





Phyllodes tumors are rare fibroepithelial lesions, with an incidence of 2.1 cases per million. They represent 0.2–2% of all breast tumors. The breast tumor department treats the largest number of patients per year at the Oncology Hospital, National Medical Center Siglo XXI, Mexican Social Security Institute, representing 17.4% of all patients treated in this centre.
Material and methodsRetrospective, descriptive study. We assessed clinical and pathological characteristics, recurrences and overall survival at 5 years in patients with phyllodes tumor of the breast treated at the Oncology Hospital, Siglo XXI National Medical Center, from January 2000 to December 2017.
ResultsThirty-two patients were included in the analysis. Mean age was 43.5 years, presentation was in the right breast in 66% of the patients and pain was present in 19%. 66% presented in the right breast, presented pain 19%. A total of 41% were benign phyllodes tumors, 41% were borderline and 18% malignant. In all, 18% of the cases were treated with wide resection, 65% with simple total mastectomy and 15% with modified radical mastectomy. Recurrence at 5 years was observed in 12%. Overall survival at 5 years was 94%, 100% for patients with benign histology, 100% for patients with borderline histology, and 66% for those with malignant histology (p=0.09).
ConclusionsIn our population, phyllodes tumors show a tendency towards size greater than 5cm, which is reflected in the greater number of mastectomies in contrast to other reports.
Los tumores phyllodes son lesiones fibroepiteliales raras, con una incidencia de 2,1 casos por millón, representando del 0,2 al 2% de todos los tumores de mama. El departamento de tumores de mama del Hospital de Oncología, Centro Médico Nacional Siglo XXI, Instituto Mexicano del Seguro Social, ocupa el primer lugar en la atención, por el número de pacientes al año, lo que representa el 17,4% de todos los pacientes tratados en este centro.
Material y métodosEstudio retrospectivo, descriptivo. Se analizaron las características clínico-patológicas, la recurrencia y la supervivencia general a los 5 años en pacientes con tumor phyllodes de la mama, tratados en el Hospital de Oncología, Centro Médico Nacional Siglo XXI, desde enero de 2000 hasta diciembre de 2017.
ResultadosIncluimos 32 pacientes. La edad media fue 43,5 años. El 66% se localizó en la mama derecha y el 19% presentó dolor. El 41% correspondió a tumor phyllodes benigno, 41% límítrofe y el 18% maligno. El 18% se trató con resección amplia, 65% con mastectomía total simple y 15% con mastectomía radical modificada. La recurrencia a 5 años se observó en el 12%. La supervivencia global a 5 años fue del 94%; para la histología benigna del 100%, limítrofe 100% y maligna 66% (p = 0,09).
ConclusionesEn nuestra población el tumor phyllodes presentó una tendencia hacia un tamaño mayor a 5 cm, lo cual se refleja en el mayor número de mastectomías que contrasta con otros estudios.
Phyllodes tumors are rare fibroepithelial lesions, with an incidence of 2.1 cases per million, representing 0.2–2% of all tumors of the breast.1–3 They primarily occur in young women, often presenting with lesions larger than 3cm, predominantly in the left breast.4–8 Bilateral tumors are infrequent, representing 3.5% of all phyllodes tumors.9
Among phyllodes variants, benign tumors are the most frequent, followed by borderline and malignant.4,5,7 Most lesions are treated with wide resection; however, mastectomy is performed in a small number of cases.5,7,9 Malignant phyllodes tumors have a higher frequency of recurrence, with a lower 5-year survival rate.4,5,7,9
The breast tumors’ department provides attention to the largest number of patients at the Oncology Hospital, National Medical Center Siglo XXI, Mexican Social Security Institute. Overall, it they represent about 17.4% of all patients treated at this center.10
The main objective of our study is to describe the clinicopathological characteristics, recurrence and overall survival at 5 years in patients with phyllodes tumor in the breast treated at the Oncology Hospital, National Medical Center Siglo XXI, Mexican Social Security Institute, from January 2000 to December 2017.
Materials and methodsWe describe a retrospective cohort comprised of all patients diagnosed with phyllodes tumor, treated at the Oncology Hospital, National Medical Center Siglo XXI, Mexican Social Security Institute, from January 2000 to December 2017.
