



Define the modes of procedure of the Deductive Care Methodology (DCM) in the generation of knowledge about person's health care.
MethodologyDesign and test of the DCM modes based on three phases: mapping of the DCM, generation of models from this methodology and testing of the models through studies in a clinical context.
ResultsThe DCM presents five levels of abstraction with three modes broken down to 16 types. The modes are: Philosophical Mode to conceptualize and obtain generalities about reality, Mathematical Mode to operate with generalities, and Physical Mode to operationally verify, validating the results and the predictive capacity of the model. This MDC allows the creation of three models: Knowledge Model about Person Care, an ontology of care, Vulnerability Model about the person and Taxonomic Triangulation Model for knowledge management. All models generate products for computational knowledge management. In addition, the models are applied in teaching and generate research with more than a hundred participations in conferences and journals, of which five impact publications (from 2008 to 2022) classified in the categories of Nursing and Informatics are analysed.
ConclusionsThe DCM collects prior knowledge to work with certainties, evidence and applying inferences that do not depend on the number of cases or inductive designs. This research presents a formal structure of the DCM with an interdisciplinary orientation between Health Sciences and Computer Sciences.
Definir los modos de procedimiento de la Metodología Deductiva del Cuidado (MDC) en la generación de conocimiento acerca del cuidado de la salud de las personas.
MetodologíaDiseño y prueba de los modos de la MDC basado en tres fases: mapeado de la MDC, generación de modelos desde esta metodología y prueba de los modelos a través de estudios en contexto clínico.
ResultadosLa MDC presenta cinco niveles de abstracción con tres modos desglosados hasta 16 tipos. Los modos son: Modo Filosófico para conceptualizar y obtener generalidades acerca de la realidad, Modo Matemático para operar con las generalidades y Modo Físico para verificar operacionalmente, validando los resultados y la capacidad predictiva del modelo. Esta MDC permite crear tres modelos: Modelo de Conocimiento sobre el Cuidado de la Persona, una ontología de cuidado, Modelo de Vulnerabilidad sobre la persona y Modelo de Triangulación Taxonómica para gestión de conocimiento. Todos los modelos generan productos para gestión computacional del conocimiento. Además, los modelos se aplican en docencia y generan investigaciones con más de un centenar de participaciones en congresos y revistas, de las cuales se analizan cinco publicaciones de impacto (desde 2008 a 2022) clasificadas en las categorías de Enfermería e Informática.
ConclusionesLa MDC recoge conocimiento previo para trabajar con certezas, evidencias y aplicando inferencias que no dependen del número de casos o diseños inductivos. Esta investigación presenta una estructura formal de la MDC con orientación interdisciplinar entre Ciencias de la Salud y Ciencias de la Computación.
Deductive care methodology (DCM) appears in books on nursing models and theories, but it has not been developed or explained, and is scarcely acknowledged in the scientific literature.
What it contributes?The study provides the first detailed description of the CDM and the different ways of proceeding that can be used by other research. It allows hypotheses to be generated and tested, phenomena to be predicted, and various disciplines to be connected in healthcare research.
Interdisciplinarity between Health Sciences and Computer Science has progressed in recent decades to become a cornerstone for solving problems of all kinds: from predictions regarding the evolution of the COVID-19 pandemic to challenges related to the impact of Artificial Intelligence on human life.1
Research in this area calls for perspectives and methodologies that creatively emerge from the combination of both branches of knowledge. Current projects and publications encompass research, such as building and evaluating healthcare technologies, modelling for big data analysis, or designing games with the aim of acquiring competencies in care. These methodologies go beyond the traditional classifications in Health Sciences that differentiate between inductive-deductive-retroductive methods and quantitative-qualitative analysis, or a combination of them. Such strategies have not been found in published references to sustain them with evidence.2,3
In this respect, research on human healthcare faces two challenges. First, the object of study is an abstract construct in its concept and one that can be measured in a variety of ways in its expression as a phenomenon. Care is thought and action about sustaining life by ensuring that a set of needs are met by means of responses that create and establish life habits. Health is a dynamic situation of relationship between need and competence in people's life path that is both the result of past care and a vital resource for projecting the future. Second, publications in this area of healthcare have followed the ideal of scientific method in applied sciences that address phenomena of reality (care as acts and health as states) through inductive studies that compile and analyse specific data so as to draw a more general conclusion. However, these studies offer new knowledge in terms of probability depending on their design and sample. In contrast, deduction has traditionally been associated with the so-called pure (or exact) sciences, such as mathematics, physics, or chemistry, in which general premises are used to infer particular conclusions in terms of truth and validity.4–6
A way of generating knowledge, deduction, which has been recognised in the creation of models and theories of care, but which is seldom made explicit in the publications of impact journals and, when it is, it is not clearly defined and is limited to the use of a prior model (from any discipline and level of abstraction) or to content analysis strategies.4,5,7,8
Against this background, the MISKC Group (Management about Information and Standard Knowledge of Care) of the University of Alcalá (Madrid) and the Sorge Academy investigates how knowledge about human health care is managed and proposes the Deductive Methodology of Care (DMC) as the approach to acquire and, potentially, implement knowledge about human care through deduction.9
The deductive perspective is derived from general or universal (axioms, laws, propositions…) to individualise knowledge and understanding of reality or, at least what is known about it. Thus, the act of understanding entails, not only understanding or describing reality, but responding to the why, what, and how in order to explain and predict facts. There are three concepts that for this purpose of understanding an area of knowledge are key to the management of knowledge and, specifically, to management from a deductive methodology. The three concepts are: ideal, as a perfect model that serves as a reference or archetype, true, because things conform to the concept that is formed in the mind or that proposition that cannot be rationally denied, and, finally, falsehood or the lack of agreement between words, ideas, and things.5,10,11
Understanding modes as the ways of proceeding, the procedure or set of procedures into which the deductive methodology perspective can be divided, the general aim of this work is to define the procedural modes of DCM in generating knowledge about people's health care.
