




Diabetes mellitus is presently considered one of the most frequent diseases, therefore, it is important to know the most relevant alterations in the mouth caused by it. Diabetic patients are subjects afflicted with general health changes, with early or late complications characteristic of their systemic circumstances. With respect to local behaviour of the disease, it is possible to encounter patients with poor oral hygiene, caries, periodontal disease, infections such as candidiasis, herpes and canker sores, tendency to postsurgical bleeding, and poor healing response among other infectious or inflammatory diseases. Therefore, changes in conventional dental therapy modes are needed, as well as study of restrictions and considerations of dental treatment of these patients due to their inherent complications. The aim of the present research project was to study every oral/dental complications with different signs and symptoms exhibited by diabetic patients, as well as to propose a manual of dental procedures to undertake treatment. Consultation methodology was implemented by means of a survey conducted on 100 patients from the Diabetics Club of the «Dr. Efrén Jurado López» Day Hospital (Social Security) and the number 10 Dispensary of the Public Health Ministry. Both institutions were located in Guayaquil. Participating subjects were presented with a questionnaire in order to determine the knowledge they possessed on repercussions the disease might exert on their oral health, within the frame of our basic health zone, as well as risks encountered when receiving dental care in a state of uncontrolled disease. Likewise, surveys will be used with dentists in order to ascertain whether they apply care protocol for diabetic patients, since they are considered high-risk patients. With expected results, a dental treatment manual will be designed in order to improve oral and dental treatment for diabetic patients and concomitant diseases, so as to improve patient's quality of life.
La diabetes mellitus es considerada, hoy en día, como una de las enfermedades crónicas más frecuentes; por ello, es importante conocer cuáles son sus alteraciones más relevantes a nivel bucal. El paciente diabético representa a una persona con cambios generales de salud, con complicaciones tempranas o tardías propias de su estado sistémico, con referencia a su conducta local, es posible encontrar pacientes con pobre higiene bucal, caries, enfermedad periodontal, infecciones tales como: candidiasis, herpes, y aftas, tendencia al sangrado postquirúrgico y pobre respuesta cicatrizal, entre otras afecciones infecciosas o inflamatorias. Por lo tanto obliga a implementar cambios de modalidad terapéutica dental convencional, así como observar restricciones y consideraciones del manejo odontológico de estos individuos por las complicaciones que conlleva. En esta investigación se plantea estudiar cada una de las complicaciones bucodentales con los distintos signos y síntomas que presentan los pacientes diabéticos, con la propuesta de un manual de procedimientos odontológicos para el manejo de las mismas. La metodología es de consulta mediante encuestas a 100 pacientes del Club de Diabéticos del Hospital del Día «Dr. Efrén Jurado López» perteneciente al Seguro Social y el Dispensario N° 10 del Ministerio de Salud Pública, ambos ubicados en Guayaquil a los cuales se les aplicará un cuestionario de preguntas con la finalidad de determinar el conocimiento que tienen los mismos, en el ámbito de nuestra zona básica de salud, referente a la repercusión de la enfermedad en la salud bucodental, y el riesgo que supone someterse a la atención dental, cuando la misma no está controlada. De igual forma se aplicarán las encuestas a odontólogos para saber si aplican el protocolo de atención para pacientes diabéticos debido a que son de alto riesgo. Con los resultados esperados se diseñará un manual de atención odontológica para mejorar los tratamientos bucos orales al paciente diabético y sus enfermedades concomitantes que conlleven a mejorar su calidad de vida.
