




Fungal infections are emerging as an important cause of human disease, especially among hospitalized patients with serious underlying disease and several risk factors.
AimsTo evaluate epidemiological and clinical characteristics of patients with nosocomial candidiasis in university hospitals in Cuiabá – MT, Brazil.
MethodsA descriptive study of 91 patients admitted to university hospitals in Cuiabá – MT, with clinical and laboratory diagnosis of nosocomial candidiasis, over a 20-month period.
ResultsA rate for nosocomial infections by Candida spp. of 5 per 1000 admissions, proportional mortality of 14.4% and lethality of 53.8% were determined. The patient age ranged from 29 days to 82 years-old, among which, 74.7% were adults and 25.3% children. The intensive care units contributed with the highest number of cases of infection by Candida spp. (69.2%). The most important underlying disease was gastrointestinal tract disease (11%). Prematurity and low birth weight were the most important risk factors among newborns. The use of antibiotics, invasive procedures, H2 blockers, multiple blood transfusions and stay length of ≥21 days were the most frequent risk factors among adults. Candida albicans was the most common species in all cases.
ConclusionsIn this study, C. albicans was the most frequently detected species in candidiasis and risk factors increased the susceptibility of hospitalized patients to acquiring a nosocomial infection by Candida spp.
Las micosis están emergiendo como una importante causa de enfermedad en el ser humano, en especial entre pacientes hospitalizados con enfermedades subyacentes graves y otros factores de riesgo.
ObjetivosExaminar las características epidemiológicas y clínicas de los pacientes con candidiasis nosocomial en hospitales universitarios de Cuiabá, Mato Grosso, Brasil.
MétodosDurante un período de 20 meses, se realizó un estudio descriptivo de 91 pacientes ingresados en hospitales universitarios de Cuiabá, Mato Grosso, con un diagnóstico clínico y de laboratorio de candidiasis nosocomial.
ResultadosSe determinó una tasa de infección nosocomial por Candida de 5 por cada 1.000 ingresos; la tasa de mortalidad fue del 14,4% y la de letalidad del 53,8%. Las edades de los pacientes variaron entre 29 días y 82 años. El 74,7% de los pacientes estaban en la edad adulta y el 25,3% eran niños. Las unidades de cuidados intensivos contribuyeron con el mayor número de casos de infección por Candida (69,2%). La enfermedad subyacente más importante fue un proceso del tracto gastrointestinal (11%). La prematuridad y el bajo peso al nacer fueron los factores de riesgo más importantes entre los recién nacidos. La administración de antibióticos, los procedimientos cruentos, el uso de antagonistas H2, las múltiples transfusiones de sangre y una duración de la estancia hospitalaria ≥ 21 días fueron los factores de riesgo más frecuentes entre los adultos. C. albicans fue la especie más habitual en todos los casos.
ConclusionesEn el presente estudio, C. albicans fue la especie detectada con más frecuencia en las candidiasis y las exposiciones de riesgo aumentaron la predisposición de los pacientes hospitalizados a adquirir una infección nosocomial por Candida spp.
Fungal hospital infections emerge as an important cause of human disease, especially among immunocompromised and hospitalized patients with serious underlying disease. Of the hospitalized patients, 8% may acquire a fungal hospital infection, whose mortality is usually high (40–60%), involving costly treatment, especially in adult and neonatal intensive care units.7,20 The vast majority of fungal infections are caused by yeasts of the genus Candida (80%), being Candida albicans the most prevalent. Species identification of Candida yeasts in recent years has proved to be relevant, mainly to obtain data regarding the epidemiology of these pathogens in hospitals and to direct subsequent antifungal treatment. The increase in infections by other species of Candida yeasts should be highlighted.7,8,15 These yeasts are considered prominent pathogens in nosocomial infections, mainly because they are constituents of the microbiota of healthy individuals and are widespread in the environment.9,15,20 The objectives of this study were to evaluate the epidemiological and clinical characteristics of patients with nosocomial candidiasis in university hospitals in Cuiabá, MT, Brazil.
