



McArdle's disease (glycogen storage disease type V) is an energy-dependent disorder of skeletal muscle caused by a deficiency of myophosphorylase, an important enzyme of carbohydrate metabolism that converts glycogen to glucose-1-phosphate. A 46 year-old man was sent to the rheumatology outpatient department with a 3-year history of severe exercise-induced cramps and myalgias. The episodes began when he worked in France and used to practice ski and snowboard in the Alps Mountain, with exercise intolerance, muscle cramps, and myoglobinuria. The laboratory results showed elevated serum creatine kinase levels (∼15,000U/L), and the biopsy of the deltoid muscle revealed glycogen subsarcolemmal vacuoles and absence of myophosphorylase enzymatic activity. This clinical case emphasises the importance of taking into account this metabolic disorder when faced with a patient with exercise intolerance and cramps, especially after vigorous/anaerobic exercise and elevated levels of CK activity. It is fundamental to explain the aetiology of the patient symptoms in order to improve quality of life and avoid unnecessary complications.
La enfermedad de McArdle (enfermedad de almacenamiento de glucógeno tipoV) es un trastorno del músculo esquelético dependiente de la energía causado por una deficiencia de miofosforilasa, una importante enzima del metabolismo de los hidratos de carbono que convierte el glucógeno en glucosa-1-fosfato. Un hombre de 46años de edad fue enviado al departamento de reumatología para pacientes ambulatorios con un historial de 3años de calambres y mialgias severos inducidos por el ejercicio. Los episodios comenzaron cuando trabajó en Francia y solía practicar esquí y snowboard en el macizo de los Alpes, con intolerancia al ejercicio, calambres musculares y mioglobinuria. Las pruebas de laboratorio mostraron niveles elevados de creatina quinasa sérica (∼15.000U/l) y la biopsia del músculo deltoides reveló vacuolas subsarcolémicas de glucógeno y ausencia de actividad enzimática de la miofosforilasa. Nuestro caso clínico enfatiza la importancia de pensar en este trastorno metabólico cuando tenemos un paciente con intolerancia al ejercicio y calambres, especialmente después de un ejercicio vigoroso/anaeróbico y niveles elevados de actividad CK. Es fundamental explicar la etiología de los síntomas del paciente para mejorar la calidad de vida y evitar complicaciones innecesarias.
Glycogen storage disease type V is an energy-dependent disorder of skeletal muscle caused by a deficiency of myophosphorylase,1–3 an important enzyme of carbohydrate metabolism that converts glycogen to glucose-1-phosphate, first described by McArdle in 1951 in a 30 year old man with lifelong intolerance to exercise.1 Its deficiency is caused by autosomal recessive mutations in the myophosphorylase gene (PYGM) located on chromosome 11.3–5 Because the energy produced by glycolysis is reduced in patients with a deficiency of myophosphorylase, symptoms of exercise intolerance, muscle cramps and weakness usually predominate during short bursts of high-intensity exercise. Many patients experience a second wind, that is, when they rest after cramps first appear, they can continue exercise without further symptoms.2,6 Myoglobinuria, rhabdomyolysis and renal failure can also occur.1–3
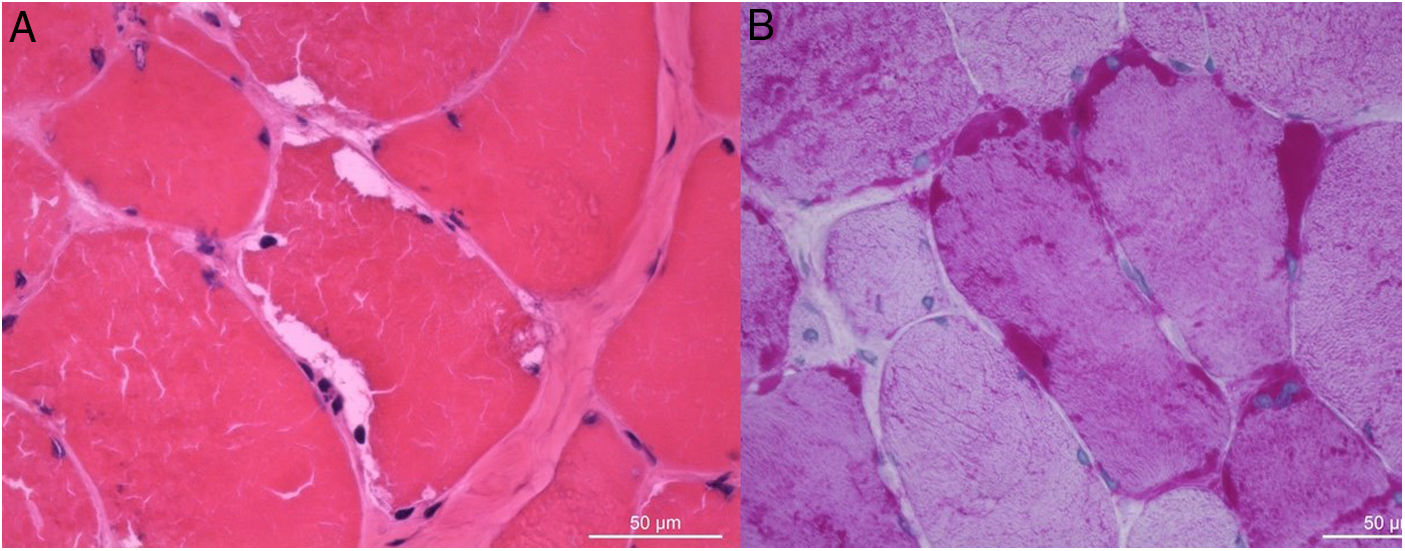
