








The treatment of pilonidal sinus (PS) is usually surgical, but no procedure is considered the gold standard. The Karydakis (K) technique is widely used, and unroofing and marsupialization (UM) is a simple surgery with good results.
Primary objectiveTo evaluate early postoperative complications (EPC) 30 days after UM surgery compared to the K technique.
Secondary objectivesTo evaluate surgical time, postoperative pain, patient satisfaction, return to daily activity and early recurrence within 3 months.
MethodProspective, single-center, randomized study in patients who underwent surgery for primary PS with no abscess between June 2016 and November 2017. They were randomized using a computer-generated block method. To analyze the main objective, a non-inferiority analysis was performed.
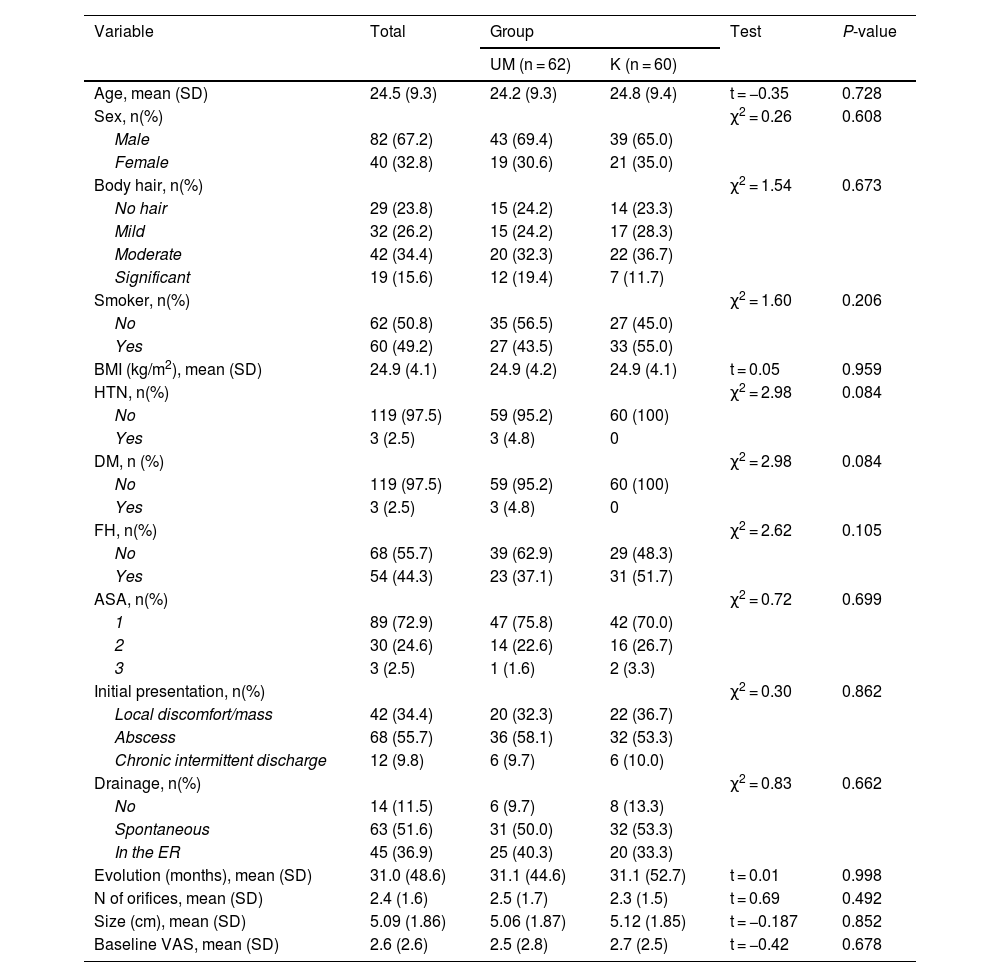
Results122 patients with symptomatic primary PS were randomized: 60 in the K group and 62 in the UM group. Both groups were homogeneous.