Patients and methodsStudy design and settingThis study was approved by an institutional review board, which granted a waiver of informed consent for anonymous data collection. A descriptive study was conducted over a 20-month period (March 2008 to November 2009), involving reviewing the medical records of 91 patients with nosocomial candidiasis admitted to university hospitals in Cuiabá. The review of the clinical information of patients’ medical records was conducted by filling out a previously established epidemiological form, developed to elucidate the possible risk factors associated with nosocomial fungal infections. All the patients included in this study were initially investigated for the presence of fungi as a cause of infection, because they showed clinical signs and symptoms compatible with nosocomial fungal infection. Thus, following laboratory confirmation, all these patients were treated with antifungals and clinically followed until remission of the infection and/or death.The clinical specimens blood and urine were more associated with nosocomial fungal infections, which is why the analysis of risk factors for candidemia and candiduria were performed in isolation.
Hospitals characteristicsUniversity Hospitals of Cuiabá, Mato Grosso (Brazil) related to the SUS (Sistema Único de Saúde, Brazilian National Health System) has a total of 253 beds. A university hospital provides medical care to cancer patients and bone marrow transplantation (BMT) and another hospital is a reference center for HIV patients. The university hospitals together have five intensive care units (2 adult, 2 neonatal and 1 coronary), medical, surgical, gynecological and obstetric and pediatric inpatient care units.
Patient assessmentPatients admitted to university hospitals in Cuiabá, State of Mato Grosso, Brazil, with clinical signs or symptoms of nosocomial candidiasis were included in the study. Collection included the following clinical specimens and sterile swabs of hospital devices consistent with the site of infection in order to perform cultures, and determine the identification of yeast species of the genus Candida: urine, blood, catheter tip, bronchoalveolar lavage, tracheal aspirate, pleural fluid, ascitic fluid, secretions of subphrenic abscess and surgical site.
Case definition of nosocomial infections by yeasts of the genus CandidaA case of nosocomial infection by Candida was considered confirmed when clinical specimens and hospital devices were in accordance with the following criteria:
- •
Positive blood culture for Candida spp. obtained after the first 72h of hospitalization or;
- •
Urine with more than one isolate and counts above 100,000CFU/mL or;
- •
Catheter tip showing 15 or more CFU/plate or;
- •
Bronchoalveolar lavage (BAL) positive for Candida and positivity for the same species in other clinical specimens;
- •
Other clinical specimens, when positive for Candida, with proven clinical diagnosis and treatment of infection at a particular site matching the clinical status presented by the patient.
Isolation of Candida yeast colonies was performed in tubes containing Sabouraud dextrose agar with chloramphenicol (Difco, USA) or Mycosel agar (Difco, USA), incubated at 27°C. The following tests were conducted for yeast identification: germinative tube, microculture in Corn-meal agar with Tween 80 (Difco, USA), CHROMagar-Candida® (Difco, USA) growth, auxanogram and zymogram subcultures.
Statistical studyThe data were tabulated and presented in tables of frequency distribution of categorical variables, and measures of central tendency and dispersion for quantitative variables. For the association between risk factors with candiduria and candidemia, the Chi square was used. It was considered significantly different when the p value was ≤0.05.
ResultsOver a 20-month period, a total of 18,258 patients were admitted to the university hospitals evaluated. The general rate of hospital infection was 11.4% (2088/18.258). Nosocomial candidiasis was confirmed in 91 patients admitted that represents a rate of nosocomial infections by Candida of 5 per 1000 admissions (91/18.258), a proportional mortality of 14.4% (49/341) and lethality equal to 53.8% (49/91). The age of patients admitted to university hospitals ranged from 29 days to 82 years-old with a mean of 37.5 years-old. The pediatric group (children younger than 1 year-old) showed a prevalence of 21 (23%). In adult patients, the greatest concentrations occurred among the age groups 45–54 years-old (17%), 55–64 years-old (11%), 65–74 years-old (12%) and 75 years-old or over (9%). Regarding patient sex, among the 91 patients studied, there was a predominance of females (n=49, 54%). The adult (41%) and neonatal intensive care units (25%) contributed to the largest number of isolates related to hospital infections by yeasts of the genus Candida.