Diabetes mellitus (DM) is a non infectious disease caused by absolute or relative insulin insufficiency; as such it represents a disease that,1 although not directly treated by the dentist must be known to him in all its inherent factors. Diabetes mellitus is one of the most prevalent diseases in our country and in the world; it affects 8% of all Ecuadorians, causing severe, sometimes disabling complications. Diabetes mellitus is considered a public health issue, due to the high mortality rate exhibited by afflicted patients. It is of chronic evolution and inevitable complication, with irreversible lesions of organs vital to life, it causes high mortality rates and affects patient's average survival rates. Diabetes can be found in two types: type I is insulin-dependent and more frequently found in young patients, type II is non-insulin dependent, it is a chronic disease characterized by exhibiting high glucose levels in the blood, cell resistance to insulin action or by a deficient insulin secretion. DM2 is more common than DM1 and represents 85 to 90% of all diagnosed cases.2 It is related to risk factors that can be modified by the subject, such as obesity or overweight, physical inactivity, poor oral hygiene habits as well as low nutritional value and hypercaloric feeding habits.3
Within diabetes most relevant oral and dental alterations we find signs such as unexplained xerostomy, intense or chronic fungus-related oral candidiasis, burning sensation in the tongue, extensive caries, multiple and recurrent abscesses, gingivitis, rapid progressing periodontitis, canker sores, mean rhomboidal glossitis, increase of salivary glands, persistent oral ulcers, lichen planus, dry alveolitis after extraction, delayed post extraction or surgery healing.4
Along the course of history it has been suggested that certain clinical manifestations are more frequent in diabetic patients, nevertheless, results obtained in different studies are contradictory.5 Presence of these oral manifestations can, in some cases hinder one of the most important proposed achievements which is improving quality of life. This is due to the fact that oral and dental alterations can entail oral pain and/or discomfort, preventing suitable feeding; furthermore they can worsen the diagnosis of the main disease since they frequently alter, reverberate and aggravate some processes affecting certain organs.6 Conversely, knowledge of these manifestations can alert the dentist on the existence of a non-diagnosed diabetic patient, and thus help him to achieve suitable diagnosis and oral treatment plan, without fearing unexpected complications.7
Once the disease has been identified (based on questionnaire, signs, symptoms observation and a blood glucose test) dentists must refer patients to a physician to be evaluated.8 In the present institution, classification is made according to whether it be type I (insulin dependent) or type II (non insulin dependent).9 Type I diabetes mellitus is a chronic, autoimmune entity associated to the selective destruction of beta cells in the Langerhans islets, patients thus afflicted require insulin in order to survive. Type II diabetes mellitus, frequently associated to obesity, is the most common cause for hypoglycaemia in adults, with resistance to ketoacidosis and does not require insulin administration for survival, although it could be administered in order to better control blood glucose. Gestational diabetes is characterized by glucose intolerance during pregnancy.10
The World Health Organization (WHO) estimates there are over 220 million diabetic subjects in the world. Almost 80% of all deaths caused by this disease occur in countries with low or middle income. In 2000, there were already 165 million people afflicted with diabetes, 239 million were predicted for 2010 and 300 million for 2025.11
Out of the 165 million diabetic subjects, 35 million lived in the American Continent, out of these, 19 million resided in Latin America and the Caribbean. Projections indicate that in 2025 this number will increase to 64 million, out of which 62% will live in Latin America and the Caribbean, representing approximately 40 million. Estimated data of diabetes in adult population in Central America vary from 3 to 6%, Nicaragua and Honduras are the countries with lesser type II diabetes prevalence.12
In Ecuador, there are 500,000 diabetic subjects. Out of these, in 2010, 92,629 were diagnosed with type II diabetes, nevertheless, only some 100,000 receive proper treatment. It must be borne in mind that these figures are much higher, since about half of the subjects afflicted with the disease do not know it. To these, patients suffering type I diabetes must be added, and this total figure is equally unknown. Moreover, prevalence of diabetes mellitus type II is 4.1 to 5%. Frequency per year is about 115.19 cases per 100,000 inhabitants.
Ecuador's Public Health Ministry (PHM) informs that In 2010 92,691 cases of diabetes were diagnosed at national level, but in the last four years, increase of affected subjects has reached 403% (74,285 new cases).
According to the Ecuatorian Diabetes Federation (Fediabetes,) out of the total 14 million Ecuatorian population, about 5% of subjects older than 18 years in small cities, and 7% in Quito suffer diabetes. By 2030 diabetes could be the seventh cause of death in the country (Society 2012).
Due to the scarce information presently existing on diabetes mellitus applied to the field of dentistry, the present research work focuses on the interest of, in a simple manner, gathering, analysing and applying norms and special care which will be thoroughly described, so that dentists will have a chance to be alert, to know and apply resources available13 to them to suitably treat these complex patients. Thus, extensive study of this disease is compulsory, applying it to different fields of health sciences, among which dentistry is but one. Therefore, thorough knowledge of the subject is imperative, so as to apply correct strategies to the handling of these patients. Results obtained in the present study will be notified to Health and University Authorities so they can implement concrete and pertinent measures in order to benefit patients afflicted with diabetes mellitus.