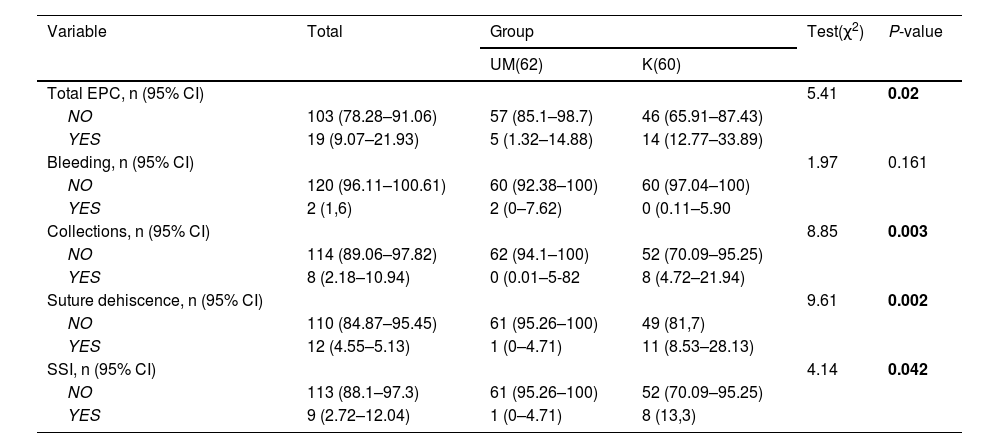
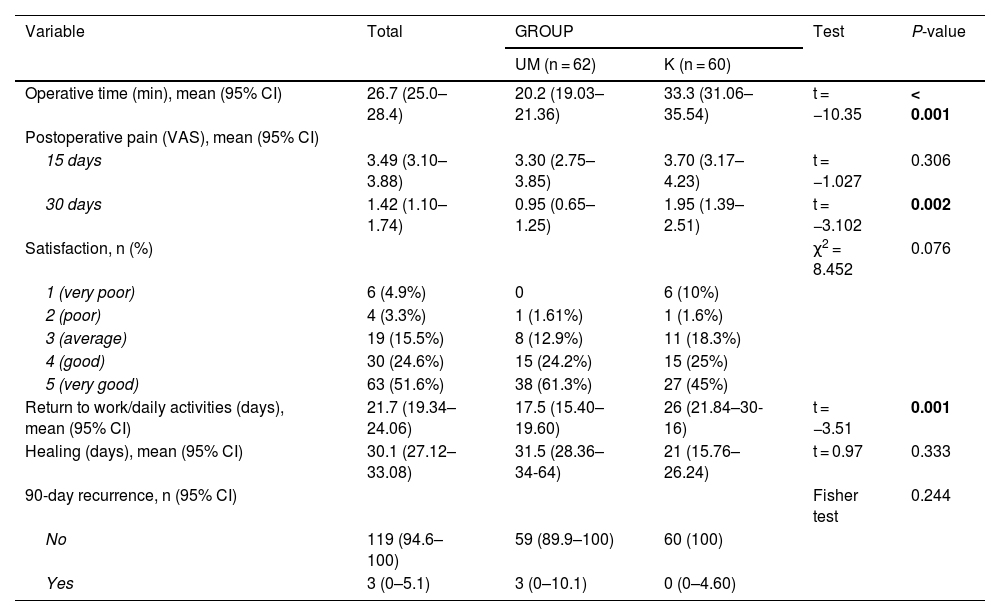
There were statistically significant differences between surgery and postoperative complications at 15 and 30 days in favor of UM. There were also differences in favor of UM in surgical time and return to daily activity. During the 90-day follow-up, there were 3 recurrences in the UM group and 0 in the K group.
ConclusionsUM is a simple, minimally invasive, easily reproducible technique that has a lower rate of early complications, with a shorter operative time and an earlier return to daily activity.
El tratamiento del sinus pilonidal (SP) es habitualmente quirúrgico, pero no existe un procedimiento considerado como “gold stándard”. La técnica de Karydakis (K) es ampliamente utilizada y la Puesta a Plano, Curetaje y Marsupialización de bordes (PPCYM) es una cirugía sencilla y con buenos resultados.
Objetivo primarioEvaluar las complicaciones postquirúrgicas precoces (CPP) a 30 días tras la cirugía de la PPCYM en comparación con la técnica K.
Objetivos secundariosEvaluar el tiempo quirúrgico, dolor postoperatorio, satisfacción del paciente, reincorporación a las tareas habituales y recidiva precoz a los 3 meses.
MétodosEstudio prospectivo, unicéntrico y aleatorizado en pacientes intervenidos de SP primario y sin absceso entre junio de 2016 y noviembre de 2017. Se aleatorizaron mediante un método de bloques balanceados generado por ordenador. Para analizar el objetivo principal se realizó un análisis de no inferioridad.
Resultados122 pacientes aleatorizados con SP primario sintomático: 60 en el grupo K y 62 en el grupo PPCYM. Ambos grupos fueron homogéneos.
Hubo diferencias significativas en las complicaciones postoperatorias a los 15 y 30 días a favor de PPCYM. También hubo diferencias a favor de PPCYM en el tiempo quirúrgico y la reincorporación a las tareas habituales. Durante el seguimiento a 90 días hubo 3 recidivas en el grupo PPCYM y 0 en el grupo K.
ConclusionesUM PPCYM es una técnica sencilla, mínimamente invasiva, fácilmente reproducible y que tiene una menor tasa de complicaciones precoces, con un menor tiempo quirúrgico y una reincorporación a las tareas habituales más precoz.