The variables studied were the site of presentation, the duration of symptoms and signs before diagnosis, (pain, fixed skin, nipple retraction), lymph nodes, metastasis, surgical treatment and surgical margins according to histology (benign, borderline, malignant), recurrence and overall survival. The variables were analyzed, using the SPSS 25 system through descriptive statistics. The Kaplan Meier curves and the log rang were used. Values of p less than 0.5, were considered significant.
All patients diagnosed with phyllodes tumor in breast treated in the unit were included, excluding patients with incomplete dossier, as well as those with a follow-up period shorter than the objective of the study.
ResultsA total of 42 patients were identified. Ten patients were excluded due to incomplete information or missing clinical files. Data on the remaining 32 patients was analyzed.
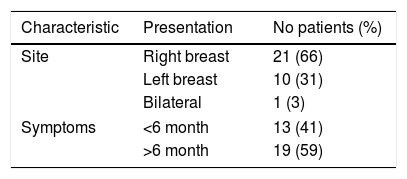
All patients were female. Mean age was 43.5 years (range 18–64). Clinical presentation patterns are described in Table 1.
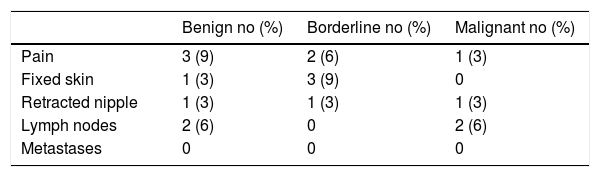
Prior to diagnosis, 19% of patients described pain, 12% fixed skin, 9% a retracted nipple, 12% palpable lumph nodes. No patients had metastases at presentation (Table 2).
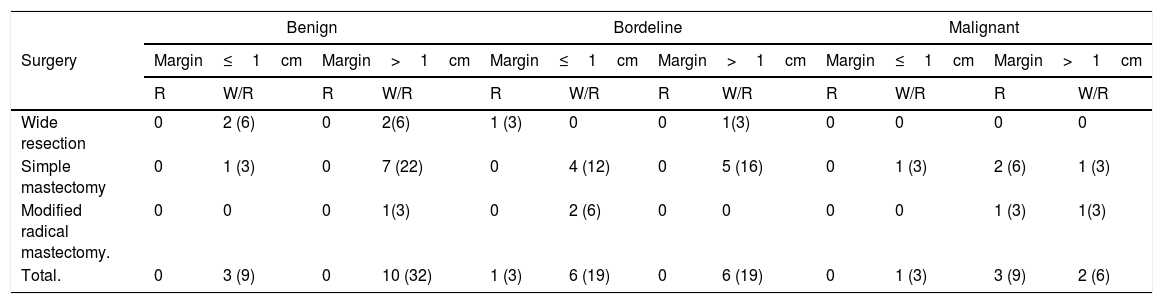
Histopathological variants were 13 benign, (41%), 13 borderline (41%), and 6 malignant tumors (18%). Surgical treatment according to histology as well as tumor dimensions are presented in Table 3.
Adjuvant radiotherapy was administered in 6 patients (18%), 5 (15%) with malignant and 1 (3%) with borderline tumors. Two patients (6%) received adjuvant chemotherapy.
Recurrence was observed in 4 patients (12%). Three patients (9%) with malignant phyllodes tumors developed recurrence, at 13, 36 and 40 months. Of these, one developed local recurrence, one presented with hepatic metastases, and one developed axillary and abdominal wall disease. One patient (3%) with borderline variant developed local recurrence 8 months after surgery. All recurrences were treated with surgery. Patients with malignant variant also underwent, chemotherapy. One patient did not accept treatment (Table 4). Two recurrent patients (6%) died of disease.
Postoperative margins according to treatment.
| Benign | Bordeline | Malignant | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Surgery | Margin≤1cm | Margin>1cm | Margin≤1cm | Margin>1cm | Margin≤1cm | Margin>1cm | ||||||
| R | W/R | R | W/R | R | W/R | R | W/R | R | W/R | R | W/R | |
| Wide resection | 0 | 2 (6) | 0 | 2(6) | 1 (3) | 0 | 0 | 1(3) | 0 | 0 | 0 | 0 |
| Simple mastectomy | 0 | 1 (3) | 0 | 7 (22) | 0 | 4 (12) | 0 | 5 (16) | 0 | 1 (3) | 2 (6) | 1 (3) |
| Modified radical mastectomy. | 0 | 0 | 0 | 1(3) | 0 | 2 (6) | 0 | 0 | 0 | 0 | 1 (3) | 1(3) |
| Total. | 0 | 3 (9) | 0 | 10 (32) | 1 (3) | 6 (19) | 0 | 6 (19) | 0 | 1 (3) | 3 (9) | 2 (6) |
R, recurrence; W/R, without recurrence.