MATERIAL AND METHODSThe present research was conducted in the «Dr. Efrén Jurado López» Day Hospital Attached to Social Security Services of Guayaquil, in the time span August 2013 to March 2014. Total patients were 100, and the sample was composed of 60 patients. The present study was observational, descriptive and cross-sectioned. All patients selected for the study were duly informed so as to obtain from them verbal agreement to become part of the study. Data were obtained of diabetic patients belonging to clubs of the aforementioned Health Institutions. Moreover, before submitting the questionnaire, a motivation and information lecture was offered on the complications represented by diabetes in the mouth, as well as the motives of the research. Patients with type I diabetes (insulin dependent) and type II diabetes (non-insulin dependent) were included. Non diabetic patients were excluded from the study.
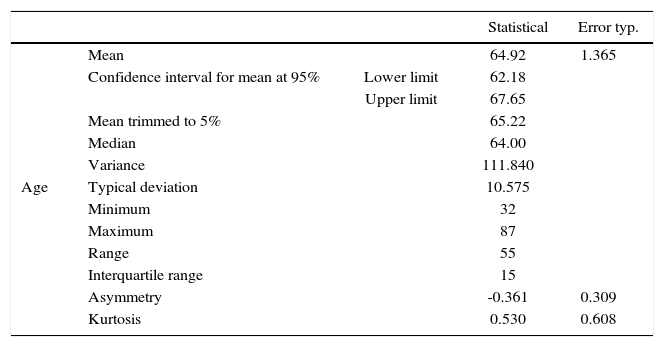
Results analysisTable I shows that mean age is 65.22, this means patients are mostly elderly citizens.
Description of the age variable.
| Statistical | Error typ. | |||
|---|---|---|---|---|
| Age | Mean | 64.92 | 1.365 | |
| Confidence interval for mean at 95% | Lower limit | 62.18 | ||
| Upper limit | 67.65 | |||
| Mean trimmed to 5% | 65.22 | |||
| Median | 64.00 | |||
| Variance | 111.840 | |||
| Typical deviation | 10.575 | |||
| Minimum | 32 | |||
| Maximum | 87 | |||
| Range | 55 | |||
| Interquartile range | 15 | |||
| Asymmetry | -0.361 | 0.309 | ||
| Kurtosis | 0.530 | 0.608 |
Source: OWN.
Typical deviation is 10.57, this expresses that approximately 68% of all values are found among [54.65; 75.79].
Values of kurtosis and asymmetry are close to zero, therefore it can be inferred that distribution is close to normal. This was corroborated with the Shapiro Will test, in where probability associated to stadigraph was p = 0.335, that is to say the null hypothesis which expresses that distribution of the age variable is normal was accepted.
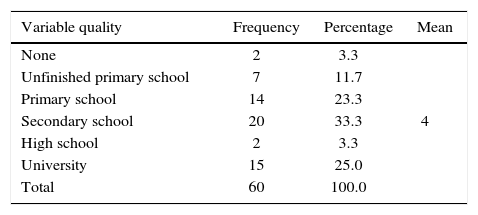
Table IIandfigure 1 show that the median of the education variable is 4, that is to say, basic secondary school, and that the rest of the qualities are distributed in a proportional manner with a prolonged extreme to high values since the quality University has high score.

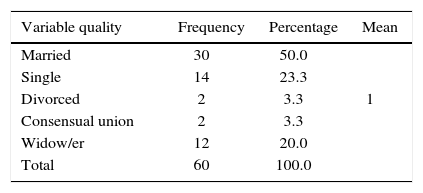
Table III shows that «married» is the variable mode of «marital status», this means that most patients (50%) are married, followed by (23.3%) single and (20%) widow/widower.
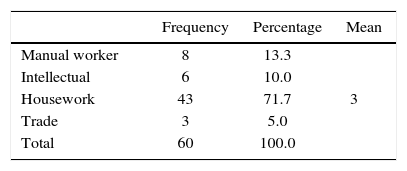
Table IV shows that mode is 3, that is to say that the most repeated quality is housework (71.7%), followed by manual workers and intellectuals (13.3 and 10.0% respectively).
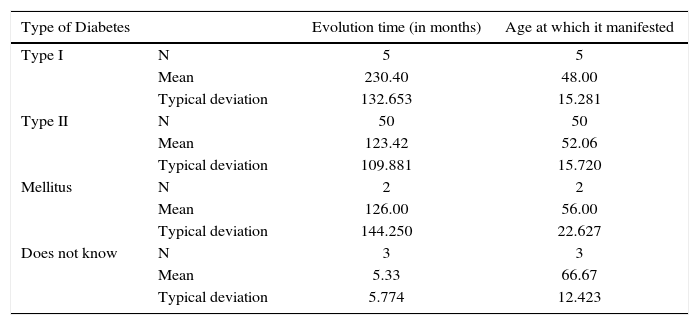
In table V we see predominance of type II diabetes, with 50 patients (out of all patients surveyed) representing 83.3%. Patients of this majority group experienced onset of the disease at 52.06 years of age, with typical deviation of 15.7 years, that is to say, onset was observed at 34-36 and 67-68 years approximately. Evolution time was 230.40 months, that is to say that patients have been afflicted with the disease for 19.2 years.