The specific objectives comprise:
- -
To describe the modes of DCM.
- -
To apply the modes of DCM in generating models.
- -
To test the models in a clinical context.
The study followed a create-and-test a methodology design; that is to say, the main result is DCM mapping that includes different modes and subtypes. A DCM that is to be tested as a knowledge generator. Therefore, once the DCM has been mapped, models of knowledge that have used this kind of deductive methodology will be presented and, subsequently, the published research studies that stem from these models and that demonstrate the impact on generating knowledge regarding care will, likewise, be presented.
Thus, the research procedure was conducted in three phases:
- 1
Mapping the DCM
The modes were described applying a multidisciplinary knowledge extraction strategy from Health Sciences, Philosophy, and Mathematics. The knowledge generation strategies from these disciplines were combined to determine common elements, definitions, and relationships of the DCM, which were ordered constituting a structure of levels for this deductive methodology.
- 2
Generating models
DCM was used to create models of knowledge in the interdisciplinary are of Health Sciences and Computational Sciences: an ontology of care (disciplinary object), a model of person (subject), and a model of knowledge management (method and language).
The three models share a purpose or framework: managing knowledge about healthcare in computational systems; care of the person being the object interest, and its focus is on application-oriented information systems.
Each model applies different types of DCM from the premises of the metaparadigm and theories of Nursing. Thus, every model should include the definition of concepts, relationships, and ways of operating knowledge.
- 3
Application in clinical studies
The models were tested to demonstrate their explanatory and predictive usefulness. Academic training and postgraduate research based on these models generated more than a hundred contributions to national and international conferences and journals, of which those that meet the criteria of making the model explicit in its conceptual basis and being endorsed by a high impact publication (publications included in the Journal Citation Reports) that implies blind peer review with international experts are selected as a study sample.
The applications are summarised as follows:
- -
Ontological model:
- -
Person model:
- o
The Care Vulnerability Index (CVi) tool applied to the Colombian population. The questionnaire consists of 12 items arranged in five clusters. The variables were the Basic Care Variables (BCV): stage of life, developmental status, gender, cultural integration, family support, individual care, limitations (mobility, cognition, sensory), surroundings, availability of time and resources.
- o
- -
Knowledge management model:
- o
Taxonomic Triangulation Technique applied in two contexts: nursing protocols of the Madrid Health Service (SERMAS, for its acronym in Spanish) and the World Health Organisation's (WHO) COVID-19 clinical guidelines.15 The sample for analysis are the documents, the data collected through knowledge extraction, and the variables formalised in Nursing Outcomes Classification (NOC) and Nursing Interventions Classification (NIC) languages to represent the care process and identify the underlying NANDA-I diagnoses through triangulation.12–14
- o
The DCM is part of a Doctoral Thesis in Health Sciences at the University of Alcalá, forming part of the research lines of the MISKC Group and its project having been approved by the corresponding Commission, in keeping with the current regulations on research and data processing (Declaration of Helsinki, Royal Decree 1090/2015, Law 14/2007, Law 41/2002). The design does not involve a population sample and, as such, does not require informed consent or [approval by] an ethics committee for research with individuals.
With respect to the doctoral theses and clinical studies, each one has its own particular methodological and ethical characteristics, which the reader can consult in the corresponding references. In summary, the designs consist largely of text analyses and expert consensus. The only study with a population sample is the vulnerability study in Colombia and this line of research has the approval of the Eastern Assistance Directorate of the Madrid Primary Care Management (SERMAS, Spain) and the University of Cartagena (Colombia).
In any case, experts and participants were always informed both verbally and in writing about the corresponding study, their voluntary participation, the anonymous and confidential treatment of their data.
Moreover, the studies received the approval of the Epistemology and Bioethics Commission de la Madrid Scientific Society of Care (Sociedad Científica Madrileña del Cuidado, SoCMaC) and the endorsement of the Madrid Official College of Nursing (Colegio Oficial de Enfermería de Madrid, CODEM).
Data processing involved using researchers to gather the data who were not already involved in analysing the anonymised data. The lead researcher of each study is responsible for the safekeeping and custody of the data obtained.