Disease-free survival at 5 years was 87% (100%, 92% and 50% in benign, borderline and malignant variants, respectively (p=0.08). Overall survival at 5 years was 94% (100%, 100% and 66% for benign, borderline and malignant variants, respectively (p=0.09).
DiscussionSimilar to reported by Karim and Ruvalcaba, the mean age of presentation in our cohort is 43.5 years.4,5 A majority of patients presented with large tumors that were asymptomatic. In our cohort, the majority of patients (66%) had right breast disease, lower than reported by Jang and Tse who observed a higher frequency in the left breast (up to 53.7%).7,8 Bilateral presentation is a rare reporting, we observed an incidence of 3%, similar to reported by Barrio et al.9
Regarding histopathological variants frequencies, benign phyllodes tumors are reported from 50 to 72.3%, borderline in 16.2 to 35% and malignant 11.4 to 24.3% of cases. In our cohort, we observed 41% of benign and borderline tumors and 18% of malignant tumors.4,5,7,11 According to various reports, the benign tumor size averages 4.3cm, borderline tumors 5.8cm, and malignant tumors 6.8cm. In our study, we observed that benign tumors averaged more than 5cm at presentation, whereas borderline tumors were larger than 10cm. In malignant variants we observed tumors smaller than 5cm similar to previous reports.5,8 Barrio et al., in their analyses found that tumor size larger than 3cm was associated with malignant histology, however we did not find this trend in our population.9,12
With respect to treatment, 69.8–90.2% of phyllodes tumors are reported to be treated with wide resection alone and 9.8–30.1% with mastectomy. In our institution, 65% of the cases were treated with simple total mastectomy and 15% with modified radical mastectomy, whereas wide resection was performed in 18% of the cases. According various reports, mastectomy is carried out in tumors with an average tumor size of 8.8–14.7cm. In our population patients presented a size larger than 5cm in benign tumors, larger than 10cm in the borderline, while most malignant tumors were smaller than 5cm, which explains the greater frequency of mastectomy compared to the literature.4–7,9,13 In addition, the Oncology Hospital is a third level referral center, which could account for the difference in frequency and type of procedures.
For benign variants, tumor-free margins of 1mm have been accepted. For borderline and malignant histologies, a margin of 1cm is recommended. Jang et al. reported margins greater than 1cm in 3.0%, we obtained 34% margins less than 1cm and 66% greater than 1cm.2,5,7,14 Barrio reported an association between tumor size greater than 3cm with positive margin. We found a similar trend in our study, particularly in tumors with borderline histology.9
Regarding histopathologic variants, benign tumor recurrence develops in up to 14.6, borderline in 21.4% and malignant in 25% of cases. We observed a recurrence at 5 years in a 12%. In our cohort malignant variants showed a greater propensity to recurrence compared to benign and borderline variants. Regarding the histopathological variant of the recurrence, it has been reported that the recurrence is of the malignant variant up to 75% of recurrences as malignant and 16% are benign recurrent. In our cohort, 100% of malignant resected tumors, recurred as malignant.5,7,9
In patients treated with mastectomy, a lower tendency to local recurrence is reported when compared to those managed with conservative surgery, similar to our study.9
We observed a frequency of 3% of patients with distant recurrence in malignant histology, Barrio et al. described 1.7% of distant metastases. Metastases are found in up to 4% of patients with malignan tumors, with an average presentation of 1.9 years after initial diagnosis the most frequent sites are lung (91%), pleura (67%) and bones (44%). After the diagnosis of metastases, average survival time is around 4 months.7,9,15
Adjuvant radiotherapy was administered to 18% of the patients in our cohort. Radiotherapy has been reported to reduce the local recurrences of borderline or malignant phyllodes tumors after breast-conserving surgery, but without an effect on overall or disease-free survival.5,16
In our cohort, 6% of patients received chemotherapy. Adjuvant chemotherapy has been shown to have little effect on local recurrence rates, without affecting patient survival.17,18
In conclusion we report our experience in the management of phyllodes tumors of the breast. The phyllodes tumor in our population presents a size greater than 5cm, which is reflected in the greater number of mastectomies in contrast to other reports.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Conflict of interestThe authors declare no conflict of interests.