Patient distribution according to diabetes type, evolution (in months) and age at which diabetes was manifested.
| Type of Diabetes | Evolution time (in months) | Age at which it manifested | |
|---|---|---|---|
| Type I | N | 5 | 5 |
| Mean | 230.40 | 48.00 | |
| Typical deviation | 132.653 | 15.281 | |
| Type II | N | 50 | 50 |
| Mean | 123.42 | 52.06 | |
| Typical deviation | 109.881 | 15.720 | |
| Mellitus | N | 2 | 2 |
| Mean | 126.00 | 56.00 | |
| Typical deviation | 144.250 | 22.627 | |
| Does not know | N | 3 | 3 |
| Mean | 5.33 | 66.67 | |
| Typical deviation | 5.774 | 12.423 | |
Source: OWN.
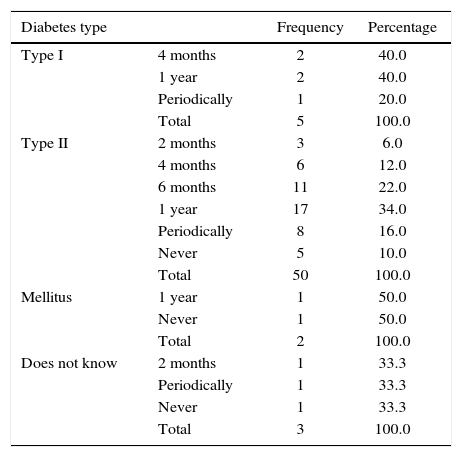
Table VI shows that within type II diabetes patients, the most common behaviour is to attend a dental office every six months (22.0%). Type I patients attend dental offices every 4 months and once a year.
Behavior of frequency of visit to the dentist according to diabetes type.
| Diabetes type | Frequency | Percentage | |
|---|---|---|---|
| Type I | 4 months | 2 | 40.0 |
| 1 year | 2 | 40.0 | |
| Periodically | 1 | 20.0 | |
| Total | 5 | 100.0 | |
| Type II | 2 months | 3 | 6.0 |
| 4 months | 6 | 12.0 | |
| 6 months | 11 | 22.0 | |
| 1 year | 17 | 34.0 | |
| Periodically | 8 | 16.0 | |
| Never | 5 | 10.0 | |
| Total | 50 | 100.0 | |
| Mellitus | 1 year | 1 | 50.0 |
| Never | 1 | 50.0 | |
| Total | 2 | 100.0 | |
| Does not know | 2 months | 1 | 33.3 |
| Periodically | 1 | 33.3 | |
| Never | 1 | 33.3 | |
| Total | 3 | 100.0 | |
Source: OWN.
Table VII shows that 53.3 of all patients consider that their health would be improved if they did not suffer diabetes, 38.3% consider this opinion as a possibility, 65.0% of patients were not informed by the physician on diabetes complications that might arise in the mouth, whereas 26.7% did receive that information from their treating physician.
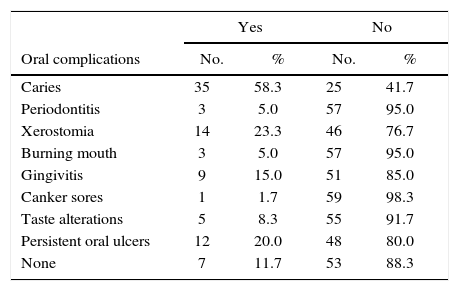
Table VIII shows that caries is the most frequent complication found in diabetic patients (58.3%) followed by xerostomia (23.3%). Canker sores were the least frequent complication (1.7%).
Oral complications of diabetes patients.
| Yes | No | |||
|---|---|---|---|---|
| Oral complications | No. | % | No. | % |
| Caries | 35 | 58.3 | 25 | 41.7 |
| Periodontitis | 3 | 5.0 | 57 | 95.0 |
| Xerostomia | 14 | 23.3 | 46 | 76.7 |
| Burning mouth | 3 | 5.0 | 57 | 95.0 |
| Gingivitis | 9 | 15.0 | 51 | 85.0 |
| Canker sores | 1 | 1.7 | 59 | 98.3 |
| Taste alterations | 5 | 8.3 | 55 | 91.7 |
| Persistent oral ulcers | 12 | 20.0 | 48 | 80.0 |
| None | 7 | 11.7 | 53 | 88.3 |
Source: OWN.