ResultsThe results by specific objectives are:
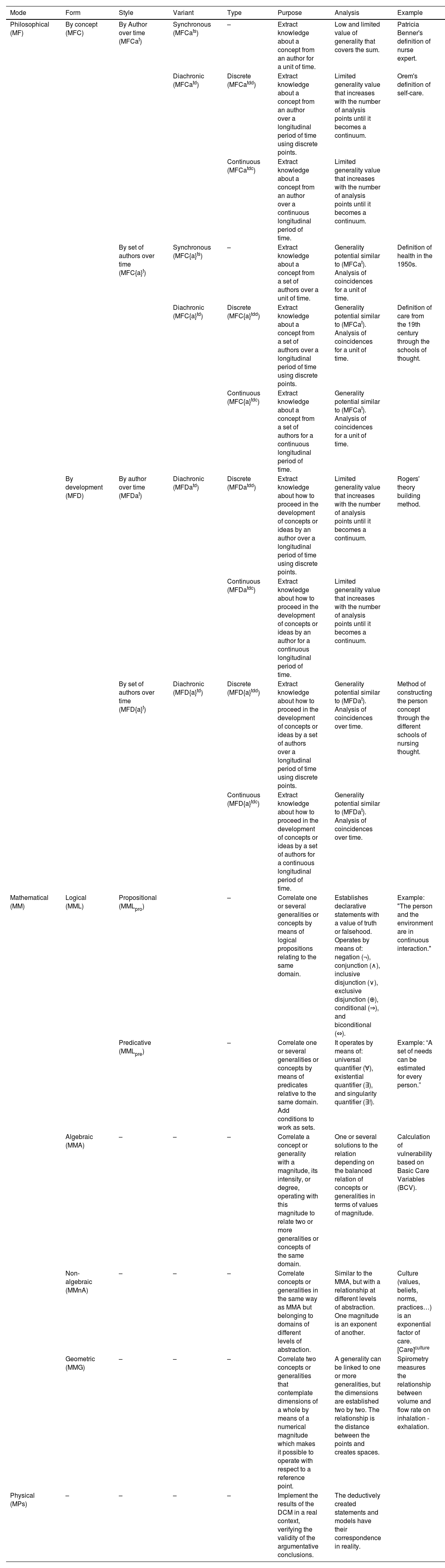
Mapping the DCMThe DCM is organised into five levels, from greater to smaller: Mode (procedure or set of procedures), Form (the way or manner in which the thing is performed or occurs, of being organised), Style (form of behaviour, of doing the thing), Variant (variety or difference between different forms or styles of the same thing), and Type (characteristic model between the different forms, styles, or variants of the thing).
All told, the DCM has three modes that are broken down into 16 types:
Philosophical mode (MF)This mode enables us to obtain generalities about reality, or the knowledge we have of it, by studying the works of other authors on a given area of knowledge. Unlike knowledge extraction, this mode entails a reference paradigm to analyse the sources. It has two forms: concept (MFC), aimed at generality and its structure of relations, or development (MFD), focused on understanding how to proceed in the development of these concepts and relations. The latter mode always requires several time points of analysis.
Mathematical mode (MM)The MM allows us to operate with generalities about reality, or about the knowledge we have of it, using the reasons of Mathematics. The MM can range from classical propositional logic to the most complex geometry.
Physical mode (MPs)This enables an operational verification of the generality or model, validating the respective results and making it possible to make predictions that demonstrate the validity of the model.
The DCM mapping appears in Table 1.
DCM mapping.