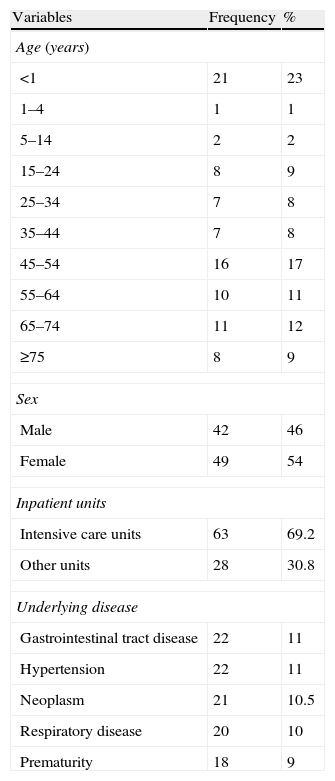
The most important underlying diseases were gastrointestinal tract disease and hypertension (n=22, 11%), and tumors (n=21, 10.5%), while the most frequently affected systems were the gastrointestinal (n=11, 44%), followed by the genitourinary and blood systems (n=20, 10%). Demographic and clinical data of patients with nosocomial candidiasis are presented in Table 1.
Demographic and clinical data of 91 patients in the university hospitals of Cuiabá, MT, 2008–2009.
| Variables | Frequency | % |
| Age (years) | ||
| <1 | 21 | 23 |
| 1–4 | 1 | 1 |
| 5–14 | 2 | 2 |
| 15–24 | 8 | 9 |
| 25–34 | 7 | 8 |
| 35–44 | 7 | 8 |
| 45–54 | 16 | 17 |
| 55–64 | 10 | 11 |
| 65–74 | 11 | 12 |
| ≥75 | 8 | 9 |
| Sex | ||
| Male | 42 | 46 |
| Female | 49 | 54 |
| Inpatient units | ||
| Intensive care units | 63 | 69.2 |
| Other units | 28 | 30.8 |
| Underlying disease | ||
| Gastrointestinal tract disease | 22 | 11 |
| Hypertension | 22 | 11 |
| Neoplasm | 21 | 10.5 |
| Respiratory disease | 20 | 10 |
| Prematurity | 18 | 9 |
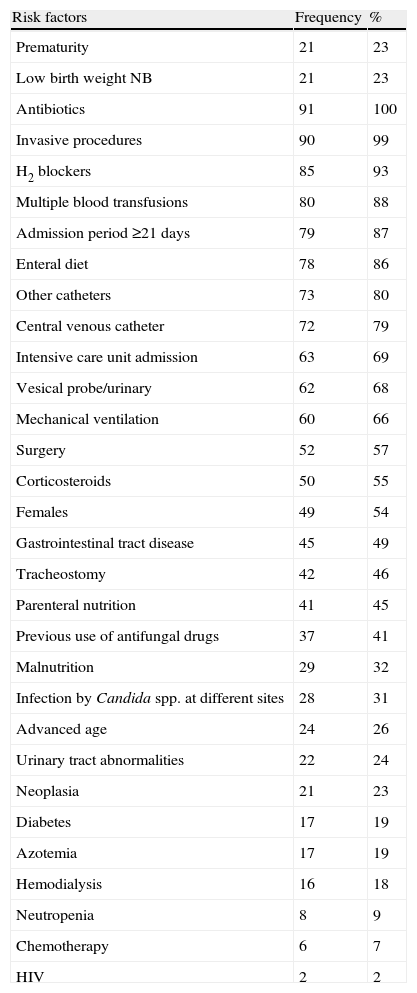
The risk factors of greatest relevance are shown in Table 2. Observation revealed that 91 (100%) patients were treated with antibiotics (specifically, penicillins associated with beta-lactamase inhibitors, carbapenems and cephalosporins; mainly third and fourth generation); 90 (99%) were submitted to some invasive procedure; 85 (93%) used H2 blockers; 80 (88%) were submitted to multiple blood transfusions and 79 (87%) were hospitalized for 21 days or more (mean of 55.8 days); 78 (86%) required enteral feeding; 41 (45%) required parenteral nutrition; and all 21 (23%) newborns were premature and had low birth weight.
