonomy supervised through telematic monitoring is particularly valued by patients with diabetes.27 Similarly, in the AETSA review, eight of the 10 articles where patient satisfaction was assessed showed a high user satisfaction with these telematic monitoring systems.1
This study had some limitations, including assessment of a small, highly heterogeneous cohort of diabetic patients, lack of a control group, non-randomization of patients, and exclusion from the analysis of patients lost to follow-up. However, the study was not designed to assess the efficiency of telematic monitoring or to make a comparison with the traditional monitoring method, but to analyze whether telematic monitoring in a shared virtual space such as the DiabeTIC web platform is accepted and improves short-term metabolic control in a subgroup of patients with diabetes who may potentially benefit from this modality of care. We think that although the results of this study are consistent with current scientific evidence,1 longer studies are required to investigate the best way to implement this technology for monitoring patients with diabetes. In addition, this study did not analyze the potential relationship between the use of the system by patients (number of connections, level of access to educational pages, number of electronic mails, etc.) and its potential impact on glucose control, an aspect which should be assessed in subsequent research.
In conclusion, patients with diabetes monitored through DiabeTIC reported a high degree of satisfaction with both the web platform and with telematic monitoring of diabetes, and a favorable evolution in metabolic control was seen in the short term. It currently appears advisable to enhance the use of virtual spaces of cooperative work (such as web sites) that promote shared diabetes care between patients and professionals while allowing for real time changes in insulin doses or for the supervision of adjustments in therapy made by the patients themselves.
FundingThis study was partially funded by Laboratorios Sanofi. Florentino Carral has received fees for teaching activities from Abbott, Lilly, Novartis, Novonordisk, and Sanofi.
Conflicts of interest: The authors of this article state that they have no conflicts of interest with regard to the results of this study.
Please cite this article as: Carral San Laureano F, Ayala Ortega MC, Jiménez Millán AI, Piñero Zaldivar A, García Calzado C, Prieto Ferrón M, et al. Página web DiabeTIC: estudio piloto de la satisfacción e impacto sobre el control metabólico. Endocrinol Nutr. 2013;60:441–446.