| Mode | Form | Style | Variant | Type | Purpose | Analysis | Example |
|---|---|---|---|---|---|---|---|
| Philosophical (MF) | By concept (MFC) | By Author over time (MFCat) | Synchronous (MFCats) | – | Extract knowledge about a concept from an author for a unit of time. | Low and limited value of generality that covers the sum. | Patricia Benner's definition of nurse expert. |
| Diachronic (MFCatd) | Discrete (MFCatdd) | Extract knowledge about a concept from an author over a longitudinal period of time using discrete points. | Limited generality value that increases with the number of analysis points until it becomes a continuum. | Orem's definition of self-care. | |||
| Continuous (MFCatdc) | Extract knowledge about a concept from an author over a continuous longitudinal period of time. | Limited generality value that increases with the number of analysis points until it becomes a continuum. | |||||
| By set of authors over time (MFC{a}t) | Synchronous (MFC{a}ts) | – | Extract knowledge about a concept from a set of authors over a unit of time. | Generality potential similar to (MFCat). Analysis of coincidences for a unit of time. | Definition of health in the 1950s. | ||
| Diachronic (MFC{a}td) | Discrete (MFC{a}tdd) | Extract knowledge about a concept from a set of authors over a longitudinal period of time using discrete points. | Generality potential similar to (MFCat). Analysis of coincidences for a unit of time. | Definition of care from the 19th century through the schools of thought. | |||
| Continuous (MFC{a}tdc) | Extract knowledge about a concept from a set of authors for a continuous longitudinal period of time. | Generality potential similar to (MFCat). Analysis of coincidences for a unit of time. | |||||
| By development (MFD) | By author over time (MFDat) | Diachronic (MFDatd) | Discrete (MFDatdd) | Extract knowledge about how to proceed in the development of concepts or ideas by an author over a longitudinal period of time using discrete points. | Limited generality value that increases with the number of analysis points until it becomes a continuum. | Rogers' theory building method. | |
| Continuous (MFDatdc) | Extract knowledge about how to proceed in the development of concepts or ideas by an author for a continuous longitudinal period of time. | Limited generality value that increases with the number of analysis points until it becomes a continuum. | |||||
| By set of authors over time (MFD{a}t) | Diachronic (MFD{a}td) | Discrete (MFD{a}tdd) | Extract knowledge about how to proceed in the development of concepts or ideas by a set of authors over a longitudinal period of time using discrete points. | Generality potential similar to (MFDat). Analysis of coincidences over time. | Method of constructing the person concept through the different schools of nursing thought. | ||
| Continuous (MFD{a}tdc) | Extract knowledge about how to proceed in the development of concepts or ideas by a set of authors for a continuous longitudinal period of time. | Generality potential similar to (MFDat). Analysis of coincidences over time. | |||||
| Mathematical (MM) | Logical (MML) | Propositional (MMLpro) | – | Correlate one or several generalities or concepts by means of logical propositions relating to the same domain. | Establishes declarative statements with a value of truth or falsehood. Operates by means of: negation (¬), conjunction (∧), inclusive disjunction (∨), exclusive disjunction (⊕), conditional (⇒), and biconditional (⇔). | Example: "The person and the environment are in continuous interaction." | |
| Predicative (MMLpre) | – | Correlate one or several generalities or concepts by means of predicates relative to the same domain. Add conditions to work as sets. | It operates by means of: universal quantifier (∀), existential quantifier (∃), and singularity quantifier (∃!). | Example: “A set of needs can be estimated for every person.” | |||
| Algebraic (MMA) | – | – | – | Correlate a concept or generality with a magnitude, its intensity, or degree, operating with this magnitude to relate two or more generalities or concepts of the same domain. | One or several solutions to the relation depending on the balanced relation of concepts or generalities in terms of values of magnitude. | Calculation of vulnerability based on Basic Care Variables (BCV). | |
| Non-algebraic (MMnA) | – | – | – | Correlate concepts or generalities in the same way as MMA but belonging to domains of different levels of abstraction. | Similar to the MMA, but with a relationship at different levels of abstraction. One magnitude is an exponent of another. | Culture (values, beliefs, norms, practices…) is an exponential factor of care. [Care]culture | |
| Geometric (MMG) | – | – | – | Correlate two concepts or generalities that contemplate dimensions of a whole by means of a numerical magnitude which makes it possible to operate with respect to a reference point. | A generality can be linked to one or more generalities, but the dimensions are established two by two. The relationship is the distance between the points and creates spaces. | Spirometry measures the relationship between volume and flow rate on inhalation - exhalation. | |
| Physical (MPs) | – | – | – | – | Implement the results of the DCM in a real context, verifying the validity of the argumentative conclusions. | The deductively created statements and models have their correspondence in reality. |
MF: Philosophical mode. MFC: Philosophical mode of concept; includes: 1. MFCat Philosophical mode by an author's concept over time; MFCats Philosophical mode by an author's concept in synchronous time (in a section as a unit of time); MFCatd Philosophical mode of an author's concept over a period of time or diachronic: discrete or with several cut-off points. (MFCatdd) or continuous (MFCatdc), and 2. MFC{a}t Philosophical mode of concept of a set of authors over time; MFC{a}ts Philosophical mode of concept of a set of authors in synchronous time (in a section as a unit of time); MFC{a}td Philosophical mode of concept of a set of authors over a period of time or diachronic: discrete or with several cut offs (MFC{a}tdd) or continuous (MFC{a}tdc). MFD: Philosophical mode of development; includes: 1. MFDat Philosophical mode of development of an author over time; MFDatd Philosophical mode of development of an author over a period of time or diachronic: discrete or with several cut offs (MFDatdd) or continuous (MFDatdc), and 2. MFD{a}t Philosophical mode of development of a set of authors over time; MFD{a}ts Philosophical mode of development of a set of authors in synchronous time (in a section as a unit of time); MFD{a}td Philosophical mode of development of a set of authors over a period of time or diachronic: discrete or with several cut offs (MFD{a}tdd) or continuous (MFD{a}tdc).
MM: Mathematical mode. MML: Logical mathematical mode; includes: MMLpro Mathematical mode of propositional logic and MMLpre Mathematical mode of predicative logic. MMA: Algebraic mathematical mode. MMnA: Non-algebraic mathematical mode. MMG: Geometric mathematical mode.
MPs: Physical mode.