Risk factors associated with patients admitted to university hospitals in Cuiabá, MT, 2008–2009.
| Risk factors | Frequency | % |
| Prematurity | 21 | 23 |
| Low birth weight NB | 21 | 23 |
| Antibiotics | 91 | 100 |
| Invasive procedures | 90 | 99 |
| H2 blockers | 85 | 93 |
| Multiple blood transfusions | 80 | 88 |
| Admission period ≥21 days | 79 | 87 |
| Enteral diet | 78 | 86 |
| Other catheters | 73 | 80 |
| Central venous catheter | 72 | 79 |
| Intensive care unit admission | 63 | 69 |
| Vesical probe/urinary | 62 | 68 |
| Mechanical ventilation | 60 | 66 |
| Surgery | 52 | 57 |
| Corticosteroids | 50 | 55 |
| Females | 49 | 54 |
| Gastrointestinal tract disease | 45 | 49 |
| Tracheostomy | 42 | 46 |
| Parenteral nutrition | 41 | 45 |
| Previous use of antifungal drugs | 37 | 41 |
| Malnutrition | 29 | 32 |
| Infection by Candida spp. at different sites | 28 | 31 |
| Advanced age | 24 | 26 |
| Urinary tract abnormalities | 22 | 24 |
| Neoplasia | 21 | 23 |
| Diabetes | 17 | 19 |
| Azotemia | 17 | 19 |
| Hemodialysis | 16 | 18 |
| Neutropenia | 8 | 9 |
| Chemotherapy | 6 | 7 |
| HIV | 2 | 2 |
Of the 110 clinical specimens (urine, blood, body fluids, secretions and bronchoalveolar lavage) and swabs from hospital devices (catheter tip) obtained from the 91 patients, the following species of yeasts of the genus Candida were identified: 43 (39.09%) were identified as Candida albicans, 36 (32.73%) as Candida tropicalis, 24 (21.82%) as Candida parapsilosis, 6 (5.45%) as Candida glabrata and 1 (0.91%) as Candida krusei. The species C. albicans was the most frequently detected in cases of candidemia and candiduria, and C. tropicalis was slightly more prevalent among the other clinical specimens evaluated, followed by C. albicans and C. parapsilosis.
A statistically significant association of H2 blockers (p≤0.05; OR 0.14; IC95% 0.01–1.31) and parenteral nutrition (p≤0.003; OR 3.65; IC95% 1.50–8.87) with candidemia was observed; whereas, candiduria showed a statistically significant association with urinary tract abnormalities (p≤0.0001; OR 26.32; IC95% 5.43–127.52), diabetes (p≤0.002; OR 9.15; IC95% 2.34–35.78) and the use of urinary catheter (p≤0.004; OR 8.10; IC95% 2.46–26.7).
DiscussionNosocomial candidiasis was present in all the units assessed in this study, following the hegemonic trend of Candida as the main agent of nosocomial fungal infections.