When conducting χ2 test among all complications with the regrouped variable of having type II diabetes or other, significant differences could not be found in any of the cases. This condition is necessary in order to be able to develop a logistic regression, this propitiated that no variable entered in the model and must be associated to the fact that only 10 patients, 16.7% are suffering from a diabetes other than type I.
CONCLUSIONSPopulation of Latin America and the Caribbean exhibit the highest percentages of diabetes in the world. This has been confirmed by WHO and Panamerican Health Organization in 2012.
WHO informed that presently there are over 360 million diabetic subjects in the world, and estimates this figure will double by 2030.
In Ecuador there are 200,000 diabetic subjects, about 40,000 (20%) of them have been diagnosed and are receiving treatment (2013).
Diabetes type II is present in 1 to 5% of cases.
Diabetes incidence, as such, is not responsible for any specific oral disease, it has been shown that oral complications are related to the patients’ ability to control sugar levels in the blood (glycemic control) and their general health circumstances.
According to INEC (National Institute of Statistics and Census) the following provinces exhibit higher incidence rates: Santa Elena, Cañar, Manabí, El Oro, los Ríos, Guayas and Azuai, representing 80.6% of all subjects afflicted by diabetes in Ecuador.
Diabetes is a chronic disease that, left undiagnosed and untreated, might cause heart disease, blindness, renal failure, infections in limbs due to neuropathy or even the patient's demise.
Diabetes is a disease that appears when the body does not suitably use glucose to transform it into energy. Its cause can be inability of the pancreas to produce insulin, called type I diabetes, or the inability of using it in the appropriate manner, called type II diabetes.
There is no National Health Policy which might allow diabetic patients as well as the rest of the population with some disease to avoid disease aggravation, by the simple fact of unawareness or ignorance of suitable treatments.
There is an obvious need for changes in prevention strategies and disease screening.
Policies implemented by the Ecuador Public Health Ministry are practically nil.
In educational programs, theoretical-practical content should always try to achieve that diabetic patients learn concepts, attitudes and oral health practice which will improve their quality of life.
RecommendationsFostering a state supported «National Program of Health Education» into one single system, for all Ecuatorians, which might signify improvement in treatment to subjects suffering this catastrophic type disease, especially patients with type II diabetes mellitus, who will have the opportunity of living without the devastating consequences of the disease's chronic complications, since only an empowered patient, educated and convinced of the benefits of self-care, will generate personal, social and financial benefits.
Developing schemes and strategy changes to assess the impact of diabetes prevention and control programs.
Conducting an education and information campaign for citizens on specific signs and symptoms of diabetes and derived oral complications, in order to timely detect the 160,000 diabetics who are as yet undiagnosed.
Protection of the mouth could generate health of the whole body. The mouth is one of the body's areas with greater bacteria concentration, 700 types of bacteria can be identified in that environment.
Involve all health sectors in order to plan prevention, protection, promotion and health improvement strategies at this life stage of the human being.
Establish health treatment programs for elderly patients in all facilities of public and private sectors.
Create public policies to guarantee access to diabetes prevention for women, who are the most affected according to conducted research.
To become aware of the importance of preserving suitable oral health in order to prevent disease which could affect other systems and functions of our body.
To regularly attend the dental office, no less than twice a year, to control onset of caries and infections such as candidiasis, and always inform the patient about diabetes when he is afflicted by it.
Suitably treat oral infections since solving them will help the diabetic patient to control glucose levels.
Frequently control glucose levels in the blood.
Patients should devote a few minutes every day to regularly inspect their mouth so as to identify any existing problems. The patient might notice bleeding gums upon brushing or using dental floss.
To recommend personal care based on true information, giving the patient personal responsibility, which represents an effective strategy to delay or decrease development of oral complications.
DDS, Health Management Degree, University of Guayaquil, Pilot Faculty of Dentistry. Graduate Degree from Catholic University of Santiago, Guayaquil.
This article can be read in its full version in the following page: http://www.medigraphic.com/facultadodontologiaunam
Graduate from Pilot Faculty of Dentistry, Guayaquil University, Master's Degree University of Guayaquil, Graduate School, Pilot Faculty of Dentistry.
University of Guayaquil, Pilot Faculty of Dentistry, Graduate School, University of Guayaquil, Orthodontics Specialist.