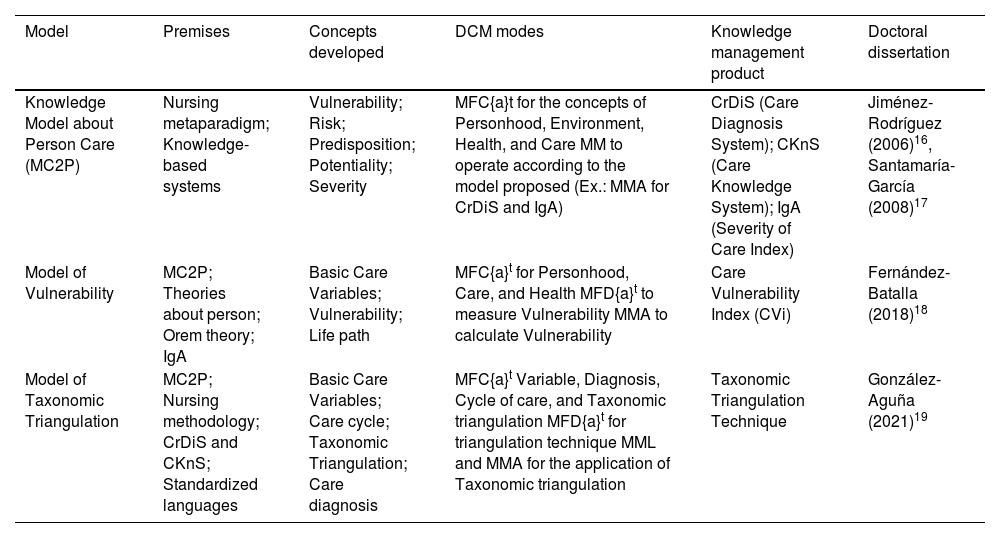
Using DCM, three models are created that are summarised in Table 2.
Care models created using DCM.
| Model | Premises | Concepts developed | DCM modes | Knowledge management product | Doctoral dissertation |
|---|---|---|---|---|---|
| Knowledge Model about Person Care (MC2P) | Nursing metaparadigm; Knowledge-based systems | Vulnerability; Risk; Predisposition; Potentiality; Severity | MFC{a}t for the concepts of Personhood, Environment, Health, and Care MM to operate according to the model proposed (Ex.: MMA for CrDiS and IgA) | CrDiS (Care Diagnosis System); CKnS (Care Knowledge System); IgA (Severity of Care Index) | Jiménez-Rodríguez (2006)16, Santamaría-García (2008)17 |
| Model of Vulnerability | MC2P; Theories about person; Orem theory; IgA | Basic Care Variables; Vulnerability; Life path | MFC{a}t for Personhood, Care, and Health MFD{a}t to measure Vulnerability MMA to calculate Vulnerability | Care Vulnerability Index (CVi) | Fernández-Batalla (2018)18 |
| Model of Taxonomic Triangulation | MC2P; Nursing methodology; CrDiS and CKnS; Standardized languages | Basic Care Variables; Care cycle; Taxonomic Triangulation; Care diagnosis | MFC{a}t Variable, Diagnosis, Cycle of care, and Taxonomic triangulation MFD{a}t for triangulation technique MML and MMA for the application of Taxonomic triangulation | Taxonomic Triangulation Technique | González-Aguña (2021)19 |
DCM: Deductive Care Model; MC2P: Knowledge Model about Person Care or Modelo de Conocimiento sobre el Cuidado de la Persona; CrDiS: Care Knowledge System or Sistema para el Diagnóstico del Cuidado in Spanish; CKnS: Care Knowledge System or Sistema para el Conocimiento del Cuidado in Spanish; IgA: Severity of Care Index or Índice de Gravosidad Asistencial; CVi: Care Vulnerability Index or Índice de Vulnerabilidad en Cuidados in Spanish.
Ontological model of person-centred care. Care is continuous and ever present in people, regardless of whether they are professionally cared for. The person is constructed from care and is defined by their vulnerability as an essential and dynamic condition of the relationship between need and competence throughout life. The setting (referred to as environment in the Nursing metaparadigm) is that which surrounds the person and interacts as open and complex systems that determine risk. The combination of vulnerability and risk establishes predisposition. This predisposition, depending on the existence of care limitations (knowledge, skill, or motivation), generates the potential to suffer problems, the severity of which will be either subclinical or clinical with symptomatology.
Vulnerability modelModel of the person as a vulnerable being in the life cycle continuum. Vulnerability is the expression between the need and competence of care that makes it possible to describe life pathways. The determination and representation of vulnerability is achieved through the Basic Care Variables as essential and sufficient information to express the continuum of care: how care has been provided and, from there, what its possible future trajectories are. The BCVs are: stage of life, developmental status, gender limitation, cultural integration, family support, individual care, limitation (mobility, cognitive, sensory), environmental factors, availability of time and resources. Vulnerability is calculated as the sum of the scores given for each variable, with 0 being the lowest score for vulnerability and 15 the highest.