In the neonatal intensive care units, nosocomial fungal infection varies between 10% and 20%, with mortality rate around 60% and candidemia of 40–60%.7,12,20
In this study, a rate hospital infection by Candida of 5 per 1000 admissions was determined, as well as proportional mortality of 14.4% and lethality of 53.8%. A study involving public hospitals in São Paulo determined that the incidence of nosocomial fungal infection ranged from 2.3% to 5% per 1000 admissions, whereas others studies have reported an incidence of 2.4 per 1000 admissions for candidemia alone.1,20,21 Blumberg et al.1 and Colombo and Guimarães7 found a mortality of 40–60% among these patients, a value higher than that verified in this study.
In contrast, a lethality rate of 53.8% due to nosocomial infections by yeasts of the genus Candida must be considered relevant.
Of the 91 evaluated patients admitted to university hospitals, 21 (23%) were children younger than 1 year-old, while among adult patients, the greatest concentrations occurred among the age groups 45-54 years-old (17%), 55-64 years-old (11%), 65-74 years-old (12%), and 75 years-old or over (9%). In their study of candidemia in Campo Grande, MS, Chang et al.5 reported this infection in newborns (0-30 days-old, 20.8% of cases), followed by patients aged over 60 years-old (21.9%). Hahn et al.15 identified greater involvement of patients between the ages of 0 and 10 years-old (18.1%) and between 61 and 70 years-old (24.2%). These data corroborate series described in the literature, which show that patients of extreme ages are more susceptible and present high rates of infection (patients younger than 1 year-old, and those over fifty years-old).
Regarding patient sex, of the 91 patients studied, females (n=49, 54%) were the most susceptible. This result demonstrates the vulnerability of women to urinary tract infections, primarily due to the physiological anatomy of the female urethra (shorter) and the fact that 30% of healthy women present persistent vulvovaginal colonization by Candida spp.2,5
The underlying disease may favor the occurrence of hospital infection by affecting the immune system mechanisms. Patients with multiple preexisting conditions certainly have a greater chance of contracting infections.10,11,24 This study has shown the relevance of gastrointestinal tract diseases and hypertension, which also contributed with 22 cases (11%), followed by neoplasms (n=21, 10.5%), which most frequently affected the gastrointestinal and genitourinary system, followed by the blood; 20 (10%) patients presented respiratory diseases. França et al.12 observed that of 100 cases evaluated at the Clinics Hospital of the Federal University of Paraná (2001–2004), only 9 (9%) presented gastrointestinal tract disease, 1 (1%) presented heart disease, 25 (25%) presented neoplasms and 19 (19%) presented respiratory diseases. In a prospective study on the epidemiology of candidemia in Brazil, involving 11 medical centers in 9 major Brazilian cities, Colombo et al.8 detected 712 cases of candidemia and reported cancer as most important underlying disease, corresponding to 195 cases (27%). Of these, 75 cases (38%) affected only the blood system. The cardiac and respiratory diseases were verified in 139 and 138 cases (19%), respectively.
Several pathological, physiological or traumatic processes can facilitate the colonization and subsequent infection of the host, mainly by yeasts of the genus Candida.4,9,13,16,23 Comparing the findings concerning the risk factors found in this study to data obtained by França et al.,12 they reported that antibiotics occupied a prominent position among the risk factors evaluated, which is consistent with that obtained in this study. However in their study, the frequency of these factors were as follows: presence of central venous catheter (77%), H2 blockers (57%), total parenteral nutrition (49%), admission to a intensive care unit (41%), values that corroborate the risk factors identified in this study, but lower than those obtained in the University Hospitals of Cuiabá, MT. In northeastern Brazil, Hinrichsen et al.17 reported that the presence of central venous catheter was associated with 57% of patients in a tertiary hospital in Recife, which is lower than the value obtained in this study.
The increase in the frequency of hematogenous infections by Candida species (candidemia) has been observed particularly among patients being treated with antibiotics, H2 blockers, corticosteroids, parenteral nutrition and in patients exposed to multiple invasive procedures.6,14 A statistically significant association of the risk factors H2 blockers and parenteral nutrition were observed with candidemia in the present work. Candiduria has been significantly associated with risk factors, including urinary tract abnormalities, diabetes and the use of urinary catheter.