Clinical observationA 46 years-old man was sent to the rheumatology outpatient department with a 3-year history of severe exercise-induced cramps and myalgias. The episodes began when he worked in France and used to practice ski and snowboard in the Alpes Mountain. He described fatigue and the feeling of a slight loss of strength in his upper and lower limbs following strenuous exercise. He also complained of dark urine after these episodes, which may be suggestive of myoglobinuria. He had no past medical history or smoking habits and no known family history of cramps. At our observation muscle strength was preserved. The lab tests showed elevated serum creatine kinase (CK) levels ∼15,000U/L (10–172); aldolase 20.5U/L (<7.6) and myoglobin 489.6ng/mL (<146.9) and slightly increased liver enzymes. B-type natriuretic peptide (BNP) was in the normal range. At this time the urine sediment analysis was unremarkable. An echocardiogram showed preserved ventricular function and there was not electrocardiographic detection of acute myocardial ischaemia. An electromyogram revealed no evidence of myopathy but the biopsy of the deltoid muscle revealed the presence of subsarcolemmal vacuoles containing glycogen (periodic acid Schiff-positive) and absence of enzymatic activity of myophosphorylase (Fig. 1). Moreover, a genetic variant (deletion of 164–168) in homozygotic pattern in the exon 1 of the PYGM gene was detected. Therefore, the diagnosis of McArdle's disease was made and the patient was oriented to nutrition and metabolic diseases consultation and received proper diet and exercise advices. At 12 months follow-up, he had no further complaints of myalgias or cramps, remaining asymptomatic and with a good quality of life.
Discussion. (A) H&E, (B) PAS, scale bar: 50μm.")
Myophosphorylase deficiency makes it impossible to obtain energy from the glycogen stores in muscle. Usually the symptoms manifest during adolescence or early adulthood. Rarely, it may appear for the first time in older patients, mainly after strenuous exercise, such as in this case report. The characteristic laboratory findings are elevated CK levels and the electromyography can either be normal or show evidence of myopathy.2 The definitive diagnosis is based on muscle biopsy through the observation of the absence of myophosphorylase by histoenzymological analysis. The histological findings are characterized by the presence of subsarcolemmal vacuoles containing glycogen, which can be examined using periodic acid Schiff staining.2,3 Although there is no specific treatment for this disease at the present time, it is possible to improve the quality of life of the patients and prevent rhabdomyolysis and renal failure with proper diet and by controlling physical activity.2,6,8 The diet should be rich in carbohydrates an low in fat and patients must be advised to consume foods containing simple carbohydrates 5min before exercising.2,7
ConclusionOur clinical case emphasizes the importance of thinking about this metabolic disorder when we have a patient with exercise intolerance and cramps, especially after vigorous/anaerobic exercise and elevated levels of CK activity. It's fundamental to explain the aetiology of the patient's symptoms in order to improve quality of life and avoid unnecessary complications.
Conflict of interestsThe authors declare that there is no conflict of interests.