Taxonomic Triangulation modelThis knowledge management model is based on the nursing care process, standardised nursing languages, and mathematical principles for inferences implicit in triangulation as a data management technique. Taxonomic triangulation allows knowledge to be acquired by analysing texts with reference to the MC2P and the process of care as a cycle of care. This model serves to make knowledge about care explicit and, primarily, to identify nursing diagnoses from data relating to three points of reference: assessment, outcomes, and intervention. This technique minimises possible errors when inferring in the opposite direction to the logical order established in the nursing process; that is, when seeking to deduce the diagnostic premise from the planned outcomes and interventions. The model can be applied manually or computationally in an Expert System.
Testing in a clinical contextThe three models were developed and tested more than a decade ago at the university level, with four doctoral dissertations in the programs of Health Sciences and Computational Sciences, and at the clinical level, by means of studies to create computer tools and validation in actual clinical situations, such as the validation of the Vulnerability index calculation tool in the Colombian population or the validation of the Taxonomic Triangulation tool in the actual situation of pandemic when there was no evidence available with respect to care.16–19
Among the hundred or so communications in international congresses and journals, five articles have been selected that meet the criteria of making the model explicit and having been published in a high impact journal. These publications cover the following Web of Science categories: “Nursing”, “Medical Informatics,” and “Computer science, interdisciplinary applications.”20
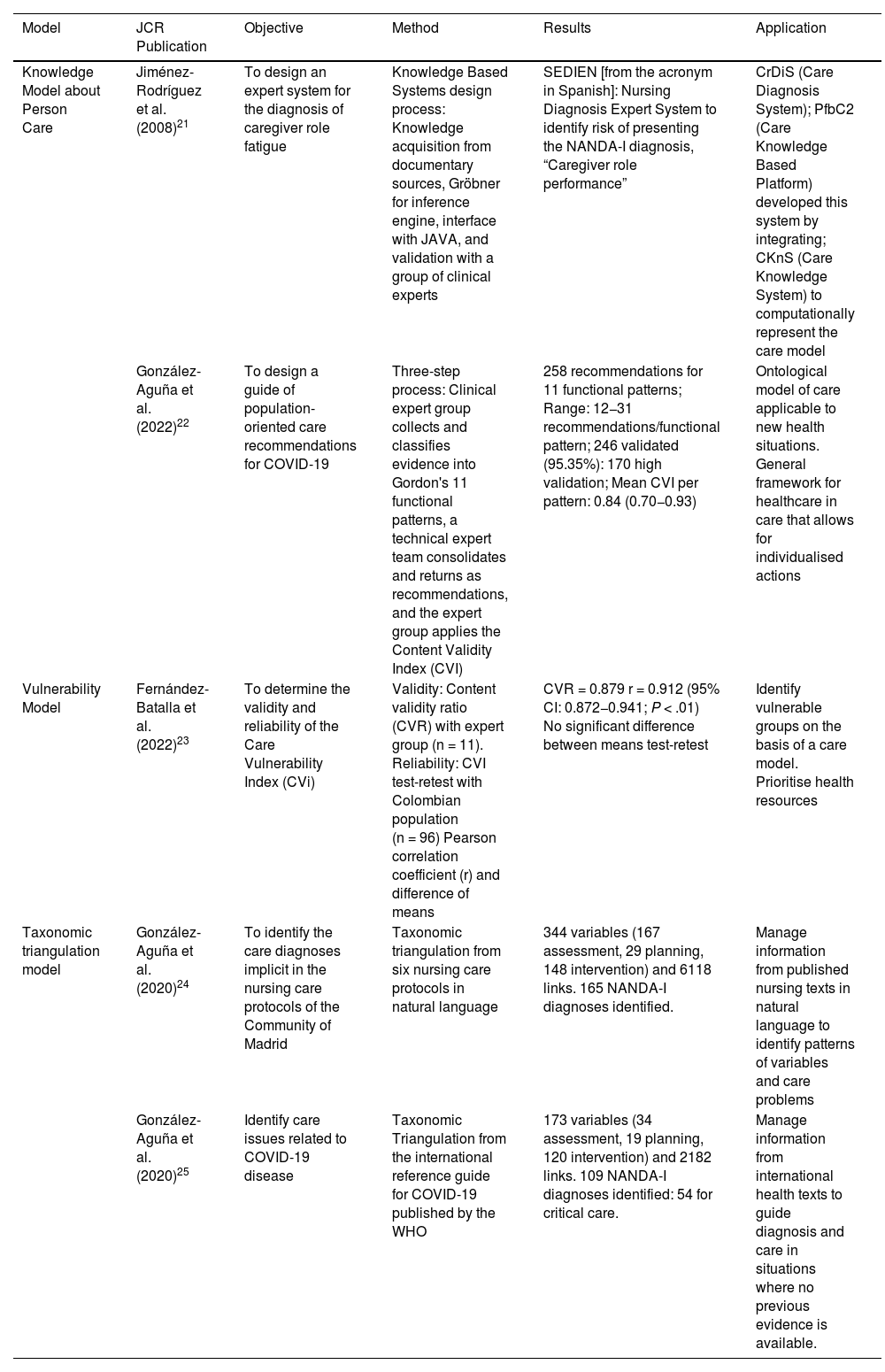
The main characteristics of these studies are summarised in Table 3.