In Brazil, the main species causing candidemia are C. albicans, C. parapsilosis and C. tropicalis, while C. albicans is the most frequently isolated species in specimens worldwide.6–8 Considering the species distribution of yeasts of the genus Candida in the hospitals studied, predominance of C. albicans was observed, followed by C. tropicalis, C. parapsilosis, C. glabrata and C. krusei.
Regarding the episodes of candidemia, the species C. albicans was the most frequently isolated in the university hospitals of Cuiabá, MT, confirming the findings of other authors.6,12,14,18-20
The high prevalence of C. parapsilosis and C. tropicalis as etiologic agents of candidemia in South America has been recorded by other researchers.6,20 Brito et al.3 reported the association between candidemia by C. parapsilosis and the presence of central venous catheter, suggesting that the presence of central venous catheter was the main mode of acquisition of this species from an external source. Its greater frequency in children and premature infants hospitalized in intensive care units, with prevalence of 17–50% was reported by Colombo and Guimarães.7
Among the urine cultures evaluated, C. albicans was the most prevalent species (41.3%), followed by C. tropicalis (8.7%). In a study of candiduria in children (0–7 years-old), Silva et al.22 identified C. albicans as the most frequent species (56%), followed by C. tropicalis (20%), confirming the results obtained in the present study.
Regarding the distribution of the yeasts identified according to the inpatient unit in university hospital intensive care units, analysis verified that these units had a larger number of cases of hospital infection by yeasts of the genus Candida (63 cases, 69.2%) compared to all the other clinics studied. In the adult intensive care unit, C. albicans was the most frequent species identified; C. parapsilosis was prevalent in the neonatal intensive care unit and C. tropicalis in the coronary intensive care unit, performing well as a significant risk factor for developing nosocomial infections.
In a study of fungal specimens collected at public hospitals in São Paulo, Paula et al.20 verified that the yeasts isolated in most cases of candidemia and candiduria were C. albicans, C. parapsilosis and C. tropicalis.
A combination of factors likely contribute to higher rates of candidemia in Brazil, including difficulties in the implementation of an effective program for hospital infection control, the limited number of staff in healthcare, intensive care units and prevention and less aggressive practices of empirical antifungal therapy in high risk patients. However, the data presented may be underestimated, possibly due to the absence of fungal growth in vitro, or even the institution of empirical therapy without collection of clinical material for laboratory diagnosis of fungal hospital infection.
Despite these factors, in general, the data obtained in this study highlighted the importance of characterizing and specifying the species of Candida yeasts to add to current knowledge of the regional epidemiological profile and of individual hospitals. Furthermore, it was possible to perform comparisons of the data obtained, emphasizing the risk factors associated with nosocomial infections by Candida species identified in this study, with records held in different geographical regions. Several other studies have reported data for other countries and regions, including Europe and North America; however, Brazilian studies and the realities of local hospitals should be carefully evaluated and compared.
This work shows that nosocomial candidiasis is a significant source of mortality in university hospitals in Mato Grosso, Brazil, with a substantial burden of disease, mortality, associated to risk factors and likely high costs. It's important to identify those steps that can help to prevent the disease, and observe the rules established by hospital infection control committees about the appropriate use of antifungal agents after identification of yeast of the genus Candida.
Financial supportFAPEMAT − Fundação de Amparo à Pesquisa de Mato Grosso.
Conflict of interestAuthors have nothing to declare.
The authors are grateful to the entire team of the Investigation Laboratory (Mycology); Laboratory Specialized in Mycology, University General Hospital and the Mycology Laboratory, University Hospital Júlio Müller, Cor Jesus Fernandes Fontes and Mariana Caselli Anzai.