Characteristics and evidence of DCM-based models.
| Model | JCR Publication | Objective | Method | Results | Application |
|---|---|---|---|---|---|
| Knowledge Model about Person Care | Jiménez-Rodríguez et al. (2008)21 | To design an expert system for the diagnosis of caregiver role fatigue | Knowledge Based Systems design process: Knowledge acquisition from documentary sources, Gröbner for inference engine, interface with JAVA, and validation with a group of clinical experts | SEDIEN [from the acronym in Spanish]: Nursing Diagnosis Expert System to identify risk of presenting the NANDA-I diagnosis, “Caregiver role performance” | CrDiS (Care Diagnosis System); PfbC2 (Care Knowledge Based Platform) developed this system by integrating; CKnS (Care Knowledge System) to computationally represent the care model |
| González-Aguña et al. (2022)22 | To design a guide of population-oriented care recommendations for COVID-19 | Three-step process: Clinical expert group collects and classifies evidence into Gordon's 11 functional patterns, a technical expert team consolidates and returns as recommendations, and the expert group applies the Content Validity Index (CVI) | 258 recommendations for 11 functional patterns; Range: 12−31 recommendations/functional pattern; 246 validated (95.35%): 170 high validation; Mean CVI per pattern: 0.84 (0.70−0.93) | Ontological model of care applicable to new health situations. General framework for healthcare in care that allows for individualised actions | |
| Vulnerability Model | Fernández-Batalla et al. (2022)23 | To determine the validity and reliability of the Care Vulnerability Index (CVi) | Validity: Content validity ratio (CVR) with expert group (n = 11). Reliability: CVI test-retest with Colombian population (n = 96) Pearson correlation coefficient (r) and difference of means | CVR = 0.879 r = 0.912 (95% CI: 0.872−0.941; P < .01) No significant difference between means test-retest | Identify vulnerable groups on the basis of a care model. Prioritise health resources |
| Taxonomic triangulation model | González-Aguña et al. (2020)24 | To identify the care diagnoses implicit in the nursing care protocols of the Community of Madrid | Taxonomic triangulation from six nursing care protocols in natural language | 344 variables (167 assessment, 29 planning, 148 intervention) and 6118 links. 165 NANDA-I diagnoses identified. | Manage information from published nursing texts in natural language to identify patterns of variables and care problems |
| González-Aguña et al. (2020)25 | Identify care issues related to COVID-19 disease | Taxonomic Triangulation from the international reference guide for COVID-19 published by the WHO | 173 variables (34 assessment, 19 planning, 120 intervention) and 2182 links. 109 NANDA-I diagnoses identified: 54 for critical care. | Manage information from international health texts to guide diagnosis and care in situations where no previous evidence is available. |
NOTE: The diagnosis “Caregive role strain” with code 00061, corresponds to the diagnosis of "Caregive role tension" in the latest 2021–2023 version.
JCR: Journal Citation Reports; CrDiS: Caring Knowledge System o Sistema para el Diagnóstico del Cuidado in Spanish; CKnS: Caring Knowledge System o Sistema para el Conocimiento del Cuidado in Spanish; CVi: Care Vulnerability Index o Índice de Vulnerabilidad en Cuidados in Spanish; CVR: Content Validity Ratio o Razón de Validez de Contenido in Spanish; CVI: Content Validity Index o Índice de Validación de Contenido in Spanish
Although deduction is recognised as a basic methodology with which to develop the epistemology of care, its study and description has not achieved the same level of detail as induction.5,26,27 While inductive [methodologies] are recognised and required in the standards of most impact publications, other designs do not qualify as accepted methodologies, are not associated with levels of evidence, and do not meet the guidelines to report research.28 This difference at the outset hinders the publication of research that apply a deductive methodology and, therefore, makes it difficult to strengthen the evidence for such designs.
However, deduction makes theoretical description and explanation of reality possible, as well as allowing hypotheses to be generated that will be evaluated with empirical data. Some nurses propose theories from nursing models or from other disciplines with a vision of care.5 Nevertheless, despite the role of deduction in building disciplinary knowledge, the publications reduce this methodology to referencing previous models or, often, linking it to the technique of content analysis that identifies and categorises concepts.7,8
Likewise, the analysis of any text (whether models or other types of documents that collect knowledge about care) is only one part of the possible forms of DCM.
MF covers this content analysis through those sub-types where the works of a set of authors are collected, either conceptually or developmentally, and either synchronically or diachronically. Similar to content analysis, MF provides for theoretical issues to be tested, data to be categorised according to previous models, replicable inferences to be made, facts to be represented, and new ideas to be obtained, as well as adding other utilities such as the analysis of conceptual development itself.27 In relation to this MF, a recent narrative review of data analysis and presentation was found in 151 integrative reviews and its results revealed that only 13 used deductive methods because their design involved the development of themes and categories according to an earlier criterion.8 The designs applied two pathways: turning objectives or questions into themes to classify concepts or using domains and concepts previously defined in other research or models.8 These analyses can provide reliable and revealing findings, but no pragmatic description of how to go about the process is found despite some attempts.7 Furthermore, the articles generally apply deduction with reference to a single model (with little explanation of their choice and form of analysis) or as part of a mixed induction-deduction methodology with expert groups as a source of information.
Regarding developmental MF, there are no publications with the object of study in the process of constructing concepts and relationships itself. Deductive methodology applies models as the final product, but does not delve into how they arrived at these models or replicate valid inferences. Thus, publications dealing with methodologies are associated with the translation and validation of instruments such as scales as opposed to studies on how to construct methodologies. This is even less the case in interdisciplinary fields, where each branch of knowledge has different perspectives and research designs.
On the other hand, the MM is a response to this lack of procedural description. MM goes beyond the creation of a knowledge structure (of concepts and their development) and addresses how to operate on the basis of deductive inference. The most widely recognised form is logic (a blend of philosophy and mathematics), but there are also other, more advanced forms that involve elements of different levels of abstraction. A necessary perspective in the creation of health technologies, such as diagnostic aid systems, that not only look for similar patterns, but require techniques that analyse complex and non-linear relationships, just as an expert would do.29
MPs test inferred knowledge, assuming the generalities and operations elaborated to test their explanatory and predictive potential to be true. This purpose has the three models outlined in the results because they illustrate the potential of DCM from the highest level of abstraction, with the ontology of MC2P, the development of explanatory models about the person, from information about vulnerability, and the capacity to manage knowledge about care focused on computational systems, from triangulation.
This knowledge helps the nursing discipline and other Health Science disciplines to improve their understanding of the care of the person (any care) and to predict the different individual, family, and social pathways. Beyond results in inductive terms of probability, this nursing research drives a Science of Care with axiomatic foundations and common theoretical premises on what is crucial to people's health care, to enable knowledge to be managed and evidence of the paradigm to be established.
The main limitation of this research are, on the one hand, the paucity of similar publications because, as expressed in the introduction, deductive methodology and studies concerning how knowledge is generated have difficulty in finding spaces in high-impact journals, especially in Health Sciences; in addition, the methodology or procedure presented is atypical and is founded on previous works, which can hinder follow-up and lead to a kind of concatenation that reflects more of a decade of model generation and theoretical and clinical testing. Thus, the limitations of the models and the DCM utilised appear in detail in their corresponding Thesis and articles.16–19,21–25 It is worth pointing out certain limitations, such as the fact that the ontological model includes time (the person throughout their lives) but is still analysing how to represent and manage this factor computationally, that the vulnerability model arises individually, but its validity is currently being tested for families, or that the triangulation establishes diagnostic mappings, but does not delve into how they are related to each other. There are other limitations that have been identified from the deductive to advance in the understanding of care on the basis of studying it in clinical situations.
In the future, research based on this DCM and on the models generated from it will make it possible to delve deeper into the limitations and, in parallel, to progress in knowledge related to care, both at the conceptual level of the discipline of nursing and at the level of computational management. This is a necessary challenge to face future social demands which, in line with the Sustainable Development Goals for university education, call for “new paradigms and approaches that go beyond the traditional disciplinary ones.”30
In terms of impact, the conceptual bases, inferences, limitations, and impact of these models are reflected in the corresponding doctoral theses and scientific publications. Additionally, an interdepartmental Master's degree with an emphasis on Informatics Nursing used and taught the DCM and the models presented, and is currently the basis for other lines of research.31
In conclusion, this research presents a formal structure of deductive methodology in the field of care with an interdisciplinary orientation for Health Sciences and application in knowledge management. A DCM that leads to work with certainties, evidence, and consistency that does not depend on the number of cases or inductive method applied, but recognises the path travelled by the theoretical and clinical predecessors to create an ontological model from which to break down and explore each element and relationship in greater depth. An ontology that serves to value care as a science and its social value in health outcomes.
FundingThis research has received no specific support from public sector agencies, the commercial sector, or non-profit organisations.
The authors would like to thank all the people who constituted the population samples and expert panels of the various studies referred to in this manuscript for their participation, as well as the institutions that endorse the path followed in the research concerning deductive care: University of Alcala, Madrid Official College of Nursing (CODEM, for its acronym in Spanish), Eastern Assistance Directorate of the Madrid Primary Care Management (SERMAS, for its acronym in Spanish), University of Cartagena de Indias (Colombia), and the International Network of Nursing Computer Science (RIEI, for its acronym in Spanish).
Please cite this article as: Santamaría-García JM, González-Aguña A, Fernández-Batalla M, Herrero-Jaén S, Jiménez-Rodríguez ML, González-Sotos LA. Metodología Deductiva del Cuidado: descripción y prueba de los modos de investigación acerca del cuidado. Enferm Clin. 2024. https://doi.org/10.1016/j.enfcli.2023.10.004
